
Abstract
Background:
To date, there is a scarcity of literature related to the incidence of prolonged stiffness after an anterior cruciate ligament (ACL) tear that requires manipulation under anesthesia/lysis of adhesions (MUA/LOA) in the preoperative period before ACL reconstruction (ACLR) and how preoperative stiffness influences outcomes after ACLR.
Hypothesis:
Preoperative stiffness requiring MUA/LOA would increase the risk for postoperative stiffness, postoperative complications, and the need for subsequent procedures after ACLR.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
The PearlDiver Research Program was used to identify patients who sustained an ACL tear and underwent ACLR using their respective International Classification of Diseases, 9th or 10th Revision, and Current Procedure Terminology (CPT) codes. Within this group, patients with preoperative stiffness were identified using the CPT codes for MUA or LOA. Significant risk factors for preoperative stiffness were identified through univariate and multivariate logistic regression analyses. Outcomes after ACLR were analyzed between patients with and without preoperative stiffness using multivariate logistic regression, controlling for age, sex, and Elixhauser Comorbidity Index.
Results:
Between 2008 and 2018, 187,071 patients who underwent ACLR were identified. Of these patients, 241 (0.13%) underwent MUA/LOA before ACLR. Patients with preoperative stiffness began preoperative physical therapy significantly later than patients without stiffness (P = .0478) and had a delay in time to ACLR (P = .0003). Univariate logistic regression demonstrated that female sex, older age, anxiety/depression, obesity, and anticoagulation use were significant risk factors for preoperative stiffness (P < .05 for all). After multivariate regression, anticoagulation use was the only independent risk factor deemed significant (odds ratio, 6.69 [95% CI, 4.01-10.51]; P < .001). Patients with preoperative stiffness were at an increased risk of experiencing postoperative stiffness, deep vein thrombosis, pulmonary embolism, surgical-site infection, and septic knee arthritis after ACLR (P < .05 for all).
Conclusion:
Although the risk of preoperative stiffness requiring an MUA/LOA before ACLR is low, the study findings indicated that patients with preoperative stiffness were at increased risk for postoperative complications compared with patients with no stiffness before ACLR.
As sports participation has increased, injuries to the anterior cruciate ligament (ACL) and subsequent ACL reconstruction (ACLR) have mirrored such trends. 1 With the advancement of arthroscopic instrumentation, techniques, and postoperative rehabilitation, the majority of patients undergoing ACLR are extremely satisfied after surgery and are able to return to their preoperative sporting activities at high rates. 18 Nevertheless, a small percentage of patients may experience complications after ACLR requiring further surgical intervention. In a study by the Multicenter Orthopaedic Outcomes Network (MOON) Group, 9 apart from revision ACLR and subsequent cartilage procedures, arthrofibrosis was the most common complication requiring a return to the operating room. While the definition of arthrofibrosis varies widely in the literature, patients experiencing arthrofibrosis commonly have complaints of knee stiffness, pain, decreased range of motion (ROM), and decreased function. 4 Previous studies have demonstrated the incidence of arthrofibrosis to vary widely, with 4% to 38% of patients experiencing stiffness in the postoperative period. 4,9,14,15,20,21 While the incidence has declined over time, postoperative stiffness is a serious complication after ACLR, resulting in increased costs, prolonged physical therapy (PT), need for subsequent procedures, decreased patient satisfaction, and worse functional outcomes. 4,9,14,15,20,21
Given the deleterious effects of stiffness after ACLR, there have been great efforts to identify high-risk patients preoperatively and subsequently perform early targeted interventions to both prevent and treat such patients in a timely manner. Previous studies have demonstrated that one of the most significant risk factors for postoperative stiffness is decreased preoperative knee ROM. 2,13,15 –17,20,21 However, there have been few studies investigating the risk factors and influence of prolonged preoperative stiffness on the time to ACLR, the need for an intervention to address the preoperative stiffness, and the outcomes after ACLR in patients who experience prolonged preoperative stiffness.
We addressed these shortcomings in the present study by investigating the risk factors for prolonged stiffness before ACLR that requires arthrolysis in a nationally representative sample. Furthermore, we investigated the effect of stiffness in the preoperative period on patient complications after ACLR, including postoperative stiffness, prolonged postoperative opioid medication use, medical complications, and the need for subsequent operative interventions. We hypothesized that delayed presentation to PT, female sex, history of psychiatric illness, and anticoagulation use would be risk factors for stiffness in the pre- and postoperative period. Additionally, we hypothesized that the need for an arthrolysis procedure before ACLR would increase the risk of postoperative stiffness, infection, medical complications, revision surgery, and prolonged opioid use.
