
Abstract
Background:
Although double-leg squatting is less dynamic and places less demand on the quadriceps compared with landing tasks, the relationship between double-leg squatting biomechanics and persistent quadriceps weakness after anterior cruciate ligament reconstruction (ACLR) is unknown.
Purpose:
To clarify the relationships between asymmetries in quadriceps strength and lower limb biomechanics during double-leg squatting >1 year after ACLR.
Study Design:
Controlled laboratory study.
Methods:
A total of 26 participants (5.5 ± 3.8 years after ACLR) were enrolled. The limb symmetry index (LSI) of isokinetic quadriceps strength was used to divide participants into the high-quadriceps (HQ) group (LSI ≥90%; n = 18) and the low-quadriceps (LQ) group (LSI <90%; n = 8). The knee, hip, and ankle extension moment (relative to body weight and support moment [sum of knee, hip, and ankle moments]) and vertical ground-reaction force during double-leg squatting were analyzed using 3-dimensional motion analysis. The association of quadriceps strength and biomechanical variables was tested using 2-way analysis of variance and univariate regression analysis.
Results:
A significant group-by-limb interaction was found for the peak knee extension moment and the ratios of knee and hip extension moment to support moment (P < .001, P = .015 and P < .001, respectively). The LQ group showed a significantly smaller peak knee extension moment and knee to support moment ratio but a larger hip to support moment ratio in the involved limb than in the uninvolved limb (95% CIs: knee extension moment, −0.273 to −0.088 N·m/kg; knee to support moment ratio, −10.7% to −2.2%; hip to support moment ratio, 3.2% to 8.5%). No interlimb difference was found for the HQ group. The LSI of quadriceps strength was significantly associated with the LSI of peak knee extension moment (R 2 = 0.183), knee to support moment ratio (R 2 = 0.256), and hip to support moment ratio (R 2 = 0.233). The mean maximum isokinetic quadriceps strength and peak knee extension moment during squatting on the involved limb of the LQ group were 2.40 ± 0.39 and 0.90 ± 0.16 N·m/kg, respectively.
Conclusion:
Asymmetrical biomechanics during double-leg squatting was associated with persistent quadriceps weakness after ACLR. The LQ group had reduced knee extensor moment on the involved side during squatting despite loading at approximately half the maximum strength.
Clinical Relevance:
Quadriceps strengthening exercises, together with interventions to improve neuromuscular control, may reduce asymmetrical biomechanics during double-leg squatting.
Quadriceps weakness is a major problem after anterior cruciate ligament (ACL) reconstruction (ACLR). 1,22,33 Neuromuscular inhibition is reported to be associated with quadriceps weakness after ACLR. 16,25 A limb symmetry index (LSI) of quadriceps strength ≥90% is widely used as a criterion for return to sports after ACLR. 36 Return to sports without meeting this criterion increases the risk of rerupture or knee injury. 6,13 However, only 23% of patients meet this criterion before returning to sports. 36 Moreover, persistent quadriceps weakness has been associated with lower patient-reported outcome measures 24,37 and an increased risk of osteoarthritic changes. 2,32 Although quadriceps strength recovers over time after surgery, a recent metaregression model showed that 54.5 months may be required for quadriceps strength in the involved limb to recover to the level of the uninvolved limb. 33 Additionally, a previous study showed that strength deficits in the involved limb, compared with the uninvolved limb, can persist for >5 years after surgery. 14
Double-leg squatting is commonly used to improve quadriceps strength as well as neuromuscular control of lower limb muscles after ACLR. 34 An interlimb asymmetry in knee kinetics during double-leg squatting has been hypothesized to be associated with poor recovery of quadriceps strength after ACLR. 26,27,35 Although this exercise is mainly used in the early phase of rehabilitation, interlimb asymmetry of knee kinetics is present even after completion of a rehabilitation program. 5,26,35 Studies showed that knee extension moment in the involved limb was significantly smaller than that in the uninvolved limb during double-leg squatting. 