
Abstract
Background:
An increased femoral anteversion angle (FAA) is a predisposing factor for recurrent patellar dislocations (RPDs), and combined procedures including derotational distal femoral osteotomy (DDFO) have been shown to be good options.
Purpose:
To investigate the safety and effectiveness of combined DDFO on clinical and radiological outcomes to treat RPDs with an increased FAA.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
This review was performed according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) guidelines. We searched 7 databases for articles from inception to March 10, 2023, that reported outcomes after combined DDFO in patients with an RPD and increased FAA. Two reviewers independently extracted data and assessed study quality. Outcomes evaluated were functional scores, redislocation rates, complications, satisfaction, and radiological parameters. A meta-analysis was performed to pool functional scores, with data reported as mean differences (MDs) and 95% confidence intervals (CIs).
Results:
Included were 8 studies of 189 knees from 183 patients, with a mean patient age of 22.4 years and a mean follow-up of 33.4 months. The mean preoperative FAA ranged from 31° to 42.70°, and the mean postoperative FAA ranged from 10° to 19.08°. Significant improvements were found in the Kujala score (MD, 26.96 [95% CI, 23.54 to 30.37]), Lysholm score (MD, 26.17 [95% CI, 22.13 to 30.22]), visual analog scale score for pain (MD, –2.61 [95% CI, –3.12 to –2.10]), and Tegner activity score (MD, 1.33 [95% CI, 0.86 to 1.79]). No subluxation or redislocation occurred. The overall complication rate was 10.6%, and most of the complications were pain (60%) and limited knee activity (20%). The overall satisfaction rate was 83.3%. The patellar tilt angle significantly decreased from 40.7° ± 11.9° to 20.5° ± 8.7° and from 26.35° ± 6.86° to 11.65° ± 2.85° in 2 studies.
Conclusion:
Combined DDFO was found to be safe and effective for the treatment of RPDs and an increased FAA by addressing both patellar dislocations and torsional malalignment. However, because of the lack of comparisons, it remains to be investigated when DDFO should be combined in such patients.
Keywords
A recurrent patellar dislocation (RPD), a common and multifactorial condition that predominantly affects children and adolescents aged between 10 and 17 years, can result in patellofemoral pain, decreased function, reduced quality of life, and patellofemoral arthritis in the long term. 25,26,30,31 Multiple pathoanatomic abnormalities, including trochlear dysplasia, an increased tibial tubercle–trochlear groove (TT-TG) distance, patella alta, and torsional deformities, are often noted to be risk factors of an RPD. 24,38
An increased femoral anteversion angle (FAA), measured as the angle formed between a line passing through the centers of the femoral head and neck and a line tangent to the posterior condyles, has been recognized as one of the predisposing factors for an RPD. While the treatment guideline for RPDs with an increased FAA remains controversial, some studies have highlighted that isolated medial patellofemoral ligament (MPFL) reconstruction had enough ability to achieve favorable outcomes and low failure rates, even in the presence of an increased FAA. 2,7,17,18,22,26,36 However, an increased FAA can lead to a sustained lateralized force vector on the patella, thus resulting in increased lateralization of patellar tracking and causing increased stress on the reconstructed MPFL graft. 4,13,15,35 Therefore, isolated MPFL reconstruction without addressing this osseous deformity may result in MPFL graft failure and redislocations. 15,16,21,39 An increased FAA also had adverse effects on the clinical outcome after MPFL reconstruction combined with tibial tubercle osteotomy (TTO). 9,38 In addition, patients with RPDs had a 1.56-fold higher FAA compared with controls. 6
Therefore, derotational distal femoral osteotomy (DDFO) has been proposed as a treatment option to correct an increased FAA in patients with RPDs. As these patients usually have multiple abnormalities that need to be surgically addressed simultaneously and DDFO is a relatively large procedure, the safety and effectiveness of combined procedures with DDFO deserve attention. Although previous studies have reported improved clinical outcomes, patellar tracking, and patellofemoral congruence after combined DDFO, there is a lack of studies analyzing clinical or radiological outcomes after combined DDFO using quantitative analyses. 14,35
The main purpose of this systematic review and meta-analysis was to update the current evidence and pool together relevant studies to investigate clinical and radiological outcomes after combined DDFO in the management of RPDs with an increased FAA. The secondary purpose was to summarize (1) which radiological measurements of the FAA were used and (2) what cutoff values were used to indicate DDFO. It was hypothesized that combined DDFO is safe and effective in the treatment of RPDs and an increased FAA, leading to favorable clinical and radiological outcomes.