Methods
Data Source
The PearlDiver Patient Record Database (PearlDiver Inc) was utilized for this study. PearlDiver is a publicly available and Health Insurance Portability and Accountability Act–compliant national database that includes both inpatient and outpatient medical records of adult and pediatric patients drawn from Humana and United Healthcare insurance claims as well as government claims from Medicare and Medicaid. Records within the database comprise procedures defined by Current Procedure Terminology (CPT) codes and diagnoses defined by the International Classification of Diseases, 9th Revision, (ICD-9), and 10th Revision, (ICD-10). Individual patients within the database can be followed through time using these records. Descriptive characteristics of age and sex are also available for each patient.
Study Cohort
The private insurance, Medicare, and Medicaid plans in the PearlDiver database were queried for 10 years between 2008 and 2018, capturing approximately 144 million patients. Patients who underwent ACLR were identified with the respective first-instance CPT codes (Supplemental Table S1, available separately). Their date of ACL injury diagnosis was recorded as identified by ICD-9 and ICD-10 codes. Patients were excluded if they had associated diagnoses or underwent other surgical interventions, including patients with a previous history of ACLR, concomitant posterior cruciate ligament reconstruction (CPT code 29889), posterolateral reconstruction (CPT code 27427), extra-articular augmentation techniques (CPT 27427), microfracture (CPT code 29879), osteochondral autograft or allograft transfer (CPT code 29866 or 29867), meniscal transplant (CPT code 29868), open collateral ligament reconstruction (CPT code 27427), high tibial osteotomy (CPT code 27457), and femoral osteotomy (CPT code 27488). Laterality of ACLR was noted via associated ICD-10 codes for ACL tear on the date of surgery. Included in the study were patients who underwent concomitant ipsilateral meniscal surgery at the time of initial ACLR, including meniscal repair and meniscectomy, as specified by the associated CPT codes.
Patients with pre- or postoperative stiffness were identified using CPT codes as those who required manipulation under anesthesia (MUA) or lysis of adhesions (LOA). Preoperative stiffness was defined as MUA/LOA within a year before ACLR and postoperative stiffness was defined as MUA/LOA within a year after ACLR.
Risk Factors for Preoperative Stiffness
A panel of candidate variables were considered possible risk factors for pre- and postoperative stiffness and identified using ICD/CPT codes (Supplemental Table S1). This included patient age, sex, insurance type, concomitant meniscal procedures, anxiety, depression, obesity (body mass index [BMI], ≥30), oral contraceptive use, preoperative opioid use, and anticoagulation use. The times between ACL injury, ACLR, MUA/LOA, and PT sessions were recorded. We determined the time to PT by calculating the time between ACL injury diagnosis and the first PT billing CPT code. Opioid use was specified by whether there was a record for filling an opioid prescription. Preoperative opioid use was recorded if the patient had filled an opioid prescription in the month before surgery.
Postoperative Outcomes
To determine how preoperative stiffness influences outcomes in patients undergoing ACLR, the following complications were investigated: postoperative stiffness requiring MUA/LOA, prolonged opioid use, need for revision ACLR, need for ipsilateral subsequent or revision meniscal procedures, medical complications (pulmonary embolism [PE] and deep vein thrombosis [DVT]), and deep or superficial infection. The laterality of the meniscal procedure was noted via ICD-10 codes for meniscal injury coded on the date of the meniscal procedure (Supplemental Table S2). Postoperative opioid use was assessed at 1-, 3-, 6-, and 12-month time points, with use for >3 months considered to be prolonged. 7,10,19
Statistical Analysis
The study cohort was divided into patients without preoperative stiffness and those with preoperative stiffness who required MUA/LOA before ACLR. Data were recorded as absolute values and percentages or medians and interquartile ranges (IQRs) (defined as the difference between the 75th and 25th percentiles of the data). The chi-square analysis was used to compare the proportion of each group that underwent concomitant meniscal procedures. The time between the initial PT session before or after ACLR and the time between the ACL injury and ACLR were compared between groups using the 2-sample Student t test. Significant risk factors for preoperative stiffness were identified through univariate logistic regression analysis for each candidate risk factor. Multivariate logistic regression was then utilized to assess for independent risk factors using the variables found to be significant on univariate analysis (P < .05). The odds ratio (OR) for outcomes was estimated using multivariate logistic regression, controlling for age, sex, and Elixhauser Comorbidity Index. Statistical analysis was performed using the PearlDiver software, built on RStudio Version 1.1.442 (RStudio Inc). An α value of .05 was set as the level of significance.