3,26,27,30 Interlimb asymmetry in the knee extension moment was found even if there was no significant asymmetry in vertical ground-reaction forces or the support moment during double-leg squatting. 26,27 Consequently, a smaller contribution to force attenuation of the knee joint relative to the hip and ankle joints was associated with a smaller knee extension moment in the involved limb than in the uninvolved limb. 3,26,27,30 Such an asymmetrical knee extension moment has been observed not only in double-leg squatting but also in gait, running, and jump-landing. 7,15,19 Moreover, the asymmetry in knee extension moment during double-leg squatting was positively correlated with that during a jump-landing task. 21 Interlimb asymmetry in the knee extension moment during double-leg squatting is hypothesized to be a result of an altered motor control strategy as well as quadriceps weakness after ACLR. 26,27
The LSI of quadriceps strength has been significantly associated with asymmetry in landing biomechanics after ACLR. 11,12,20,28 Although double-leg squatting is less dynamic and places a smaller demand on the quadriceps compared with landing tasks, 21 asymmetry in knee kinetics during double-leg squatting may be associated with persistent quadriceps weakness after ACLR if the patient’s motor control is altered. However, no study has examined the association between persistent quadriceps weakness and asymmetry in knee kinetics during double-leg squatting. Clarifying the association between the LSI of quadriceps strength and knee extension moment during double-leg squatting is informative when considering rehabilitation to improve neuromuscular control after ACLR.
The purpose of the present study was to clarify the relationships between quadriceps strength and double-leg squatting biomechanics >1 year after ACLR. The hypothesis was that quadriceps strength deficits would be significantly associated with interlimb differences in the knee extension moment and knee to support moment ratio but not associated with interlimb differences in vertical ground-reaction force. 26,27 We further hypothesized that participants with significant strength deficits of the quadriceps would rely on hip extension and ankle plantarflexion moments instead of knee extension moments during double-leg squatting. 3,26,27,30
Methods
Participants
This study was part of a project to investigate biomechanical asymmetry during double-leg squatting after ACLR. The study protocol received institutional review board approval, and written informed consent was obtained from each participant. Some participants took part in a previous study. 10
Prior sample size calculations showed that a total of 20 participants were needed to achieve a significance level (α), statistical power (1 – β), and effect size (partial η2) of .05, 0.8 and 0.1, respectively, of the interaction effect in 2-way analysis of variance (ANOVA). The effect size was assumed based on relevant previous studies. 11,26,35 The present study enrolled 26 participants (17 female and 9 male participants; age, 23.1 ± 3.5 years; height, 166.9 ± 7.5 cm; body weight, 60.0 ± 9.2 kg). The mean time since surgery was 5.5 ± 3.8 years. The inclusion criteria were as follows: (1) primary unilateral ACLR, (2) no concomitant ligamentous injuries of grade 3 severity or requiring surgical intervention other than the primary ACL injury, (3) >1 year after ACLR surgery, (4) no restriction for sport activities, and (5) no pain during double-leg squatting. The graft source was not used as an inclusion criterion. Participants who underwent concomitant partial meniscectomy or meniscal repair were included. One year was determined because a rehabilitation period of 9–12 months is recommended to obtain sufficient function, including quadriceps strength, for safe return to sports. 34 Participants were excluded if they had undergone bilateral or revision ACLR or had a history of knee injuries in the involved or uninvolved limb in addition to primary ACLR.
Procedures
Biomechanical Evaluation of Double-Leg Squatting
All data were recorded using a motion capture system (Cortex Version 5.0.1; Motion Analysis Corporation) with 7 cameras (Hawk cameras; Motion Analysis Corporation) and 2 synchronized force plates (type 9286; Kistler AG). The sampling rates were set to 200 Hz for the marker coordinate data and 1000 Hz for the force plate data.
