
Abstract
Background:
Studies to date comparing biceps tenodesis methods in the setting of concomitant rotator cuff repair (RCR) have demonstrated relatively equivalent pain and functional outcomes.
Purpose:
To compare biceps tenodesis constructs, locations, and techniques in patients who underwent RCR using a large multicenter database.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A global outcome database was queried for patients with medium- and large-sized tears who underwent biceps tenodesis with RCR between 2015 and 2021. Patients ≥18 years of age with a minimum follow-up of 1 year were included. The American Shoulder and Elbow Surgeons, Single Assessment Numeric Evaluation, visual analog scale for pain, and Veterans RAND 12-Item Health Survey (VR-12) scores were compared at 1 and 2 years of follow-up based on construct (anchor, screw, or suture), location (subpectoral, suprapectoral, or top of groove), and technique (inlay or onlay). Nonparametric hypothesis testing was used to compare continuous outcomes at each time point. The proportion of patients achieving the minimal clinically important difference (MCID) at the 1- and 2-year follow-ups were compared between groups using chi-square tests.
Results:
A total of 1903 unique shoulder entries were analyzed. Improvement in VR-12 Mental score favored anchor and suture fixations at 1 year of follow-up (P = .042) and the onlay tenodesis technique at 2 years of follow-up (P = .029). No additional tenodesis comparisons demonstrated statistical significance. The proportion of patients with improvement exceeding the MCID did not differ based on tenodesis methods for any outcome score assessed at the 1- or 2-year follow-up.
Conclusion:
Biceps tenodesis with concomitant RCR led to improved outcomes regardless of tenodesis fixation construct, location, or technique. A clear optimal tenodesis method with RCR remains to be determined. Surgeon preference and experience with various tenodesis methods as well as patient clinical presentation should continue to guide surgical decision-making.
Tendinitis of the long head of the biceps rarely occurs in isolation. 1 Murthi et al 14 found that 91% of shoulders with significant biceps degeneration had concomitant rotator cuff tears. Biceps tenodesis is frequently performed in concert with additional shoulder procedures such as rotator cuff repair (RCR). 19 While isolated long head of the biceps tendonitis and injury can occur, biceps pathology often presents with rotator cuff tears, especially in older patients. 23 Proximal biceps pathology is often treated nonoperatively. However, tenodesis may be performed for a range of indications from tendinopathy and pain to subluxation and mechanical symptoms based on findings from clinical examinations, imaging studies, and/or intraoperative findings. 1,18 Tenotomy is an acceptable alternative to tenodesis when the cosmetic result of a Popeye deformity is not a concern to the patient. 19
Tenodesis techniques vary. With regard to fixation construct, anchor fixation has previously been found to be superior to soft tissue fixation both clinically and biomechanically. 17 Regarding tenodesis location, open subpectoral and arthroscopic suprapectoral tenodesis have both demonstrated positive outcomes, but there is some evidence that subpectoral tenodesis can decrease pain in the bicipital groove. 5,13 Advantages of both suprapectoral and intra-articular top-of-groove fixation include that they do not require an open approach and allow for revision to subpectoral tenodesis, if required. 1 Onlay techniques approximate tendon to bone, whereas inlay techniques “dunk” tendon into a cortical bone socket. 2,6 Some studies have shown a decreased revision rate when an onlay technique is utilized. 6 Although positive clinical outcomes have been reported regardless of tenodesis methods, the optimal biceps tenodesis remains debated. 1
Prior studies, such as the randomized controlled trial by Park et al, 15 have identified a higher anatomic failure rate with interference screw compared with suture anchor biceps tenodesis, in the setting of concomitant RCR, but no difference in functional outcomes. The purpose of the current study was to compare patient pain and functional outcomes when stratified by biceps tenodesis fixation construct, location, and technique in the setting of concomitant RCR using a large cohort of patients. We aimed to capture the optimal number of patients undergoing biceps tenodesis with RCR and hence included medium- and large-sized cuff tears. We hypothesized that patient outcomes would not differ between strata.
Methods
Patients
After receiving approval from our institutional review board, we conducted a retrospective review of the prospectively collected Surgical Outcomes System database (Arthrex) for the years 2015 to 2021. The database was queried independently for patients who underwent biceps tenodesis with concomitant RCR as well as for biceps tenodesis fixation construct (anchor [not including flip anchor or button], screw, or soft tissue suture), tenodesis location (subpectoral, suprapectoral, or top of groove), and technique (inlay or onlay) to obtain the desired data sets. Data sets were independently generated from the database in order to maximize patient inclusion. Patients were included if they had descriptive data (ie, age and sex) available, were ≥18 years of age at time of surgery, had a rotator cuff tear classified as medium (1-3 cm) or large (3-5 cm) per the Cofield 3 classification, and had any outcome scores reported at a minimum 1-year follow-up. Patients were excluded if they were <18 years of age, missing patient data, missing 1-year follow-up, or had a small (<1 cm) or massive (>5 cm) rotator cuff tear.
A total of 1903 shoulder entries were obtained from the database, with distinct groupings based on construct, location, and technique (Figure 1).