Results
Between 2008 and 2018, 187,071 patients who underwent ACLR were identified. Of these patients, 241 (0.1%) and 2651 (1.4%) required an arthrolysis procedure before or after ACLR, respectively (Table 1). A large proportion of the patients included in the study were 15 to 24 years of age, accounting for 41% of the included patients. Females were more likely to have preoperative stiffness than males (57.3% vs 42.7%, respectively; P < .0001). At the time of ACLR, 16.0% of the patients without preoperative stiffness had a meniscal repair and 48.2% had a meniscectomy, whereas 7.1% of the patients with preoperative stiffness had a meniscal repair and 28.6% had a meniscectomy (P < .0001) (Table 1).
Study Cohorts Undergoing ACLR a
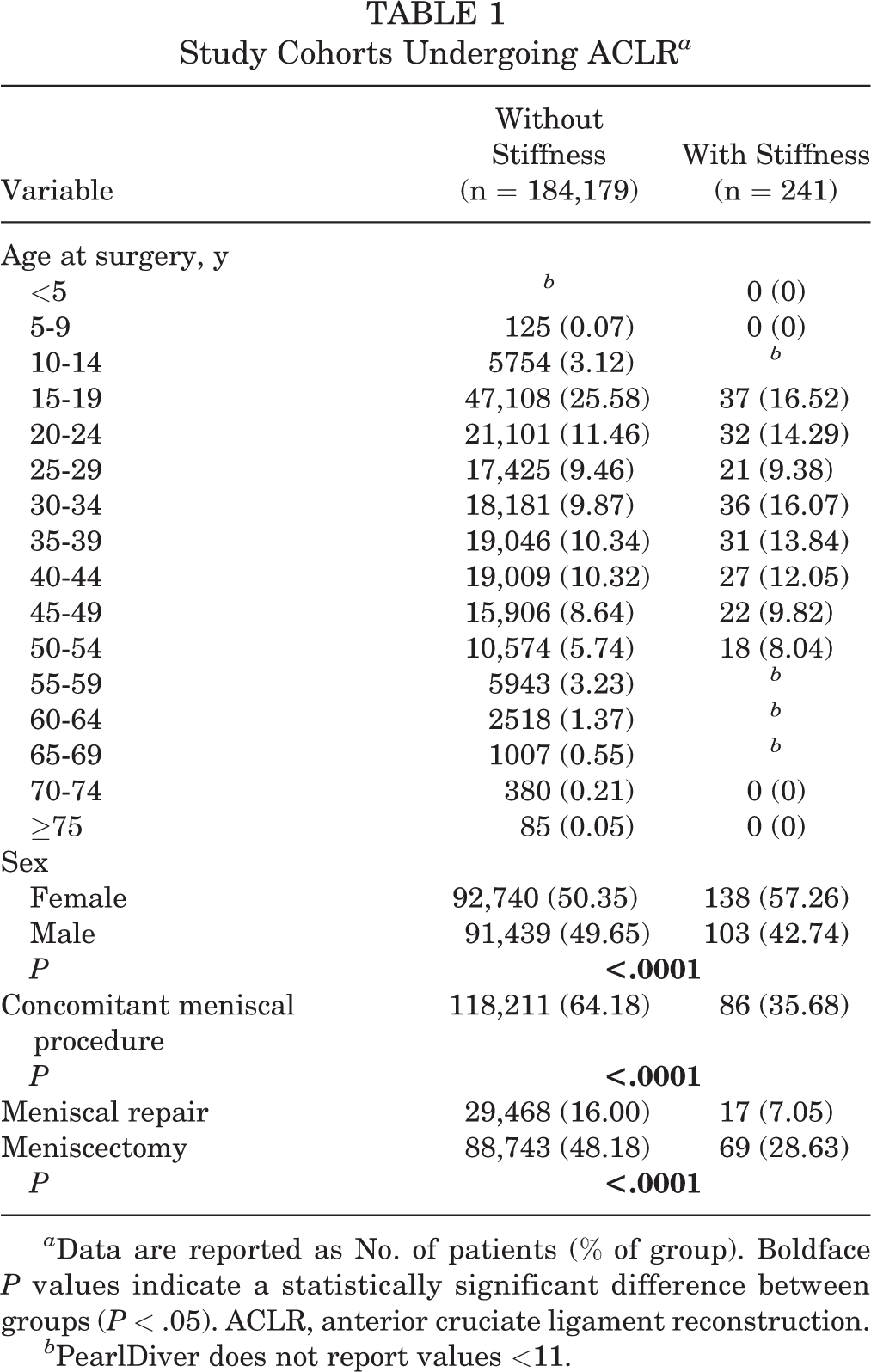
a Data are reported as No. of patients (% of group). Boldface P values indicate a statistically significant difference between groups (P < .05). ACLR, anterior cruciate ligament reconstruction.