Participants performed a 5-minute warm-up with a stationary bicycle ergometer at a self-selected pace. After warm-up, a total of 26 retroreflective markers were placed on the iliac crest, anterior and posterior superior iliac spines (ASIS and PSIS, respectively), lateral thigh, medial and lateral femoral epicondyles, lateral shank, medial and lateral malleoli, second metatarsal head and base, fifth metatarsal head, and heel. 9 A standardized static standing trial was recorded. Then the participants performed 3 trials of 5 consecutive double-leg squats. They stood with their feet shoulder-width apart, with 1 foot on each of the force plates and their arms crossed over their chest. They were asked to squat down so that their thighs were parallel to the floor and then return to the upright standing position. 9,35 The examiner visually checked the squat depth and provided verbal feedback if the depth was insufficient. No other instructions were given regarding aspects of the squatting technique, such as trunk flexion angle, toe angle, or weight distribution. A metronome was used so that patients squatted for 2 seconds for each descent and ascent phase. 9,35 The participants were allowed to rest between each trial as needed. The rest time was usually 2 to 3 minutes.
The hip, knee, and ankle joint angles and internal joint moments were determined using Visual3D (Version 6; C-Motion). The marker trajectories and force plate data were low-pass filtered using a fourth-order, zero-lag Butterworth filter with a 12-Hz cutoff frequency. 9,30 When the ASIS markers were missed during the squatting task, the iliac crest and PSIS markers were used to fill the ASIS marker trajectory gaps. 18 Hip, knee, and ankle joint moments were calculated using a joint coordinate system with the Cardan sequence (flexion/extension first). In calculating the joint moments, we set the segment inertial parameters according to a previous report. 4 The vertical ground-reaction force and joint moments were normalized to each participant’s body weight (N/kg and N·m/kg). The peak values during each squat were derived for the vertical ground-reaction force and the hip, knee, and ankle joint moments. 26 The support moment was calculated as the sum of the peak hip and knee extension and ankle plantarflexion moments. 10,26 To assess joint contributions of the knee, hip, and ankle, we calculated 3 moment ratios as percentages relative to the support moment (ie, the ratios of knee, hip, and ankle extension moment to support moment). 10,26 The LSI of each variable was calculated as the percentage of the values in the involved limb versus the uninvolved limb. All variables were averaged across the middle 3 repetitions of the 3 trials.
Quadriceps Strength Testing
After biomechanical evaluation of double-leg squatting, we assessed the isokinetic quadriceps strength at a velocity of 60 deg/s using a dynamometer (Biodex System 3; Biodex Medical Systems). Isokinetic testing at this velocity is widely used as a clinical assessment for quadriceps strength. 1,22 A shin pad was positioned 2 finger-widths above the lateral malleolus. 8,31 Before testing begin, participants were verbally instructed to extend the knee as hard and as fast as possible throughout the range of motion. 17 Five repetitions with maximum effort were recorded after 3 to 5 submaximal practice trials to familiarize participants with the test. The LSI was calculated as the percentage of the maximum torque of the 5 repetitions in the involved limb versus that in the uninvolved limb. An LSI <90% was considered a significant deficit of quadriceps strength. 36 Participants with an LSI ≥90% were grouped into the high–quadriceps LSI (HQ) group, and those with an LSI <90% were grouped into the low–quadriceps LSI (LQ) group. 11 Maximum torque was normalized to each participant’s body weight to describe the strength of each limb (N·m/kg).
Statistical Analysis
All continuous data are presented as mean and standard deviation. Independent t tests and chi-square tests were used to compare the participants’ characteristics between the LQ and HQ groups. Two-way mixed-model ANOVA was conducted to examine the effects of group (LQ and HQ group) and limb side (involved and uninvolved side) and their interaction on squatting biomechanics, including the peak knee, hip, and ankle moment; the peak vertical ground-reaction force; and the knee, hip, and ankle to support moment ratios. Moreover, if an interaction effect was found, a linear relationship was confirmed by regression analysis. The statistical significance level was set at P < .05. These statistical analyses were performed using IBM SPSS Statistics Version 22.
Results
Eight of 26 participants (31%) who had significant strength deficits (LSI <90%) were grouped into the LQ group. No significant difference was found in the participants’ characteristics between the LQ and HQ groups, except for the LSI of quadriceps strength (Table 1). The mean quadriceps strength of both the involved and uninvolved limbs for both the LQ and HQ groups was approximately 2 times larger than the peak knee extension moment during double-leg squatting.