Methods
Literature Search
This review was performed according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) guidelines. 19 A systematic and comprehensive online literature search was conducted using PubMed, MEDLINE, Embase, Web of Science, CINAHL, Scopus, and Cochrane Library from the inception of the database to March 10, 2023, by 2 independent reviewers (K.H. and Y.N.). There were no restrictions on the publication type, journal, and language. Search terms that kept to the PICO (population, intervention, comparison, outcome) framework were classified into 4 groups as follows: (1) patellar, patella, patellofemoral, PFJ (patellofemoral joint); (2) dislocation, instability, subluxation, luxating, dysfunction; (3) derotational, rotational, torsional; and (4) osteotomy. Terms within groups 1 to 3 were combined with the “OR” Boolean operator, and the 4 groups were combined with the “AND” Boolean operator. Details of the final search algorithm for PubMed are shown in Appendix Table A1.
After excluding duplicate articles, the remaining articles were examined and screened by 2 independent reviewers (K.H. and A.F.), starting from titles and abstracts to evaluate their relevance to the research question according to the inclusion and exclusion criteria. If not excluded during this phase, full-text articles were discussed among the authors and then cross-referenced to ensure the inclusion of all relevant studies. All references from the included studies were screened manually for possible articles not found through the electronic searches. Experts were also contacted for further article suggestions and pertinent unpublished studies. In cases of ≥2 studies by the same author, only the latest study was included if the patients were duplicated. Any disagreement was resolved through discussions with the senior author (F.W.).
Eligibility Criteria
The inclusion criteria for this review were as follows: (1) patients with RPDs undergoing combined DDFO; (2) patients with a minimum follow-up of 12 months; (3) studies that reported clinical or radiological outcomes; (4) cohort studies, case-control studies, or case series with levels of evidence of 1 to 4; and (5) studies published in English. The exclusion criteria were as follows: (1) studies reporting on DDFO not in cases of RPDs; (2) patients with a history of ipsilateral torsional tibial osteotomy; (3) studies with the duplication of patients; (4) studies not reporting quantitative data; and (5) nonclinical studies, systematic reviews, meta-analyses, case reports, technical guides, basic science articles, commentaries, letters, expert opinions, registries, and revisions. The articles that did not meet all inclusion criteria or met at least one exclusion criterion were excluded.
Data Extraction
The following data were extracted from the full-text version of the included articles: (1) study characteristics: lead author name, publication date, publication journal, study design, level of evidence, and study period; (2) patient characteristics: sample size, number of knees, mean age at the time of surgery, sex, and follow-up duration; (3) FAA: measurement modality, preoperative and postoperative FAA, cutoff value, and correction angle; (4) surgical details: surgical approach and combined procedures; and (5) patient outcomes: preoperative and postoperative clinical and radiological outcomes. Clinical outcomes included functional scores, redislocation rates, complications, and patient satisfaction.
Two reviewers (Y.N. and A.F.) independently performed data extraction. Any inconsistency was resolved through discussions with the senior author (F.W.). The number of knees was considered to be the same as the number of patients if not reported. The data regarding outcomes were extracted as means and standard deviations. If reported as medians and ranges/interquartile ranges, the data were transformed into means and standard deviations. 12,33 If the data were incomplete, an attempt was made to contact the corresponding author of the included study. If no response was received, the relevant data were neglected as if not reported. The data were checked and recorded into predetermined tables in Excel (Version 2016; Microsoft).
Risk-of-Bias Assessment
The methodological quality of the included studies was evaluated using the MINORS (Methodological Index for Non-Randomized Studies) criteria, which consist of 12 and 8 items for comparative and noncomparative studies, respectively. 28 The score for each item is based on whether the item was reported appropriately. There is a low risk of bias when the score for comparative studies is 21 to 24 and the score for noncomparative studies is 13 to 16, and there is a high risk of bias when the score for comparative studies is ≤20 and the score for noncomparative studies is ≤12. The MINORS score was assessed by 2 independent reviewers (K.H. and Y.N.), and the average score was used as the final score.
Statistical Analysis
Continuous variables were reported as means and standard deviations, and noncontinuous variables were reported as frequencies. Heterogeneity was assessed using the I 2 statistic in which an I 2 of 25%, 50%, and 75% represents low, moderate, and high heterogeneity, respectively. 11 In cases of heterogeneity, a random-effects model was used to analyze pooled estimates of preoperative and postoperative differences for outcomes. Otherwise, a fixed-effects model was used for pooled analyses. The mean difference (MD) was reported with the 95% confidence interval (CI) using the inverse-variance method. The overall effect was considered statistically significant if P < .05. The means of the individual study and pooled estimates of outcomes were summarized in forest plots.
The overall pooled effect size was analyzed using Review Manager software (Version 5.3; The Cochrane Collaboration). The outcomes not included in the meta-analysis were synthesized in a combination of descriptive and narrative analyses. The interreviewer reliability of the risk-of-bias assessment was measured using the Cohen kappa coefficient. The Egger test was performed to evaluate the risk of publication bias.