b PearlDiver does not report values <11.
Risk of Preoperative Stiffness by Time to Rehabilitation and ACLR
Patients with preoperative stiffness presented to PT significantly later than patients without stiffness (median [IQR], 38.5 days [214.5 days] vs 31 days [60.0 days], respectively; P = .0478) (Table 2). Furthermore, patients with stiffness had a significantly longer time from ACL tear diagnosis to ACLR compared with patients without stiffness (median [IQR], 129.5 days [165.3 days] vs 34 days [59 days]; P = .0003).
Time Between ACL Tear Diagnosis, MUA/LOA, ACLR, and First PT Session a

a Data are reported as median [IQR]. Boldface P values indicate a statistically significant difference between groups (P < .05). ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction; MUA/LOA, manipulation under anesthesia/lysis of adhesions; NA, not applicable; PT, physical therapy.
Risk Factors for Preoperative Stiffness Requiring MUA/LOA
Univariate regression analysis demonstrated that patients with preoperative stiffness were more likely to be female (57.3% vs 50.4% in patients without stiffness; OR, 1.32 [95% CI, 1.01-1.69]; P = .0390) (Table 3). Increasing age was also a significant risk factor, with each additional year associated with a 1% increase in the risk of preoperative stiffness (OR, 1.01 [95% CI, 1.00-1.02]; P = .0181). Anxiety (OR, 1.61 [95% CI, 1.15-2.21]; P = .0039), depression (OR, 1.53 [95% CI, 1.11-2.11]; P = .0092), and obesity (OR, 1.62 [95% CI, 1.12-2.29]; P = .0082) were also associated with an increased risk for preoperative stiffness. Markedly, anticoagulation use increased the risk for preoperative stiffness by 8-fold (OR, 8.09 [95% CI, 4.89-12.6]; P < .0001). Patients with preoperative stiffness were less likely than those without stiffness to require a concomitant meniscal procedure at the time of ACLR (OR, 0.35 [95% CI, 0.27-0.45]; P < .0001). Insurance type, oral contraceptive use, and opioid medication use were not associated with preoperative stiffness.