Characteristics of the Study Participants (N = 26) a

a Data are reported as No. of participants or mean ± SD. Boldface P value indicates statistically significant difference between groups (P < .05). BTB, bone–patellar tendon–bone; HQ, group with high LSI for quadriceps strength; LQ, group with low LSI for quadriceps strength; LSI, limb symmetry index.
A significant interaction effect between group and limb side was found for the peak knee extension moment, the knee to support moment ratio, and the hip to support moment ratio (P < .001, P = .015, and P < .001, respectively). The LQ group showed a significantly smaller peak knee extension moment in the involved limb than in the uninvolved limb (P = .001; 95% CI, −0.273 to −0.088 N·m/kg), whereas no interlimb difference was found for the HQ group (P = .137; 95% CI, −0.016 to 0.108 N·m/kg) (Figure 1A). The LQ group demonstrated a significantly smaller knee to support moment ratio in the involved limb than in the uninvolved limb (P = .005; 95% CI, −10.7% to −2.2%) (Figure 2A) but had a significantly larger hip to support moment ratio in the involved limb than in the uninvolved limb (P < .001; 95% CI, 3.2% to 8.5%) (Figure 2B). In contrast, no interlimb differences in the knee or hip to support moment ratio were found for the HQ group (P = .934 and P = .246, respectively). No interaction effect was detected for the peak hip extension or ankle plantarflexion moment (P = .282 and P = .340, respectively) (Figure 1), ankle to support moment ratio (P = .053) (Figure 2), or vertical ground-reaction force (P = .119) (Figure 3). There was no group effect on any variables (P = .105-.937).

Comparison of the peak extension moment for the (A) knee, (B) hip, and (C) ankle. Error bars indicate SD. Boldface P value indicates statistically significant difference between limbs (P < .05). HQ, group with high limb symmetry index for quadriceps strength; LQ, group with low limb symmetry index for quadriceps strength.

Comparison of the contributions of the (A) knee, (B) hip, and (C) ankle relative to the support moment. Error bars indicate SD. Boldface P values indicate statistically significant difference between limbs (P < .05). HQ, group with high limb symmetry index for quadriceps strength; LQ, group with low limb symmetry index for quadriceps strength.