Results
Identification of Studies
The electronic searches resulted in 530 articles (PubMed: n = 85; Web of Science: n = 95; MEDLINE: n = 85; CINAHL: n = 39; Embase: n = 98; Scopus: n = 125; and Cochrane Library: n = 3). After removing 361 duplicates, 169 articles were assessed based on titles and abstracts. Of these, 136 articles were excluded, and 33 articles proceeded to a full-text review for eligibility. Then, 25 articles were excluded for reasons described in Figure 1, and 8 articles were included. 1,3,5,10,13,20,32,37 No additional study meeting the inclusion criteria was identified by manually checking the references of included studies. Ultimately, 8 articles 1,3,5,10,13,20,32,37 reporting outcomes after combined DDFO were included. The PRISMA flow diagram is shown in Figure 1.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) flowchart showing the selection process of studies.
Characteristics of Included Studies
All 8 studies were published in English between 2015 and 2022. One study 37 was a retrospective comparative cohort study with a level of evidence of 3 that compared the outcomes of patients undergoing DDFO versus non-DDFO procedures, and 7 studies 1,3,5,10,13,20,32 were retrospective noncomparative case series with a level of evidence of 4. The characteristics of included studies are shown in Table 1.
Characteristics of Included Studies

These studies included a total of 189 knees from 183 patients. The study by Frings et al 10 reported outcomes after DDFO or varus osteotomy, and only 16 patients undergoing DDFO were included. The mean age at the time of surgery was 22.4 years (range, 18.2-28 years). There were more women than men, with a sex distribution of 21 men (14% [range, 0%-30.8%]) and 129 women (86% [range, 69.2%-100%]) in 7 studies. 1,3,5,10,20,32,37 The mean follow-up was 33.4 months (range, 16.4-44 months). Patient characteristics are shown in Table 2.
Characteristics of Included Patients a
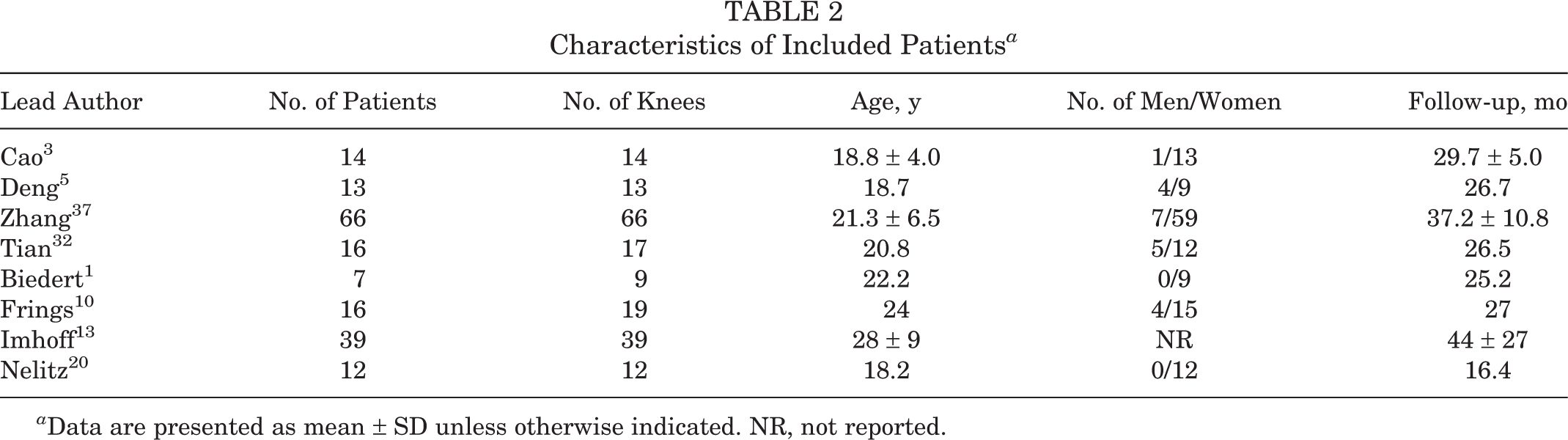
a Data are presented as mean ± SD unless otherwise indicated. NR, not reported.
Quality Assessment
The interreviewer reliability of the risk-of-bias assessment was perfect, with a Cohen kappa coefficient of 1. The MINORS score was 20 for the 1 comparative study 37 and was a mean of 12.6 ± 1.0 (range, 12-14) for the 7 noncomparative studies. 1,3,5,10,13,20,32 The overall risk of bias was high in 6 studies 1,5,10,13,20,37 and low in 2 studies 3,32 (Table 3). The most common reason that reduced the quality of included studies was retrospective nature. In addition, 4 studies 1,5,10,20 did not perform a prospective calculation of the sample size, 1 study 13 had a loss to follow-up rate of >5%, and the comparative study 37 did not have a contemporary control group.