Risk Factors for Preoperative or Postoperative Stiffness Requiring MUA/LOA a
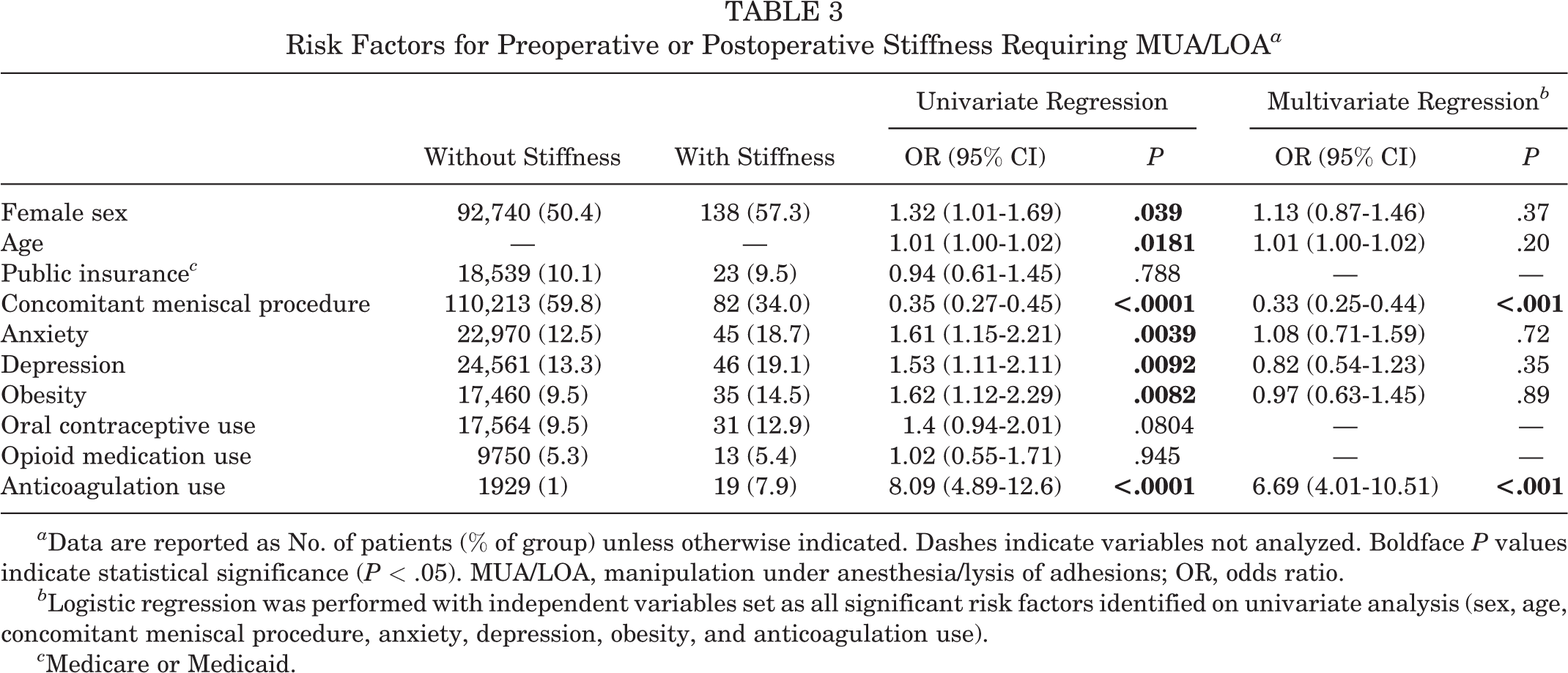
a Data are reported as No. of patients (% of group) unless otherwise indicated. Dashes indicate variables not analyzed. Boldface P values indicate statistical significance (P < .05). MUA/LOA, manipulation under anesthesia/lysis of adhesions; OR, odds ratio.
b Logistic regression was performed with independent variables set as all significant risk factors identified on univariate analysis (sex, age, concomitant meniscal procedure, anxiety, depression, obesity, and anticoagulation use).
c Medicare or Medicaid.
Multivariate logistic regression assessing the significant variables on univariate analysis revealed that only anticoagulation use increased the risk for preoperative stiffness (OR, 6.69 [95% CI, 4.01-10.51]; P < .001). Additionally, patients with preoperative stiffness remained less likely than patients without stiffness to require a concomitant meniscal procedure at the time of the ACLR (OR, 0.33 [95% CI, 0.25-0.44]; P < .001) (Table 3).
Outcomes After ACLR
Patients with preoperative stiffness had a higher risk of postoperative stiffness requiring MUA/LOA (OR, 3.34 [95% CI, 1.71-5.82]; P < .0001), DVT (OR, 3.57 [95% CI, 1.04-8.98]; P = .0179), PE (OR, 4.94 [95% CI 1.51-11.8]; P = .0018), superficial infection (OR, 4.50 [95% CI, 2.36-7.75]; P < .0001), and septic arthritis of the knee (OR, 4.00 [95% CI, 1.42-8.75]; P = .0022) compared with patients without preoperative stiffness (Table 4). However, there was no observed increased risk of ACLR revision or subsequent ipsilateral meniscal procedure.
