
Abstract
Background:
Underwater rugby (UWR) is a team sport. Athletes require a high degree of strength, endurance, speed, and coordination involving intense physical contact. Currently, a paucity of literature exists regarding injury occurrence in UWR.
Purpose:
To examine the nature and prevalence of acute and overuse injuries in UWR.
Study Design:
Descriptive epidemiology study.
Methods:
Between November 2020 and March 2021, a total of 720 German UWR athletes were invited to take an online survey developed by orthopaedic specialists with UWR athletes. Data were recorded regarding general and health-related information, training habits, acute injuries that necessitated an interruption in training and/or doctor consultation, as well as overuse injuries. Overuse injuries were evaluated using the Oslo Sports Trauma Research Centre Overuse Injury Questionnaire. Statistical analyses included t tests or rank sum tests depending on normality of distribution. A nonparametric Kruskal-Wallis 1-way analysis of variance on ranks was used for nonnormally distributed data among several groups.
Results:
This study included 161 active athletes (mean ± SD, 36.1 ± 11.9 years old; 75.3% male) for analysis, of whom 90.1% were competing regularly. The performance-level distribution was as follows: first German national league (n = 73), second German national league (n = 46), state league (n = 17), district league (n = 1), and no league (n = 24). The mean ± SD sport-specific training workload was 5.6 ± 3.0 h/wk, including UWR training, additional swimming (n = 71; 44.1%), strength (n = 70; 43.5%), and/or endurance training (n = 102; 63.4%). Acute injuries were recorded in 78.9% of all athletes. The most typical locations for acute injuries were hand/finger (42.4%), head/face (concussion, ruptured eardrum; 18.1%), wrist (5.5%), or spine (5.0%). Overuse injuries were reported by 42.9% of the participants. The predominant locations for overuse injuries were hand/finger (18.8%), shoulder/clavicle (14.1%), spine and wrist (10.7% each), head/face (8.7%), and ankle joint and knee (6.7% each).
Conclusion:
In the current study, 3 of 4 athletes reported at least 1 acute injury, and 2 of 5 athletes reported at least 1 overuse injury. Leading injury regions were the hand/finger, head/ear, wrist, and spine.
Underwater rugby (UWR) is a team sport that originated in Germany in the 1960s and has since spread worldwide. 26,31 It is currently practiced in >30 countries. 6,26 International tournaments are regularly held, and since 1980 the World Championships have taken place every 4 years. The sport is governed by the Confédération Mondiale des Activités Subaquatique, which organizes international tournaments. With 79 UWR clubs registered, the Verband Deutscher Sporttaucher e.V. in Germany is the world’s largest national federation for the sport. There are first and second national leagues (Bundesliga) as well as state and district leagues. Most teams thereby compete with a mixed team (male and female). In addition, there is an all-women’s league at the first league level.
A UWR team consists of 15 players (6 players, 6 change players, and 3 reserve players). The changes take place on the fly via a substitution lane at the edge of the field. The playing field is 12 to 22 m long, 8 to 12 m wide, and 3.5 to 5 m deep, depending on the pool in which the game is played. The ball, which may be played only underwater, is filled with salt water so that it sinks in the pool. It has the shape and size of a handball. Players wear fins, diving masks, and snorkels. The goal of the game is to place the ball in the opponent’s basket. These baskets are located at the ends of the playing field and are attached to the bottom of the pool (Figure 1). 6,26,28,31

Underwater rugby training situation.
The game requires a high degree of strength, endurance, speed, and coordination. Intensive physical contact is inherent within the sport and may result in injury. Injury data in related water sports exist (eg, water polo 7,12 and swimming 13,29 ). Publications have cited a generally high injury prevalence in UWR, 16 as well as specific injuries in UWR—for example, hamate fractures of the ball-carrying hand 1,14,22 and an increased incidence of back pain. 11 Atilla et al 2 characterized injuries of master swimmers by using a questionnaire for athletes. This method appeared useful to provide an overview of injuries in a sport and was used as such in this study of UWR. There is a paucity of information relating to the general epidemiology of injury in UWR.