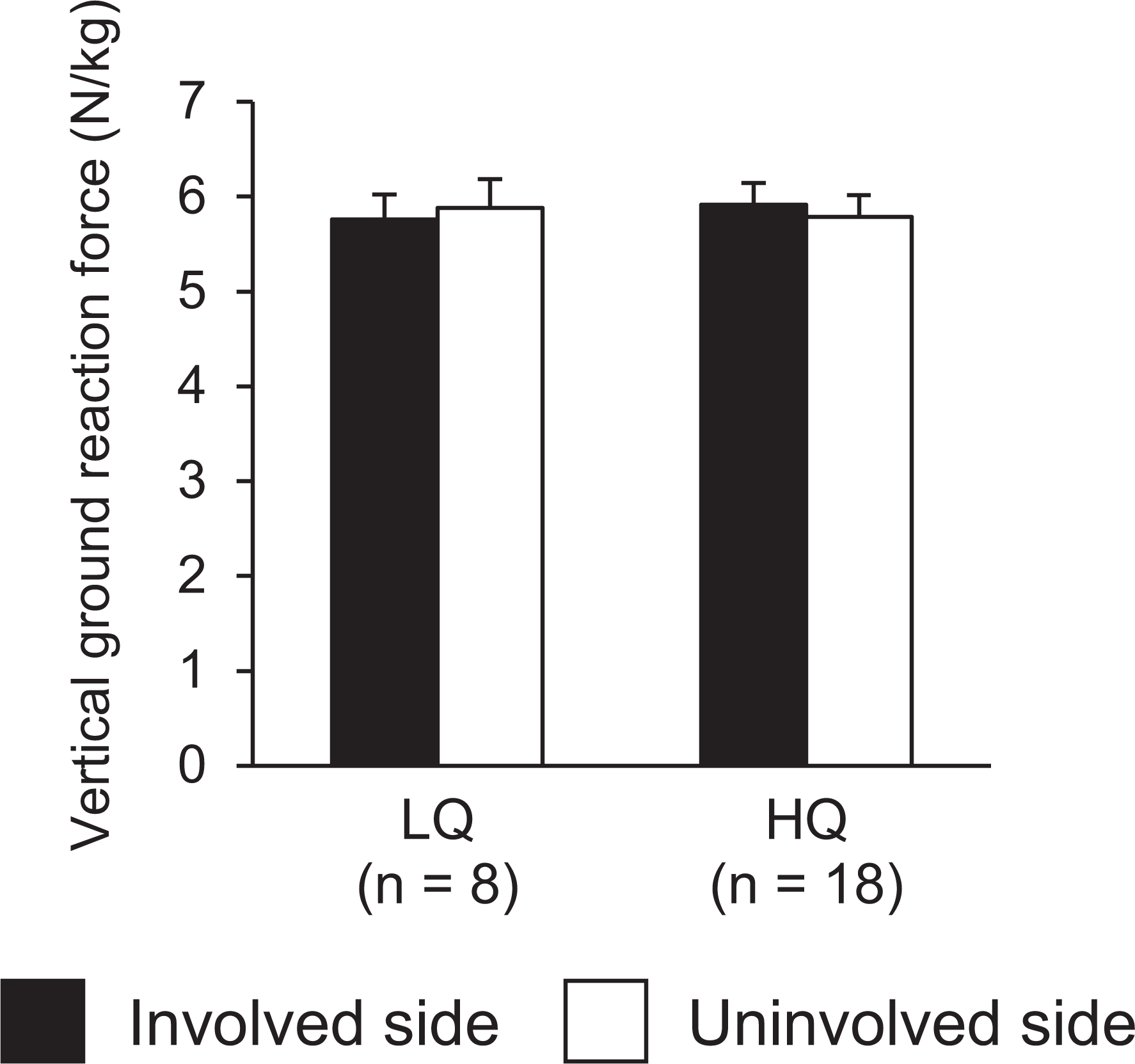
Comparison of the peak vertical ground-reaction force. Error bars indicate SD. HQ, group with high limb symmetry index for quadriceps strength; LQ, group with low limb symmetry index for quadriceps strength.
Univariate regression analysis showed that the LSIs of the peak knee extension moment, knee to support moment ratio, and hip to support moment ratio were significantly associated with the LSI for quadriceps strength (Figure 4).
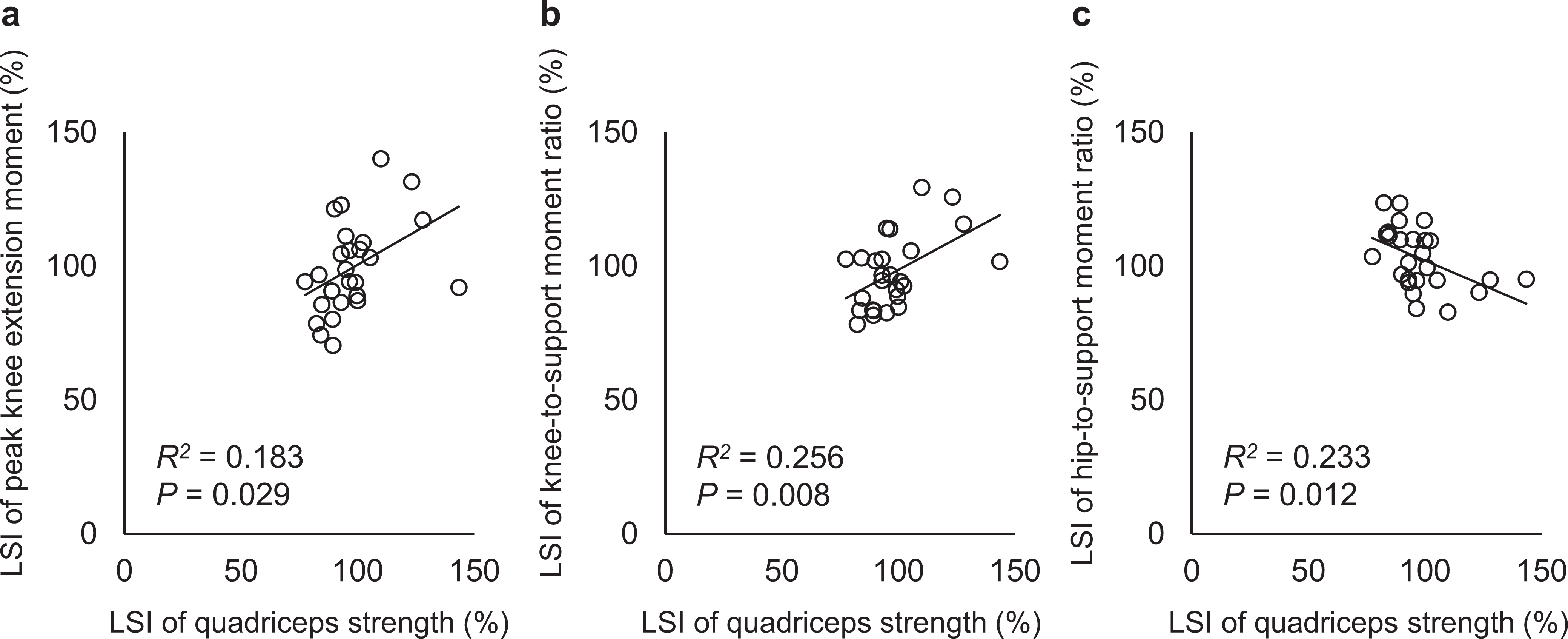
Relationship between the limb symmetry index (LSI) of quadriceps strength and the LSI of (A) the peak knee extension moment, (B) the knee to support moment ratio, and (C) the hip to support moment ratio.
Discussion
The present findings support the a priori hypothesis that quadriceps strength deficits would be associated with interlimb asymmetry in the knee moment and knee to support moment ratio during double-leg squatting. The present study revealed that the LQ group had significant interlimb differences in peak knee extension moment, knee to support moment ratio, and hip to support moment ratio during double-leg squatting. In contrast, the HQ group did not show significant interlimb differences in lower limb joint moment. The LSI of quadriceps strength was significantly associated with the LSI of the peak knee extension moment, knee to support moment ratio, and hip to support moment ratio.
The LQ group showed a significantly smaller peak knee extension moment and knee to support moment ratio but a larger hip to support moment ratio in the involved limb than in the uninvolved limb, whereas no significant interlimb difference was detected for ground-reaction force. The knee extension moment could be affected by compensation both with the contralateral limb and with the hip and ankle joint in the ipsilateral limb. 26,30 Compensation with the contralateral limb is observed as an interlimb asymmetry in the vertical ground-reaction force, which may be more apparent during the early rehabilitation phase. 