Complication Rates After ACLR When Patients Underwent MUA/LOA Before or After ACLR a
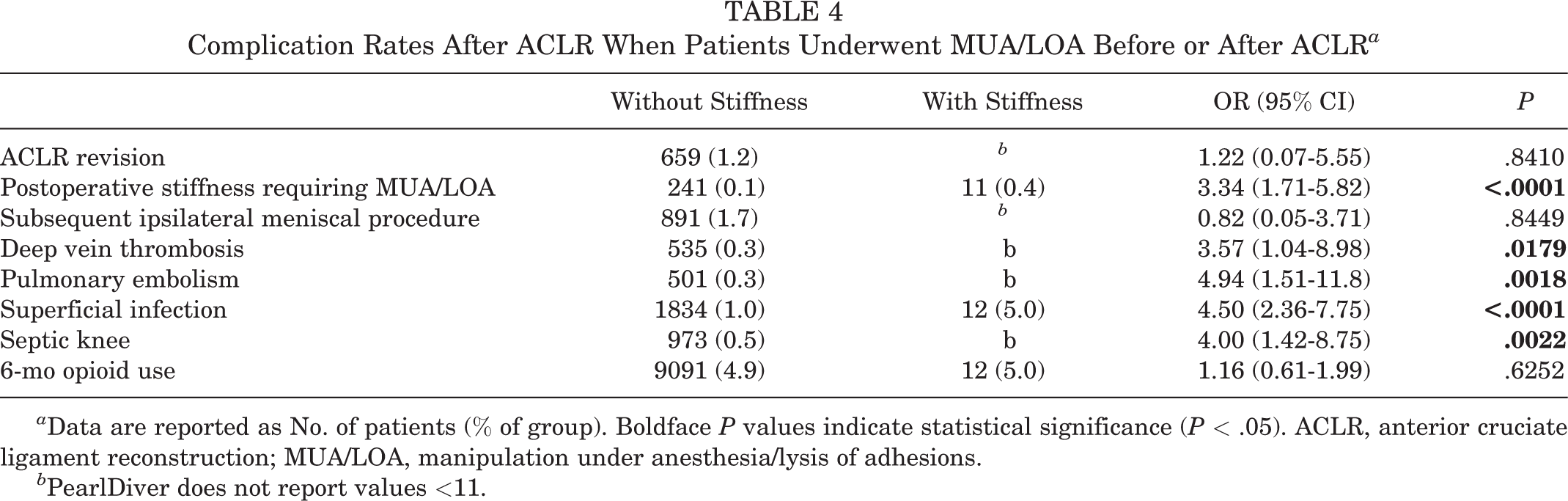
a Data are reported as No. of patients (% of group). Boldface P values indicate statistical significance (P < .05). ACLR, anterior cruciate ligament reconstruction; MUA/LOA, manipulation under anesthesia/lysis of adhesions.
b PearlDiver does not report values <11.
Discussion
The present study sought to investigate the prevalence and risk factors for stiffness after injury to the ACL that required preoperative MUA/LOA and, furthermore, the association between preoperative MUA/LOA and patient complication rates after ACLR in a large, nationally representative database. We found that despite the prevalence of preoperative MUA/LOA among ACLR patients being low, at 0.13%, notably, these patients were at increased risk for complications after their ACLR, including postoperative stiffness, DVT, PE, superficial infection, and septic knee arthritis. Univariate analysis demonstrated delayed presentation to PT, female sex, increasing age, anxiety, depression, obesity, and anticoagulation use to be associated with an increased risk of preoperative stiffness; however, only anticoagulation use was found to be an independent risk factor after multivariate analysis.
The timing of ACLR, need for prehabilitation, and preoperative benchmarks before ACLR have been frequently studied and debated topics. The consensus among most high-volume ACL surgeons is that one must have a “quiet knee” before ACLR, which is characterized by minimal pain, full knee ROM, and symmetric strength, which have been shown to be associated with improved short- and long-term outcomes after ACLR. 3,5,8,9,12 There have been little data to identify which patients are at increased risk for prolonged recovery after ACL injury and will require increased time to minimize their pain and obtain full ROM before undergoing ACLR. In the present study, we evaluated the most severely affected patients who ultimately required an MUA/LOA before ACLR to regain acceptable ROM before ACLR.
One of the most important findings in this study is that patients who required MUA/LOA preoperatively had a significant delay between their injury diagnosis and first presentation to PT for prehabilitation at a median of 38.5 days, >1 week later than patients who did not have preoperative stiffness. This finding highlights the importance of early diagnosis and a quick referral to an athletic trainer or physical therapist who specializes in prehabilitation before ACLR. Since many patients may first be evaluated by providers who are not orthopaedic surgeons, it is prudent that all providers be familiar with the presentation and clinical diagnosis of an ACL tear so they can begin early rehabilitation if there is concern for stiffness, rather than waiting for the athlete to be evaluated by one’s surgeon and obtain magnetic resonance imaging (MRI), which often can happen on a delayed basis. Our data also demonstrate that undergoing an MUA/LOA to address stiffness before ACLR was associated with a delay in the time to ACLR, with the median time from ACL tear diagnosis to ACLR being 129.5 days compared with 34 days in patients without preoperative stiffness.