Quality Assessment Using MINORS Criteria a

a MINORS items: (1) clearly stated aim, (2) inclusion of consecutive patients, (3) prospective collection of data, (4) endpoints appropriate to the aim of the study, (5) unbiased assessment of the study endpoint, (6) follow-up period appropriate to the aim of the study, (7) loss to follow-up <5%, and (8) prospective calculation of the study size. Additional MINORS items for comparative studies: (9) adequate control group, (10) contemporary groups, (11) baseline equivalence of groups, and (12) adequate statistical analyses. MINORS, Methodological Index for Non-Randomized Studies. Dashes indictate not applicable.
FAA and Surgical Details
Regarding the measurement technique of the FAA, Cao et al, 3 Deng et al, 5 and Zhang et al 37 used reconstructed 3-dimensional computed tomography (CT); Biedert 1 and Tian et al 32 used axial CT; Nelitz et al 20 used axial magnetic resonance imaging; and Frings et al 10 and Imhoff et al 13 used axial CT or magnetic resonance imaging. The measurement methods in the included studies were the same, with the FAA defined as the angle formed between the femoral neck axis and the line tangent to the posterior condyles. The cutoff values of the FAA for DDFO were reported in all studies, ranging from 20° to 30°, and 25° was the most common indication, followed by 30°. The mean preoperative FAA ranged from 31° to 42.70° in all studies, and the mean postoperative FAA ranged from 10° to 19.08° in 6 studies. 3,5,10,13,32,37 The mean correction angle ranged from 13.69° to 28.6° in 6 studies. 3,5,10,13,32,37 The FAAs are shown in Table 4.
FAA of Included Studies a
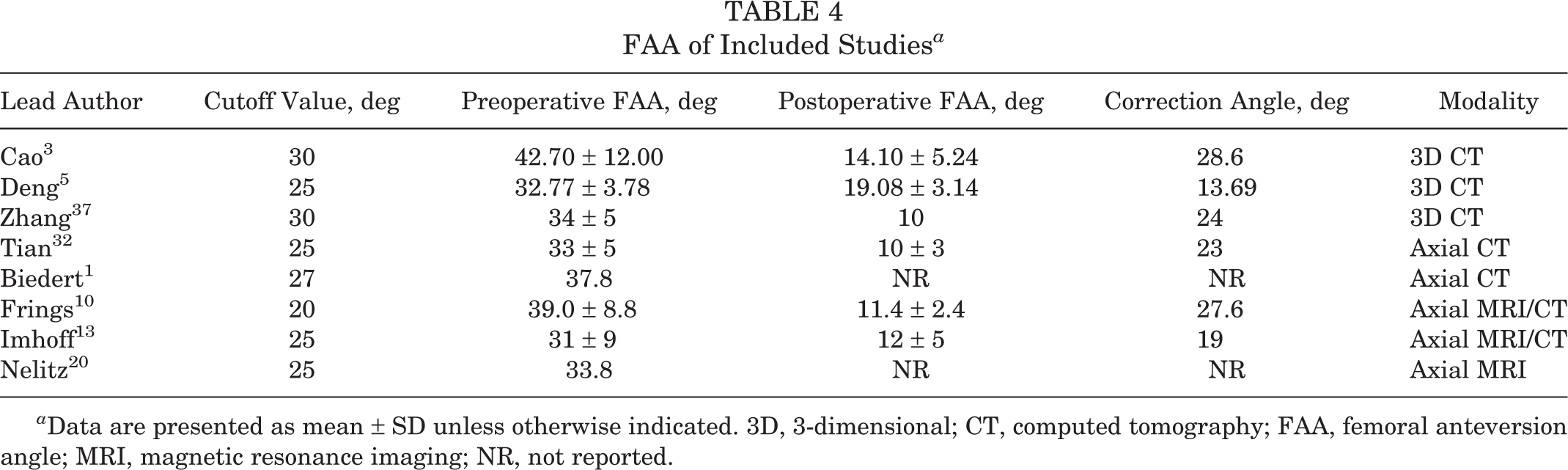
a Data are presented as mean ± SD unless otherwise indicated. 3D, 3-dimensional; CT, computed tomography; FAA, femoral anteversion angle; MRI, magnetic resonance imaging; NR, not reported.
Supracondylar DDFO was performed in all studies, usually with a lateral approach. DDFO was an isolated bony procedure in 4 studies. 3,5,20,32 In the other 4 studies, 1,10,13,37 DDFO was accompanied by additional bony procedures to address concomitant bony deformities. Of them, TTO was the most common procedure, followed by valgus/varus correction and trochleoplasty. Patellar stabilization procedures were performed in all studies, of which MPFL reconstruction was performed in 6 studies. 3,5,13,20,32,37 The other 2 studies 1,10 performed medial retinaculum constriction, MPFL shortening , MPFL augmentation, or lateral retinaculum lengthening. The surgical details are shown in Table 5.