The purpose of this study was to examine the nature and prevalence of acute and overuse injuries in UWR. We hypothesized that acute injuries as well as overuse injuries are common in this high-contact sport, especially to the hands.
Methods
Study Design and Population
To assess common injury patterns and mechanisms of injury among active German UWR athletes, a web-based survey was designed by 4 of the authors (S.G., C.L., T.T., L.T.) and was pilot tested on 14 members of the German national UWR team. The protocol for this study received institutional review board approval, and all participating athletes provided informed consent. No financial compensation was provided in exchange for study participation.
Study Survey
The online platform SurveyMonkey (https://www.surveymonkey.com) was used to prepare the survey. Invitations to participate (and 1 reminder) were emailed to 48 sports clubs across 5 leagues within Germany. Assuming that club officials distributed the questionnaires to the athletes, about 720 athletes were contacted with the questionnaire. The survey (online from November 25, 2020, until March 15, 2021) included 32 to 111 questions (depending on the number of reported injuries) that covered various aspects regarding sports activity in training and competition and UWR-related injuries. A minimum requirement for completing answers was waived, as the study was opportunistic in terms of sample size and not driven by statistical testing.
For each athlete, general and health-related data were collected on age, sex, body size, preexisting conditions, and medication (n = 10 questions). This was followed by UWR-related questions (n = 14) on training load, experience, playing position, and performance level. The third section collected information on chronic overuse injuries of the sport (n = 9 questions). Overuse injuries were defined as chronic injuries without a singular causing event or a specific trauma that had developed during or after sport performance. The injury locations were categorized according to the Orchard Sports Injury Classification System (Version 10). 24 Multiple entries were possible. The German version of the Oslo Sports Trauma Research Centre (OSTRC) Overuse Injury Questionnaire was used to assess the severity of chronic injuries. 5 The OSTRC measure consists of 4 questions, each graded on a scale of 0 to 25, for a total score of 100 (0 = no problems, 100 = maximum level of problems). In addition, information was provided on the characteristics of the problem, the duration, and the type of therapy.
The fourth and last section dealt with acute injuries. Acute injuries were defined as injuries with a sudden onset during sport performance without a history of injury. Up to 4 acute injuries could be specified individually, with the same questions asked for each (n = 18 questions). These included type, circumstances, and consequences of the injuries and to what extent they were treated medically. Last, questions were asked about minor injuries that did not result in a break from training or medical treatment.
Statistical Analysis
Survey data were exported to Microsoft Excel; statistical analyses were performed using SigmaStat software (Systat Software Inc). Data were reported as mean, standard deviation, and range or as absolute values with percentages, as appropriate. Values were checked for normality with the Shapiro-Wilk test. To determine the difference between groups, a t test or rank sum test was used, depending on normal distribution. A nonparametric Kruskal-Wallis 1-way analysis of variance on ranks was used for nonnormally distributed data among several groups. Subgroup analyses were made for athletes of different performance levels as described. P < .05 was considered statistically significant.
Results
Study Population
A total of 161 athletes responded to the survey and were included in this analysis. This resulted in a response rate of 22.4% based on the assumption of approximately 720 contacted athletes. The mean time needed to answer all questions was 14 minutes. Among the 161 athletes surveyed, 119 were men and 39 were women (3 times no gender information was given). The ratio of male to female athletes was thus approximately 3 to 1. The mean ± SD age of the respondents at the time of the survey was 36.1 ± 11.9 years (range, 17-67 years). Of the 161 participants, 137 played in a league in Germany at the time of the survey (Figure 2), and all but 16 participants played regularly in tournaments. The study included 29 national team athletes.

Number of participants per underwater rugby league in Germany.