Patient-specific risk factors that increased the risk of preoperative stiffness were female sex, older age, anxiety/depression, obesity, and anticoagulation use. However, multivariate analysis demonstrated that anticoagulation use was the only independent risk factor. Similar findings have been demonstrated by the MOON Group, who observed that female sex, increased BMI, and older age were all associated with prolonged recovery after ACL injury and increased pain at the time of ACLR. 3 In contrast to our findings, Gage et al 6 evaluated the factors associated with a delay (>3 weeks) in achieving full knee extension after an ACL injury, demonstrating bone bruising of the lateral femoral condyle to be the only significant risk factor. While increased BMI approached statistical significance, they did not observe age or sex to influence the risk of a prolonged inability to achieve full knee extension before ACLR. However, it is important to note that the Gage et al study included a much smaller sample size and may have not been powered enough to detect statistical significance for the variables of interest. Furthermore, the patients included in that study obtained care earlier after the index injury, at a mean of 7.8 days, and likely also began prehabilitation earlier, thus decreasing the risk for prolonged stiffness.
Postoperative anticoagulation use has been previously identified as a risk factor for increased stiffness after ACLR, likely because of formation of a postoperative hematoma as demonstrated by Malahias et al. 11 Our study found that the use of anticoagulation increased the risk of preoperative stiffness 8-fold. While further research is needed to elucidate the mechanism associated with this observed risk, it may be hypothesized that anticoagulation use increases the risk of hemarthrosis and hematoma formation after the initial injury. The resulting hemarthrosis likely results in the accumulation of inflammatory mediators resulting in prolonged inflammation that may initiate and propagate scar tissue formation leading to arthrofibrosis. 11 These findings suggest that physicians should be extremely vigilant when managing patients on anticoagulation and emphasize the importance of aggressive early ROM exercises after ACL injury to decrease the chance of preoperative stiffness. Future research should aim to better understand this modifiable risk factor, including the different risk profiles of the various types of anticoagulation and whether short-term cessation of these medications after injury can decrease one’s risk of stiffness without increasing the risk for DVT or PE. Another potential intervention in these patients that deserves further investigation is the use of tranexamic acid at the time of MUA/LOA and ACLR, which may theoretically reduce hemarthrosis and subsequent stiffness.
The finding that preoperative stiffness increases the risk of complications such as postoperative stiffness, DVT, PE, superficial infection, and septic arthritis underscores the importance for prehabilitation and the screening of patients at risk of stiffness after their ACL tear. Markedly, preoperative stiffness increased the risk of DVT and PE nearly 4-fold and 5-fold, respectively. The pathophysiology behind this is unclear, and patients who develop arthrofibrosis may represent a phenotype with an exaggerated inflammatory response to any type of insult (ie, injury or surgery), which could explain the development of arthrofibrosis and DVT/PE. However, this is speculative, and further research is needed.
Patients with preoperative stiffness may also experience decreased mobility, leading to increased stasis and coagulation. Another possible explanation would be that multiple surgical procedures in a short time frame increase the risk of DVT or PE. It is not surprising that patients who underwent preoperative MUA/LOA were 4.5 and 4 times more likely to experience superficial infection and septic arthritis, respectively, as a previous surgical procedure increases the risk for contamination at the initial MUA/LOA and infection after ACLR. Additionally, while only 0.4% of patients who underwent MUA/LOA before their ACLR also experienced postoperative stiffness that required MUA/LOA, logistic regression demonstrated that this cohort of patients was at 3 times the risk for postoperative MUA/LOA compared with their counterparts without stiffness. However, it remains unclear if the rate of postoperative MUA/LOA would have been even higher if these patients did not undergo MUA/LOA before ACLR. Future prospective research is needed to determine if MUA/LOA before ACLR is an effective treatment method to reduce the risk of stiffness after ACLR.
Another interesting finding in the present study is that patients who required a preoperative MUA/LOA were less likely to undergo both meniscectomy and meniscal repair at the time of their ACLR compared with the cohort of patients who did not develop preoperative stiffness. While the present study is limited by the inability to determine the relationship between the presence of a meniscal injury and the individual surgeon’s decision-making process when determining how to address these concomitant injuries, one possible explanation is that the inflammatory environment about the knee responsible for causing stiffness may also promote the healing of more peripheral meniscal tears that occurred at the time of injury. Alternatively, it is possible that the treating surgeons chose not to address any meniscal pathology in patients with preoperative stiffness at the time of their ACLR because of the known risk of stiffness after ACLR in patients undergoing a concomitant meniscal procedure, which could potentiate the risk that preoperative stiffness has on stiffness after ACLR. A final explanation may be that patients who experienced preoperative stiffness were less likely to participate in strenuous physical activity before ACLR because of their disabling stiffness and therefore were less likely to sustain further meniscal injury.