Surgical Details of Included Studies a

a MPFL, medial patellofemoral ligament; TTO, tibial tubercle osteotomy.
Functional Scores
Functional scores are shown in Table 6. The Kujala score, Lysholm score, and visual analog scale score for pain significantly improved from preoperatively to postoperatively: MD, 26.96 (95% CI, 23.54 to 30.37; P < .00001; I 2 = 56%); MD, 26.17 (95% CI, 22.13 to 30.22; P < .00001; I 2 = 59%); and MD, –2.61 (95% CI, –3.12 to –2.10; P < .00001; I 2 = 10%), respectively (Figures 2 –4). The assessment of heterogeneity was performed, and excluding the study causing heterogeneity reduced statistical heterogeneity; however, the findings of significant improvements were not affected for the Kujala score (MD, 27.99 [95% CI, 24.95-31.04]; P < .00001; I 2 = 35%) and Lysholm score (MD, 24.76 [95% CI, 22.44-27.08]; P < .00001; I 2 = 0%). There was no publication bias identified using the Egger test (P = .453).
Functional Scores of Included Studies a
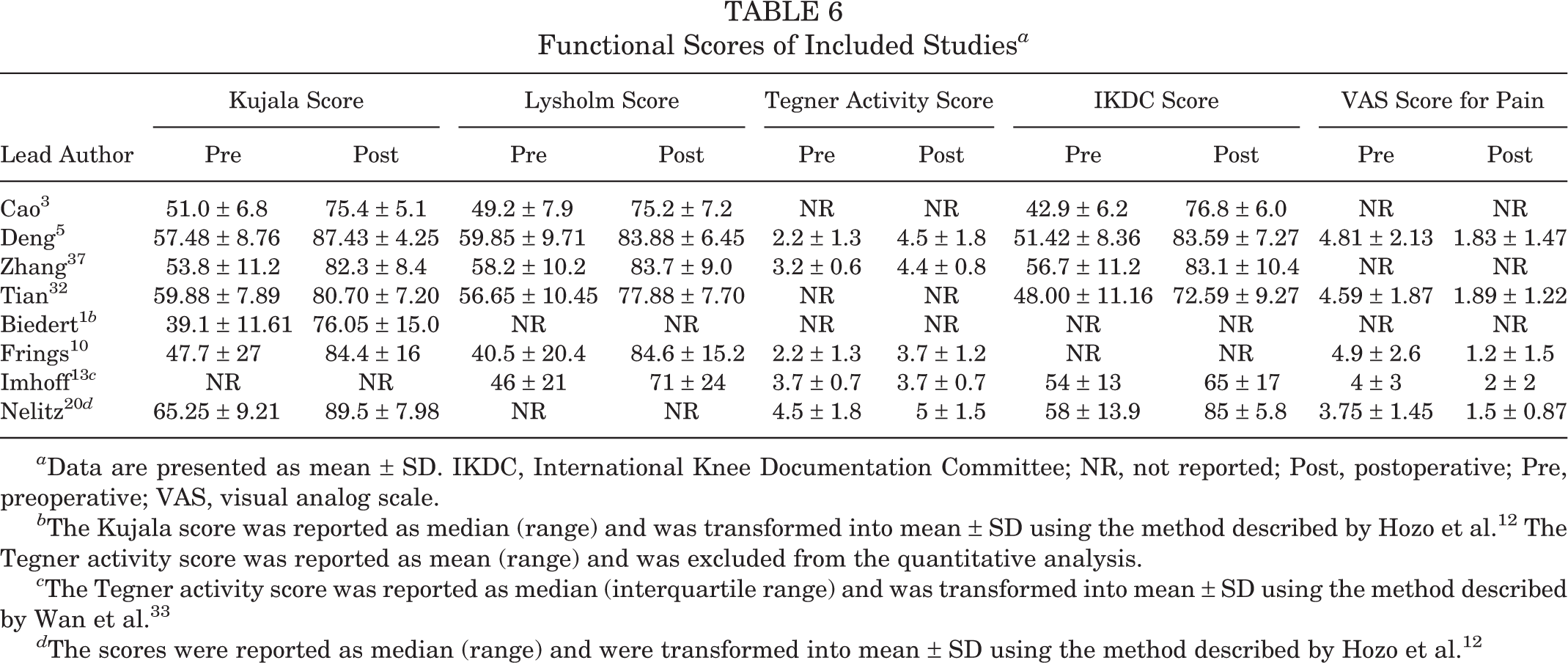
a Data are presented as mean ± SD. IKDC, International Knee Documentation Committee; NR, not reported; Post, postoperative; Pre, preoperative; VAS, visual analog scale.
b The Kujala score was reported as median (range) and was transformed into mean ± SD using the method described by Hozo et al. 12 The Tegner activity score was reported as mean (range) and was excluded from the quantitative analysis.
c The Tegner activity score was reported as median (interquartile range) and was transformed into mean ± SD using the method described by Wan et al. 33
d The scores were reported as median (range) and were transformed into mean ± SD using the method described by Hozo et al. 12

Forest plot of Kujala scores. Data were pooled with a random-effects model. IV, inverse variance.