Details on the study population are shown in Table 1. On average, the respondents practiced UWR for 14.9 ± 10.8 years (range, 2-45 years). Most athletes stated training in a gender-mixed team setup (96.3%; n = 155). The remaining 3.7% (n = 6) of the respondents trained in all-male teams. Participants in women-exclusive or youth teams were not represented in the survey. In terms of warming up during UWR training, 77% (n = 124) reported doing so during swim-in, 10% (n = 16) warmed up before entering the water, and 13% (n = 21) did not warm up at all. The 3 playing positions (goal, defense, forward) were evenly distributed among the athletes: 58 defense, 54 goalkeeper, and 48 forward (1 no answer). Playing position did not influence the type of injury.
Demographics, Training, and Performance Level of Participants Overall and by Performance Level a

a Data are presented as mean ± SD (range) or No. M:F, male/female; NS, not significant; UWR, underwater rugby; Y:N, yes:no.
b Including UWR, swimming, strength, and endurance.
The training workload averaged 2.6 ± 1.1 h/wk (range, 1-7 h/wk) of UWR, with high-level athletes practicing significantly more (Table 1). Overall, participants reported 7.1 ± 4.5 h/wk (range, 1-33 h/wk) of sports. Including swimming, strength, and endurance training (but not other sports), national team athletes had a training workload of 7.0 ± 3.6 h/wk (range, 1-15.5 h/wk), whereas nonnational team athletes had a training workload of 5.3 ± 2.8 h/wk (range, 1-18 h/wk). National team athletes were significantly younger and competed significantly more often than the comparison group but did not differ in height, weight, and body mass index from the other players.
Acute Injuries
In total, 238 independent acute injuries were reported in 127 athletes. On average, 1.5 ± 1.1 injuries were reported per athlete (Figure 3). The majority (152 injuries) occurred during training and considerably less (n = 61) in tournaments. The upper extremity was most frequently affected by acute injuries (58%; 138 injuries), followed by the head/neck area (23%; 55 injuries). The lower extremity accounted for a much smaller proportion (7%; 17 injuries), and the trunk (4%; 10 cases) was also rarely affected (Figure 4). The 8 most common injury regions in terms of injury type and typical injury mechanisms were as follows: hand/finger/thumb (n = 101), head/face (n = 43), wrist (n = 13), neck/spine (n = 12), shoulder/clavicle (n = 11), ankle (n = 9), elbow (n = 8), and ribs/chest (n = 7).
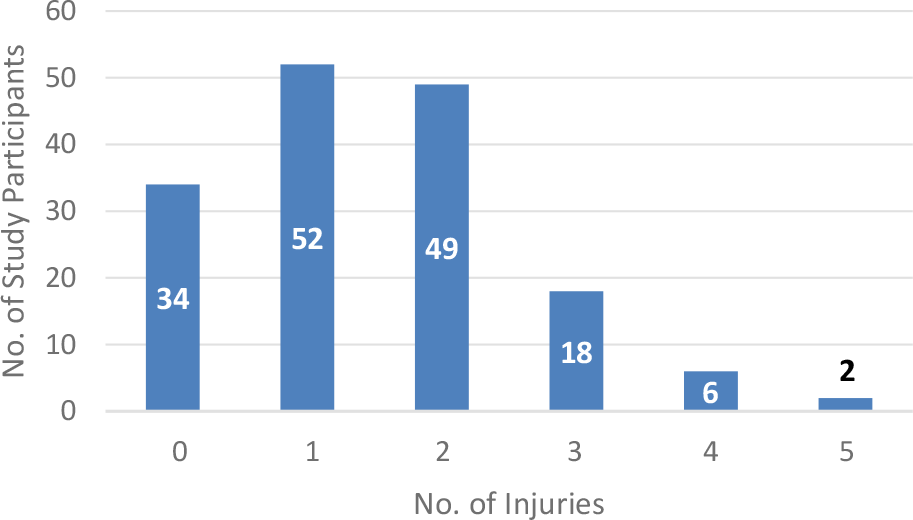
Total number of sustained acute injuries per person during career.