30 Another compensation with the hip and ankle joint in the ipsilateral limb can be observed as the change in each joint contribution (eg, knee, hip, and ankle to support moment ratios), which can be confirmed even after completion of the rehabilitation program. 26 Participants in the LQ group decreased their knee extension moment by relying on the hip extension moment in the involved limb. In contrast, no significant interlimb differences in the knee, hip, or ankle moments or vertical ground-reaction force were found for the HQ group. These findings indicate that persistent quadriceps weakness after ACLR is associated with persistent interlimb asymmetries in the peak knee extensor moment and the contributions of knee and hip extension moments during double-leg squatting.
Previous studies showed a significantly linear relationship between the LSI of quadriceps strength and knee extension moment during jump-landing tasks. 12,28 The present study is the first to reveal that the LSI of quadriceps strength was significantly associated with the LSI of the peak knee extension moment, knee to support moment ratio, and hip to support moment ratio. The present findings are interesting because the maximum isokinetic strength in both the involved and the uninvolved limbs was approximately 2 times larger than the peak knee extension moment during double-leg squatting for both the LQ and HQ groups. Thus, the interlimb asymmetry in knee extension moment mainly seen in the LQ group would not be caused simply by insufficient quadriceps muscle strength. Nevertheless, asymmetry in the peak knee extension moment during double-leg squatting was associated with asymmetry in quadriceps strength. These results support the previous hypothesis that interlimb asymmetry in knee extensor moment during double-leg squatting is caused by altered motor control to reduce quadriceps demand. 26,27 In fact, quadriceps weakness after ACLR is associated with reduced excitability of the corticospinal pathways. 16,25 Moreover, a similar relationship between quadriceps strength and knee extension moment has been reported in gait during which the demand on the quadriceps muscle is not as large, 17,23,29 which also supports that knee extensor moment asymmetry after ACLR is caused by altered motor control and is not simply the result of the deficit in quadriceps strength.