Forest plot of Lysholm scores. Data were pooled with a random-effects model. IV, inverse variance.
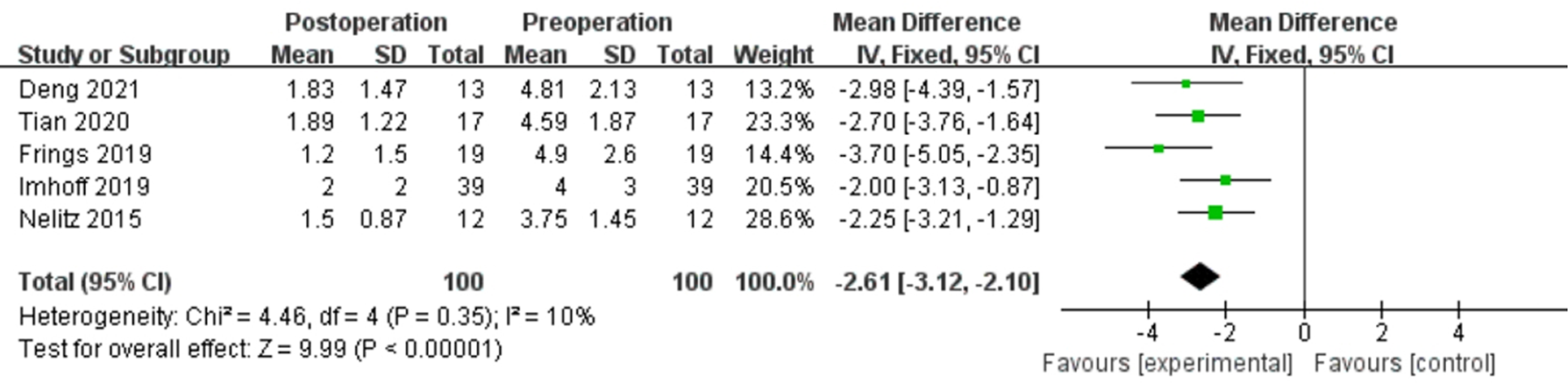
Forest plot of visual analog scale scores for pain. Data were pooled with a fixed-effects model. IV, inverse variance.
The Tegner activity score was reported in 5 studies, 5,10,13,20,37 of which 3 studies 5,10,37 reported significant improvements and 2 studies 13,20 reported no significant improvement. The heterogeneity assessment showed high heterogeneity with I 2 = 91%, and thus, pooled estimation was not performed. The study by Imhoff et al 13 was the main source of the heterogeneity, and excluding this study reduced statistical heterogeneity, showing a significant improvement (MD, 1.33 [95% CI, 0.86-1.79]; P < .00001; I 2 = 36%) (Figure 5).
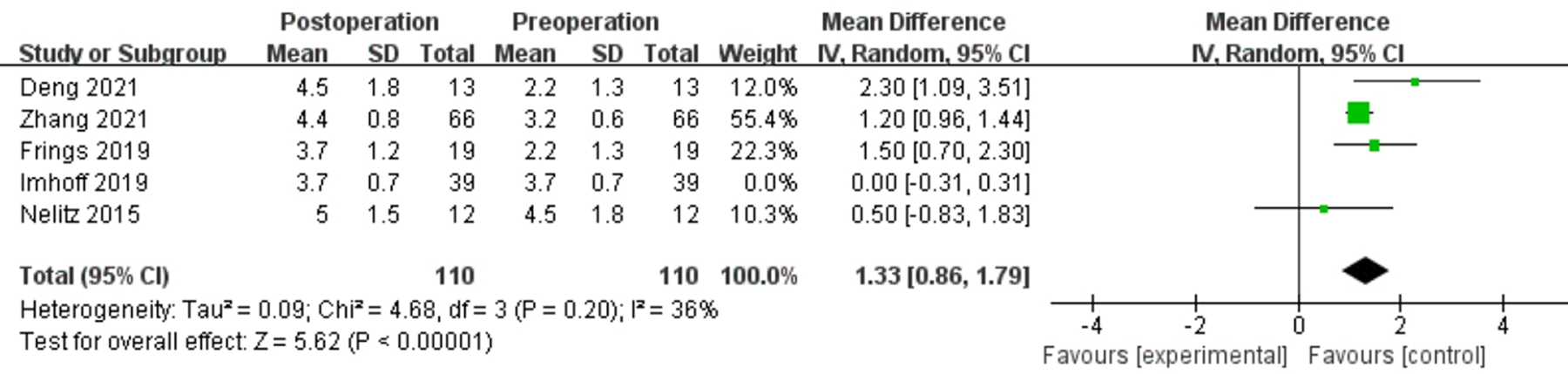
Forest plot of Tegner activity scores. Data were pooled with a random-effects model. IV, inverse variance.