Distribution of acute (blue) and overuse injuries (purple). Numbers indicate the percentage of total injuries.
The most frequent injuries occurred to the hand, finger, and thumb. These were primarily capsular tears, followed by contusions/sprains and fractures (Figure 5). The players were more often in possession of the ball, and most injuries occurred while fighting for the ball. When this was not the case, it was usually hits by opponents’ fins that resulted in finger or thumb injuries.

Types of acute injuries of hand/fingers/thumb. *“Other” refers to injuries that do not match any of the specified groups (eg, to the fingernails).
Acute injuries to areas other than the hand are shown in Table 2. Head/face injuries were the second-most common entity and affected the ears in about 50% of cases. Mostly they were ruptured ear drums, caused by blows to the ears (eg, by fins). Concussions, cuts, or lacerations were also frequent. Those injuries mostly occurred during duels, except for 6 concussions and 1 laceration where the affected individuals had no contact with the opponent. Instead, the cause of injury was swimming with the head against a wall of the pool or against the basket.
Types of Acute Injuries by Body Region a

a Injuries to the hand, finger, and thumb are detailed in Figure 5.
b Including bursitis and epicondylitis.
Wrist injuries came third in the survey, and the most common entity was hamate fracture (Table 2). The cause of injury was known in 10 cases. In the majority (n = 7), there was direct opponent contact, and a blow to the wrist occurred either in the struggle for the ball or by the opponent’s foot or fin. In the remaining 3 cases, bumping the hand at the basket caused a fracture of the hamate bone.
Injuries of the neck/spine were documented with approximately the same frequency as wrist injuries. Most frequently, these were sprains (Table 2). Contact with an opponent was present in all those injuries. Shoulder injuries included dislocations, sprains, and others. A consistent mechanism of injury could not be found. The majority of injuries that affected the ankle were capsular or ligament tears. Eight of the 9 injuries resulted from direct force applied to the fin or ankle by an opponent. Elbow injuries included biceps tendon tears and joint irritation attributed to violent bruising of the elbow on the pool wall. Injuries to the ribs (fractures and contusions) were reported and mostly caused by kicks from opponents.
Further injury circumstances are shown in Table 3. In part, statistically significant differences were seen among the injury locations with respect to the circumstances surrounding the injury. It was significant such that in possession of the ball, the wrist was more likely to be affected by injuries as compared with injuries to the head. During an attack to the opponent’s basket, the number of wrist injuries was also significantly greater than those that affected the head.
Injury Circumstances and Injury Consequences of Common Acute Injuries

Data are presented as No. or mean ± SD (range). CT, computed tomography; MRT, magnetic resonance tomography; NS, not significant; Y:N, yes:no.
a-eSuperscript letters within a row indicate injury locations that were significantly different from each other (P < .05).
The most common hand/finger/thumb injuries resulted in the shortest training interruption, averaging 3.5 ± 4.3 weeks (range, 0-24 weeks). In contrast, wrist and elbow injuries were less common but had a significantly longer rest period, averaging 10.2 ± 4.2 weeks (range, 4-20 weeks) and 11.6 ± 16.3 weeks (range, 1-40 weeks), respectively. In the case of hand/finger/thumb injuries, hospitalization and surgical therapy were significantly less frequent, in contrast to wrist and elbow injuries.
Between national and nonnational team athletes, no differences were found in the frequencies, consequences, and circumstances of acute injuries, with 1 exception. Specifically, the proportion of injuries that occurred in competition was greater among national team athletes (Table 4). A comparison between first league players (n = 73) and all other study participants (n = 88) showed a higher rate of acute injuries in the first league. Those players also had consulted doctors more frequently after injuries (Table 5).