One-third of the participants in the present study showed significant deficits in quadriceps strength. This result indicates that a certain number of patients have persistent quadriceps weakness >1 year after ACLR, as shown in previous systematic reviews. 1,22,33 We were not able to reveal the cause-and-effect relationship between quadriceps strength and altered motor control during double-leg squatting because of the cross-sectional design of this study. However, the study results suggest that the asymmetry in knee extension moment during double-leg squatting may be caused by changes in motor control and not simply by insufficiency of quadriceps strength, suggesting that quadriceps weakness and altered motor control may interact. A recent study also showed that restoration of symmetrical knee flexion motion during jump-landing requires improvement in neuromuscular control as well as quadriceps strength. 9 Researchers have hypothesized that the persistence of interlimb asymmetry in the knee extensor moment would interfere with improvement in quadriceps strength. 26,27,35
Double-leg squatting is a basic closed kinetic chain exercise in rehabilitation after ACLR. However, squatting without instruction would not be efficient in strengthening the quadriceps because patients with quadriceps weakness on the involved side would squat with reduced quadriceps demand. To effectively restore symmetrical biomechanics during squatting, we should also focus on altered motor control. A recent study reported that pelvic rotation toward the involved side (eg, if the involved side is the left, the right side of the pelvis moves anteriorly and/or the left side moves posteriorly) was associated with a smaller knee extension moment and knee to support moment ratio in the involved limb than in the uninvolved limb during double-leg squatting after ACLR. 10 As well, a more anterior center of pressure position in the foot of the involved side (or nondominant side) compared with the uninvolved side (or dominant side) is also associated with a smaller knee extensor moment in the involved limb than in the uninvolved limb during double-leg squatting for patients after ACLR and for young healthy individuals. 3,9,10 Instruction regarding pelvic rotation and biofeedback regarding the center of pressure position may be useful in reducing interlimb asymmetry in the knee extensor moment during double-leg squatting.
Limitations
There were some limitations in the present study. First, a cause-and-effect relationship was not determined by the present study due to the cross-sectional design. Longitudinal studies are needed to clarify the association between persistent quadriceps strength and altered motor control during double-leg squatting. Second, the lower limb muscle activities were not assessed. Therefore, it is unclear whether the smaller knee extension moment seen in the involved limb of the LQ group was due to decreased quadriceps activity or more antagonist muscle activity. Third, the number of patients in the LQ group was small, which may limit the statistical power. In addition, due to the small number of participants with bone–patellar tendon–bone grafts, the effect of the graft types could not be clarified. Fourth, data on the time since injury were lacking, and this parameter may have been different in the LQ and HQ groups.
Conclusion
Quadriceps strength deficits that are present >1 year after ACLR are associated with asymmetry in the peak knee extension moment, the knee to support moment ratio, and the hip to support moment ratio during double-leg squatting. Moreover, the LSI of quadriceps strength was associated with the LSI of peak knee extension moment, knee to support moment ratio, and hip to support moment ratio. The present findings indicate that individuals with quadriceps strength deficits had reduced knee extensor moment on the involved side during double-leg squatting despite loading at approximately half of maximum strength. Therefore, quadriceps strengthening exercises, together with interventions to improve neuromuscular control, may reduce asymmetrical biomechanics during double-leg squatting.
Footnotes
Final revision submitted March 14, 2023; accepted March 31, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by a grant from the Japan Society for the Promotion of Science KAKENHI (No. JP20K19477). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Faculty of Health Sciences, Hokkaido University (approval No. 19-72).