Redislocations and Complications
No subluxation or redislocation occurred in any study. Regarding patellar tracking, the proportion of patients with a positive J-sign postoperatively was significantly lower than that preoperatively. 3,37 Postoperative complications and corresponding treatment methods were reported in a total of 20 knees from 5 studies 1,10,13,20,32 (Table 7). The complication rate ranged from 0% to 100%, with an overall rate of 10.6%. Most of the complications were pain (60%) and limited knee activity (20%), which were successfully resolved after treatment, except for 1 case of persistent pain. Also, 14 reoperations were reported in 3 studies, 1,10,13 including removal of the plate and revision surgery. Bone healing at the osteotomy site was achieved in all cases, and none of the patients experienced delayed union or nonunion.
Complications and Corresponding Treatment Methods of Included Studies a

a MPFL, medial patellofemoral ligament. Dashes indicate not applicable.
Patient Satisfaction
Patient satisfaction was reported in 5 studies, 1,10,13,20,32 ranging from 71.8% to 100%, with an overall satisfaction rate of 83.3%. Tian et al 32 reported that 14 patients (82.4%) were very satisfied (n = 8) or satisfied (n = 6), while 2 patients were partially satisfied, and 1 patient was dissatisfied. Biedert 1 reported that patients were satisfied with their knee function for 8 of 9 knees (88.9%). Frings et al 10 reported that all patients were highly satisfied. Imhoff et al 13 reported that 28 patients (71.8%) were very satisfied (n = 13) or satisfied (n = 15), 6 patients were partially satisfied, and 5 patients were dissatisfied. Nelitz et al 20 reported that 11 patients (91.7%) were very satisfied (n = 8) or satisfied (n = 3), 1 patient was partially satisfied, and nobody was dissatisfied.
Radiological Outcomes
None of the radiological outcomes was reported >3 times, and thus, pooled analysis was not performed. There were 2 studies 3,37 that evaluated residual MPFL graft laxity, showing a significant improvement in postoperative patellar stability and a significantly lower rate of residual MPFL graft laxity in the combined DDFO group (6%) than in the isolated MPFL reconstruction group (19%). The patellar tilt angle significantly decreased from 40.7° ± 11.9° to 20.5° ± 8.7° 3 and from 26.35° ± 6.86° to 11.65° ± 2.85°. 32 A decreased TT-TG distance was reported in 3 studies, 2 of which showed a significant decrease from 19.63 ± 3.21 to 13.29 ± 2.78 mm 5 and from 15.63 ± 2.07 to 14.69 ± 1.78 mm, 32 while the other study 3 did not show significance from 16.9 ± 3.6 to 15.9 ± 3.9 mm. There was no significant change regarding the Caton-Deschamps index after surgery. 3,5
Discussion
The principal finding of this review is that combined DDFO was a safe and effective procedure in the management of RPDs with an increased FAA, yielding favorable knee function, pain relief, low redislocation and complication rates, high patient satisfaction, and improved patellofemoral congruence by addressing both patellar dislocations and torsional malalignment. However, because of the lack of comparisons, it remains to be investigated when DDFO should be combined in patients with RPDs and an increased FAA.
For successful outcomes in the treatment of patients with an increased FAA, DDFO has been added usually in a combined procedure to remove internal rotation of the distal femur and restore the normal geometric vector acting on the patella based on the concept that all anatomic contributing factors should be corrected. 8,23,29 However, as DDFO is a relatively large procedure that requires a prolonged recovery time and involves a greater risk of complications, the safety and effectiveness of combined DDFO are still to be verified.
Regarding the effectiveness of combined DDFO, the significant improvements in functional scores, including the Kujala, Lysholm, International Knee Documentation Committee, and visual analog scale scores, as well as high patient satisfaction demonstrated the ability of DDFO to improve knee function and reduce pain in patients with RPDs and an increased FAA. The pooled analysis also showed a significant improvement in the Tegner activity score, indicating that a high activity level could be achieved after combined DDFO. In addition, no subluxation or redislocation occurred in all studies, which demonstrated good patellar stability after surgery. From the perspective of radiological outcomes, the patellar tilt angle, which indicated patellofemoral congruence, significantly improved after combined DDFO.
Regarding the safety of combined DDFO, the overall complication rate was 10.6%, and most of the complications were pain and limited knee activity, which were successfully resolved after treatment. Bone healing at the osteotomy site was achieved in all cases, and none of the patients experienced delayed union or nonunion. The improved clinical outcomes also demonstrated that no additional risks, caused by combined DDFO that led to delayed rehabilitation, knee pain, and motion limitation, occurred. Therefore, the safety of combined DDFO can be confirmed.