Comparison of Acute and Overuse Injuries Between German National and Nonnational Team Athletes a

a Data are presented as mean ± SD (range) or No. NS, not significant; OSTRC, Oslo Sports Trauma Research Centre.
b Dashes indicate areas not applicable.
Comparison of Acute and Overuse Injuries Between Athletes From the First German National League and the Other Athletes a
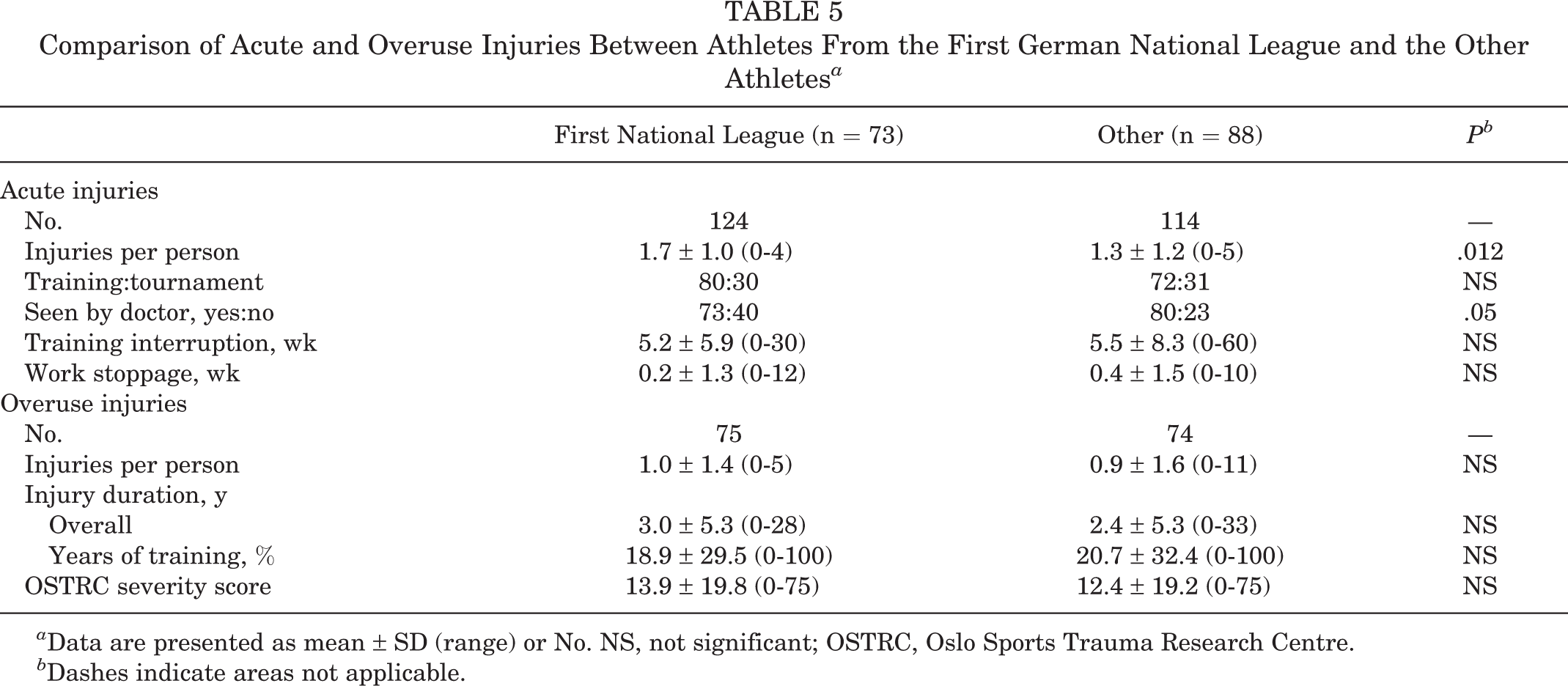
a Data are presented as mean ± SD (range) or No. NS, not significant; OSTRC, Oslo Sports Trauma Research Centre.
b Dashes indicate areas not applicable.