Limitations
This study is not without limitations. As with any database study, our data are dependent on accurate coding and diagnosis by providers and health care administrators. For example, it is possible that patients in this study have been given a diagnosis of anxiety or depression but have not undergone formal evaluation by a mental health specialist. Furthermore, the timing of injury and interventions, such as PT and MUA/LOA, relied on the dates on which the diagnosis or procedures were entered, and therefore our data may slightly over- or underestimate the time between ACL injury and formal diagnosis, first presentation to PT, and surgical intervention. Additionally, the database did not provide information on patients’ ROM pre- or postoperatively. Therefore, we were unable to determine each surgeon’s indications to perform an MUA/LOA before ACLR or the degree of ROM improvement after these interventions.
Furthermore, the PearlDiver database does not give information on the credentials and experience of the treating physicians, the type and source of graft used (eg, autograft vs allograft, hamstring tendon, quadricep tendon, bone–patellar tendon–bone, iliotibial band, etc), the technique used for reconstruction, or the rehabilitation protocols used by the treating providers pre- and postoperatively, all of which are important factors related to ACL injuries and reconstruction. In addition, we were unable to control for various patient- and injury-related factors that could alter the risk for stiffness, ACLR failure, and postoperative complications, including baseline activity level, sports participation, return-to-play time, anatomical risk factors (tibial slope, ligamentous laxity, and mechanical alignment), and injury-specific risk factors (degree and presence of bone bruising on MRI). Furthermore, we were not able to determine the mechanism of injury (ie, high-energy vs low-energy injury, acute injury vs chronic ACL insufficiency) for each patient included in the study. For example, someone with a high-energy injury may not only be at risk for early stiffness because of the nature of their injury, but also be at an increased risk for delayed diagnosis or appropriate referral if they have concomitant injuries that are more imminent. This could explain the observed delay in presentation to preoperative PT. However, we attempted to limit such confounders by not including patients who had concomitant injuries suggesting a high-energy mechanism, such as posterolateral corner and collateral ligament injuries.
Despite these limitations, we believe that the use of the large national-level database permitted the analysis of a sufficient number of patients to elucidate risk factors for pre- and postoperative stiffness and better describe their impact on outcomes after ACLR that would otherwise be very difficult to study using data from a single institution because of the low prevalence of recalcitrant stiffness, which requires MUA/LOA before ACLR. Furthermore, the variability in the studied patient cohort is likely more representative of national practice trends and eliminates the bias observed in single-institution academic practices.
Conclusion
We evaluated the prevalence, risk factors, and complications in patients who have severe and prolonged preoperative stiffness requiring MUA/LOA before ACLR. Anticoagulation use at the time of ACL injury was identified as a significant independent risk factor for preoperative stiffness requiring MUA/LOA. Our study highlights the importance of early injury diagnosis and subsequent referral to PT for prehabilitation to prevent stiffness and ensure that patients undergo ACLR promptly. Future prospective research is required to determine targeted treatment modalities to address modifiable risk factors for prolonged stiffness, such as anticoagulation use, in addition to further elucidating the indications and effectiveness of MUA/LOA before ACLR in patients with recalcitrant stiffness for whom nonoperative therapy fails.
Supplemental material for this article is available at https://journals.sagepub.com/doi/full/10.1177/23259671231181371#supplementary-materials
Supplemental Material
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671231181371 - Risk Factors and Outcomes for Preoperative Stiffness Requiring Intervention Before Anterior Cruciate Ligament Reconstruction
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671231181371 for Risk Factors and Outcomes for Preoperative Stiffness Requiring Intervention Before Anterior Cruciate Ligament Reconstruction by Nicholas J. Lemme, Daniel S. Yang, Rachel Talley-Bruns, Daniel Alsoof, Alan H. Daniels, Logan Petit and Paul D. Fadale in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted February 7, 2023; accepted March 9, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: R.T.-B. has received education payments from Smith & Nephew. A.H.D. has received fellowship support from OrthoFix; consulting fees from EOS, Medtronic, OrthoFix Medical, Davol, Spineart USA, Medicrea USA, Southern Spine, and Stryker; nonconsulting fees from OrthoFix Medical and Medicrea USA; royalties from Spineart USA and Medicrea USA; and a charitable contribution from Southern Spine. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.