It should be noted that all studies included concomitant procedures, including soft tissue procedures and bony procedures. Although these procedures make it impossible to investigate the exact contribution of DDFO in stabilizing the patella, it is essential to combine necessary surgical procedures in clinical practice. It is crucial to clarify the exact causes of an RPD, as many patients with RPDs present not only one anatomic risk factor, such as an increased TT-TG distance, which has a negative influence on patellar stability and tracking if left uncorrected and should be addressed simultaneously. In addition, soft tissue procedures are indispensable, as bony procedures can only address osseous deformities, and an insufficient MPFL or damaged medial soft tissue is still a potential risk factor for patellar redislocations.
The indication for DDFO in the treatment of RPDs remains controversial, which is mostly based on personal preference and experience. Many studies usually performed DDFO when the preoperative FAA exceeded a predetermined threshold, usually varying from 20° to 30°. This discrepancy might be prominent when different measurement methods for the FAA were used in different studies. 27 A biomechanical study has demonstrated that isolated MPFL reconstruction may be insufficient when the FAA is >20°. 16 Zhang et al 37,38 reported that a higher FAA (>30°) was negatively associated with worse patient-reported outcomes after MPFL reconstruction and combined TTO and further recommended that patients with an FAA >30° were potential candidates for DDFO. The most common cutoff value of the FAA in this review was 25°, followed by 30°. Therefore, an FAA >30° may be an appropriate indication for DDFO, and an FAA >25° should be considered with other factors. 21,34,39
Overtreatment should be avoided in cases of an increased TT-TG distance, as 3 studies 3,5,32 showed that the TT-TG distance decreased simultaneously to some extent after DDFO. DDFO should be performed first, followed by a careful evaluation of patellar tracking and stability to determine whether TTO should be performed at the same time. However, there is no study that has confirmed that DDFO could alter the TT-TG distance in which a stabilizing effect of DDFO may occur from aligning the trochlear groove with the axial force vector generated by the quadriceps mechanism.
Regarding clinical relevance, this review demonstrated that combined DDFO was a safe and effective procedure for patients with RPDs and an increased FAA. However, it remains unclear when DDFO should be combined in these patients because of a lack of comparisons. In addition, it could be realized that current studies reporting on DDFO are still inadequate, especially large-scale prospective comparative studies. The amount of evidence for the safety and effectiveness of DDFO in this review could lead to more higher-level studies investigating the rationale of DDFO in the treatment of RPDs and an increased FAA.
Limitations
This study has several limitations. First, all included studies were retrospective with a relatively low level of evidence, and no randomized controlled comparative studies were included because there were no such publications. Second, no direct comparisons could be performed between the patients with and without DDFO because of the lack of controls. As in studies without control groups, surgeons generally report good and not bad outcomes, which is a major bias for such studies. Third, the sample size of the included studies was relatively small. However, as DDFO is a relatively novel procedure, these limitations are unavoidable and understandable. Fourth, because all studies included concomitant procedures, it is impossible to know the exact contribution of DDFO to patellar stabilization when combined with other procedures. However, the treatment of RPDs should consider multiple deformities and combine several procedures in clinical practice. Fifth, the functional scores used in this review were not specifically validated for patients with RPDs, which may reduce the accuracy of the results.
Conclusion
Combined DDFO was a safe and effective procedure in the treatment of RPDs and an increased FAA, yielding favorable knee function, pain relief, low redislocation and complication rates, high patient satisfaction, and improved patellofemoral congruence by addressing both patellar dislocations and torsional malalignment. However, because of the lack of comparisons, it remains to be investigated when DDFO should be combined in patients with RPDs and an increased FAA. Large-scale prospective comparative studies are needed to confirm the findings in this review.
Footnotes
Final revision submitted March 14, 2023; accepted March 31, 2023.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. The ethics approval was obtained from the ethics committee of Third Hospital of Hebei Medical University. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Appendix
PubMed Search Algorithm

| Search Strategy |
|---|
| 1. patellar [Title/Abstract] |
| 2. patella [Title/Abstract] |
| 3. patellofemoral [Title/Abstract] |
| 4. PFJ [Title/Abstract] |
| 5. #1 OR #2 OR #3 OR #4 |
| 6. dislocation [Title/Abstract] |
| 7. instability [Title/Abstract] |
| 8. subluxation [Title/Abstract] |
| 9. luxating [Title/Abstract] |
| 10. dysfunction [Title/Abstract] |
| 11. #6 OR #7 OR #8 OR #9 OR #10 |
| 12. derotational [Title/Abstract] |
| 13. rotational [Title/Abstract] |
| 14. torsional [Title/Abstract] |
| 15. #12 OR #13 OR #14 |
| 16. osteotomy [Title/Abstract] |
| 17. #5 AND #11 AND #15 AND #16 |