Overuse Injuries
In total, 149 independent overuse injuries were reported in 69 athletes. Most affected athletes reported such injuries in 1 or 2 body regions. More than half of the injuries (53%; 79 statements) involved the upper extremity (Figure 4). The hand, fingers, and thumb were most frequently affected. The injuries were attributed by the athletes to recurrent overextending, sprains, and bruises, which occurred in duels and sometimes resulted in slight capsule tears. Tapes to stabilize the finger joints were mostly used as a measure against this. Shoulder pain (second most mentioned) was frequently indicated after long days of play or strenuous training. Targeted strengthening and stability exercises were mentioned as the most common remedy against it. In third place were overuse injuries of the wrist, as well as the cervical spine. Neck pain was caused by frequent overstretching, strains, and sprains and was treated by many athletes with physiotherapy and stretching. Wrist pain was mostly load related and attributed to repetitive “minor” sprains or past traumatic events. Less than half of affected athletes stated that they used tapes and braces to stabilize the wrist. Chronic injuries in the area of the head primarily concerned the ears (inflammations, hearing loss, feeling of pressure) and headaches. The affected athletes related these partly to strenuous training while frequently needing to hold their breath and as a result of problems with the paranasal sinuses attributed to equalizing pressure. The cause of pain in the ankle joint was seen by the athletes as the load on the joints caused by the fins. The overload reactions of knees and elbows were unspecific.
On average, the overuse injuries had existed for 6.6 ± 6.5 years (range, 0.5-33 years). No significant differences could be identified in the injury duration of the 8 most frequent injury regions (Table 6). For the total of 161 participants in the survey, the mean OSTRC severity score was 13.2 ± 19.4 (0-75), and for the 69 respondents who reported at least 1 chronic injury symptom, the mean score was 21.5 ± 21.2 (0-75). OSTRC severity scores were not significantly different according to body region.
Overuse Injuries and OSTRC Severity Score by Commonly Affected Body Region a

a Data are presented as mean ± SD (range). OSTRC, Oslo Sports Trauma Research Centre.
bP value for comparison by body region.
The comparison of acute and overuse injuries showed significant differences for various injury locations. Head/face injuries, hand/finger/thumb injuries, and injuries to the ribs and chest occurred more often with an acute onset. Neck/spine injuries, shoulder injuries, as well as injuries to the knee or foot/toe were found significantly more often as overuse injuries (Table 7; Supplemental Tables S1 and S2, available separately). In the comparison of athletes with different performance levels, no differences could be found regarding overuse injuries (Tables 4 and 5).
Comparison of Acute and Overuse Injuries by Body Region a

a NS, not significant.
bP value for comparison of acute vs overuse injuries overall.
Discussion
The most important finding of the present study is that significantly more acute than overuse injuries were recorded (P < .001), mainly involving the upper extremity (58% of all acute injuries), especially the hands. As compared with other injury locations, hand/finger/thumb injuries were the least severe, causing the shortest training interruption (P < .001). Wrist injuries were much less frequent but more severe. These injuries occurred predominantly while the player was in possession of the ball (P = .001) and attacking the opponent’s basket (P = .01). Furthermore, head injuries (18.1% of all acute injuries) predominantly occurred during defense and without possession of the ball (P = .001). Additionally, overuse injuries in UWR were of minor severity. The upper extremity (53% of all overuse injuries), primarily hand and shoulder, was particularly affected. Finally, acute injuries were more common in the head, hands, and thorax, while cervical spine, shoulder, knee, and feet were more prone to chronic overuse injuries (P < .001).
The severity of all overuse injuries in UWR in this study averaged 21.5 points according to the OSTRC score. This is roughly in the same range as the severity of overuse injuries in ice hockey, with scores between 16.8 and 33.4. 4,19,20 Delfino Barboza et al 8 showed a severity score of 21 among field hockey athletes, which is comparable to that in the present study.
Ear injuries thereby have the greatest similarity to UWR injuries, as found in our study. In both sports, ear drum ruptures represented the leading type of injury. Protective caps are nowadays used in both sports, which seem to have a preventive effect, as shown in water polo. 7,12 Despite the protective caps, blows to the ears can cause perforation of the eardrum. In water polo, these blows are mostly caused by the hands of opponents, 12 whereas in UWR they were caused by fins. 9 In water polo, the head remains above the water surface, and the ball is thrown at speeds of 60 to 70 km/h, thus representing a risk of injury. 3,12 In UWR, the ball is passed underwater and not thrown and consequently did not cause any injuries in our study.
Teeth and eye injuries, which are frequent in water polo, were not found in our study. This difference could be explained by the different equipment used. In UWR, diving masks and snorkels are worn permanently. These can provide mechanical protection against impact and prevent contact of the eyes with the water. The latter is relevant because in water polo there is frequent irritation of the eye by chlorinated water and infections. 25 Several publications focusing on water polo found acute injuries mainly in the area of the head and face as well as the hands, while overuse injuries predominantly occurred around the shoulders. 7,12,17,25,27,30 In their recent meta-analysis, Croteau et al 7 identified head injuries as the most common acute injuries in water polo (period prevalence of 20.5-53%). In our study, head injuries represented the second most frequent location of injury in UWR (18.1% of all acute injuries). Primary injury types in water polo were contusions, concussions, cuts and fractures, and injuries to the teeth, eyes, and ears. In both sports, ear drum ruptures are a common type of injury.
In water polo, a typical region for chronic overuse injuries, as well as acute injuries, is the shoulder. In a 2018 meta-analysis, Miller et al 17 reported rates of 24% to 51% for shoulder pain and injury among male athletes. Croteau et al 7 also described a prevalence of 6% to 13.6% shoulder injuries in water polo. The combination of swimming and throwing movements in water polo has been cited as the cause of overuse injuries. The so-called swimmer’s shoulder occurs frequently as a symptom complex. 7,12,17 In UWR, shoulder pathologies accounted for only 14.1% of overuse injuries. One possible explanation is that UWR, in contrast to water polo, does not involve an actual throwing motion. The ball is passed underwater with a pushing motion; load on the shoulders from crawling movements is also rare in UWR, since most distances are performed underwater by pushing with the legs/fins alone.
In swimming, a relationship has been reported between training volume and incidence of shoulder pain in swimmers. 2,10 Freestyle and backstroke swimmers show the highest risk of shoulder injury. 23 In UWR, the shoulder was the second most frequently affected by overuse injuries (14.1% of all overuse injuries). Thus, these injuries occur significantly less frequently than in swimmers.
Regarding overuse injuries, however, any conclusions and comparisons with other sports such as swimming should be made with extreme caution, as exposure time in the niche sport of UWR is very low, even among competitive athletes. Training time of UWR players in the water is less than an hour per day and therefore significantly lower than that of swimmers, some of whom have training durations of 20 to 30 h/wk. 10,13 Fins used in UWR also increase propulsion from the legs, which in turn could result in less stress on the shoulders.
In swimmers, the knee is the second-most frequently affected region with regard to overuse injuries. 13,21 Injuries to the thorax, spine, and lower extremity occurred less frequently than the aforementioned injuries to the head and upper extremity in water polo and UWR. 7,18 Nevertheless, Fett et al 11 described an increased prevalence of back pain in both sports. However, this could not be confirmed in the present study. In water polo, pathologies of the hip and knee can be favored by the breaststroke movement of the legs. 7,12,25 Thus, tendinopathies and impingements may occur at the hip, while problems of the medial ligamentous apparatus (“breaststroker’s knee”) are prominent at the knee. 7,12 In UWR, knee complaints accounted for only 6.7% of overuse injuries. The reason for it could be that the problem of the breaststroker’s knee might not play a role. The swimming technique in UWR is most comparable to freestyle or dolphin swimming, for which one’s stroke is less often affected by knee pain. 13,29
The back represents a frequent region of chronic complaints in swimmers, 13,23,29 and increased degeneration of the intervertebral discs has been observed among swimmers. 15 A strong hyperextension of the lumbar spine during swimming has been discussed as the cause of the complaints. It can be observed especially in breaststroke and dolphin swimming. 29 The severity of these complaints has been associated with the amount of training. 11,15 Although the use of fins in UWR is considered a risk factor for chronic back pain, 29 no increased injuries in the area of the thoracic or lumbar spine were found in this study.
Other literature on UWR concerned hamate fractures. Direct application of force to the palmar wrist on impact against the metal basket is one cause of fracture. Repeated traumatic events by opposing players against the dorsum of the hand are another cause. 14,22 These mechanisms of injury are consistent with the descriptions in the present study. In 2001, Andresen et al 1 published a case report of a professional UWR player with a hamate fracture sustained during a match. An increased incidence of those fractures in UWR was identified in 2011 by Kamusella et al 14 with 7 players. Scheufler et al 22 came to the same conclusion in 2013. In all cases, the ball-carrying right hand was affected by the injury. This is maximally inflected during ball control. 1,14,22 In the present study, 8 fractures of the carpal bones were recorded, 7 of them hamate fractures (in 1 fracture, the affected bone was unknown).
The knowledge gained from this study can help to establish prevention concepts in the future. For the most commonly injured regions, prevention concepts can include training programs for finger and wrist stabilization, prohibition of reaching into the opponent’s fingers, or tightening of rules regarding head/neck contact.
Limitations
This study is not without limitations. First, when evaluating the data, one should note that a niche sport was studied in which only provisional professional structures exist; furthermore, the training volumes vary greatly from individual to individual and are considerably lower than in other sports. High-level athletes from this survey trained more than the comparison group but still little as compared with competitive athletes in other sports. Second, based on the assumption that all contacted teams really distributed the questionnaire to their athletes, the response rate is relatively low. Third, the data of the study were provided by the athletes themselves; as such, exact information is missing—for example, on injury entities—and the differentiation between acute and overuse injuries was sometimes problematic. The OSTRC severity score was collected only once so that an approximate statement could be made about the degree of severity of overuse injuries. For an exact statement, however, monitoring of the athletes over a longer period would be necessary. Other potential risks underwater, such as drowning or near drowning, were not investigated in this study but need to be considered, even though we are not aware of such cases. Despite the limitations, the study shows a good systematic overview of typical injuries occurring in UWR.
Conclusion
The present study on athletes of different performance levels analyzes the distribution of injuries in UWR, with 3 of 4 athletes reporting at least 1 acute injury and 2 of 5 athletes reporting at least 1 overuse injury. Leading injury regions are hand/finger, head/ear, wrist, and cervical spine. Sport-specific awareness training programs for noncompetitive and competitive UWR athletes to reduce burden of injury should be developed, and sports medical supervision is mandatory. The knowledge gained can help to establish prevention concepts in the future.
Supplemental material for this article is available at https://journals.sagepub.com/doi/full/10.1177/23259671231181582#supplementary-materials
Supplemental Material
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671231181582 - Epidemiology of Acute and Overuse Injuries in Underwater Rugby
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671231181582 for Epidemiology of Acute and Overuse Injuries in Underwater Rugby by Christoph Lutter, Sina Gräber, Gareth Jones, Justus Groß, Lukas Tadda and Thomas Tischer in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted February 5, 2023; accepted March 9, 2023.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from University Medical Center Rostock (No. A2020-0267).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.