Flowchart of patient inclusion. Sub, subpectoral; Supra, Suprapectoral; ToG, top of groove.
Outcome Measures
Pain and functional outcomes assessed included the American Shoulder and Elbow Surgeons (ASES) shoulder score, the Single Assessment Numeric Evaluation (SANE) score, the visual analog scale (VAS) for pain score, and the Veterans RAND 12-Item Health Survey (VR-12) score. Outcome measures were collected preoperatively and postoperatively at 3 months, 6 months, 1 year, and 2 years; the VR-12 score was not assessed at the 3-month follow-up but was available for all other time points. In addition to comparing outcome scores preoperatively and at follow-up visits, we also compared groups based on improvement between the patients’ preoperative visit and 1-year and 2-year follow-ups (1-year and 2-year improvement). Improvement in outcome scores from the preoperative visit to the 1- and 2-year follow-ups was compared with the minimal clinically important difference (MCID) reported for arthroscopic RCR. Reference MCID values used were 11.1 to 27.1 for the ASES score, 13 to 16.9 for the SANE score, and 1.5 to 2.4 for the VAS for pain score; the greatest reported MCID was referenced for each score. 4,10,21
Statistical Analysis
Outcome measures had a nonparametric distribution as assessed by the Shapiro-Wilk test. Thus, age at surgery and outcome measures at each follow-up time point were compared based on fixation construct (anchor, screw, or suture), tenodesis location (subpectoral, suprapectoral, or top of groove), and technique (inlay or onlay) using the Wilcoxon rank-sum test for dichotomous comparisons or the Kruskal-Wallis rank-sum test for trichotomous comparisons. Categorical variables were compared using the chi-square test. Post hoc pairwise comparisons were made with the Dunn test using the Benjamini-Hochberg method for correction of multiple comparisons. The sex distribution and proportion of patients achieving the MCID at the 1- and 2-year follow-up visits were compared between groups using chi-square tests. The Benjamini-Hochberg procedure was used for correction of post hoc pairwise comparisons. All analyses were performed using R software (Version 4.2.0; The R Foundation for Statistical Computing), with P < .05 indicating statistical significance.
Results
The characteristics of the 2146 included shoulders by grouping based on construct, location, and technique are shown in Table 1. Age at surgery varied based on fixation construct and tenodesis location, but not fixation technique. On post hoc analysis, patients receiving a screw were significantly older than those receiving other fixation constructs (P = .028 for pairwise comparison). Additionally, patients receiving tenodesis at the top of the groove were significantly older than patients receiving a subpectoral or suprapectoral tenodesis (P < .001). There were significantly more women who underwent top-of-groove fixation compared with other fixation locations (P = .007). With regard to concomitant rotator cuff tear, more patients with a large tear underwent subpectoral tenodesis, whereas more patients with a medium tear underwent suprapectoral or top-of-groove tenodesis (P < .001).
Characteristics of Included Shoulders a

a Data are presented as mean ± SD or % (n) unless otherwise indicated. Boldface P values indicate a statistically significant difference among groups (P < .05).
Fixation Construct
Improvement in VR-12 Mental score favored anchor and suture over screw fixation at 1 year (3.1 ± 11.1 and 3.8 ± 9.6 vs 1.3 ± 9.6, respectively; P = .042) (Figure 2A), but the other outcome scores demonstrated no significant differences at the 1- and 2-year follow-up visits regarding constructs (Figure 2). The proportion of patients with improvement exceeding the MCID did not differ based on tenodesis construct for any outcome score assessed at the 1- or 2-year follow-up (Table 2). Full comparisons of all outcomes at all available time points are available in Supplemental Table S1, available separately.

Improvement in clinical outcome scores from the preoperative visit to the postoperative (A) 1- and (B) 2-year follow-ups based on fixation construct (anchor vs screw vs suture). ASES, American Shoulder and Elbow Surgeons; SANE, Single Assessment Numeric Evaluation; VAS, visual analog scale; VR-12, Veterans RAND 12-Item Health Survey.
Comparison of Shoulders That Exceeded the MCID for ASES, SANE, and VAS Scores After Arthroscopic Rotator Cuff Repair at 1 and 2 Years of Follow-up a
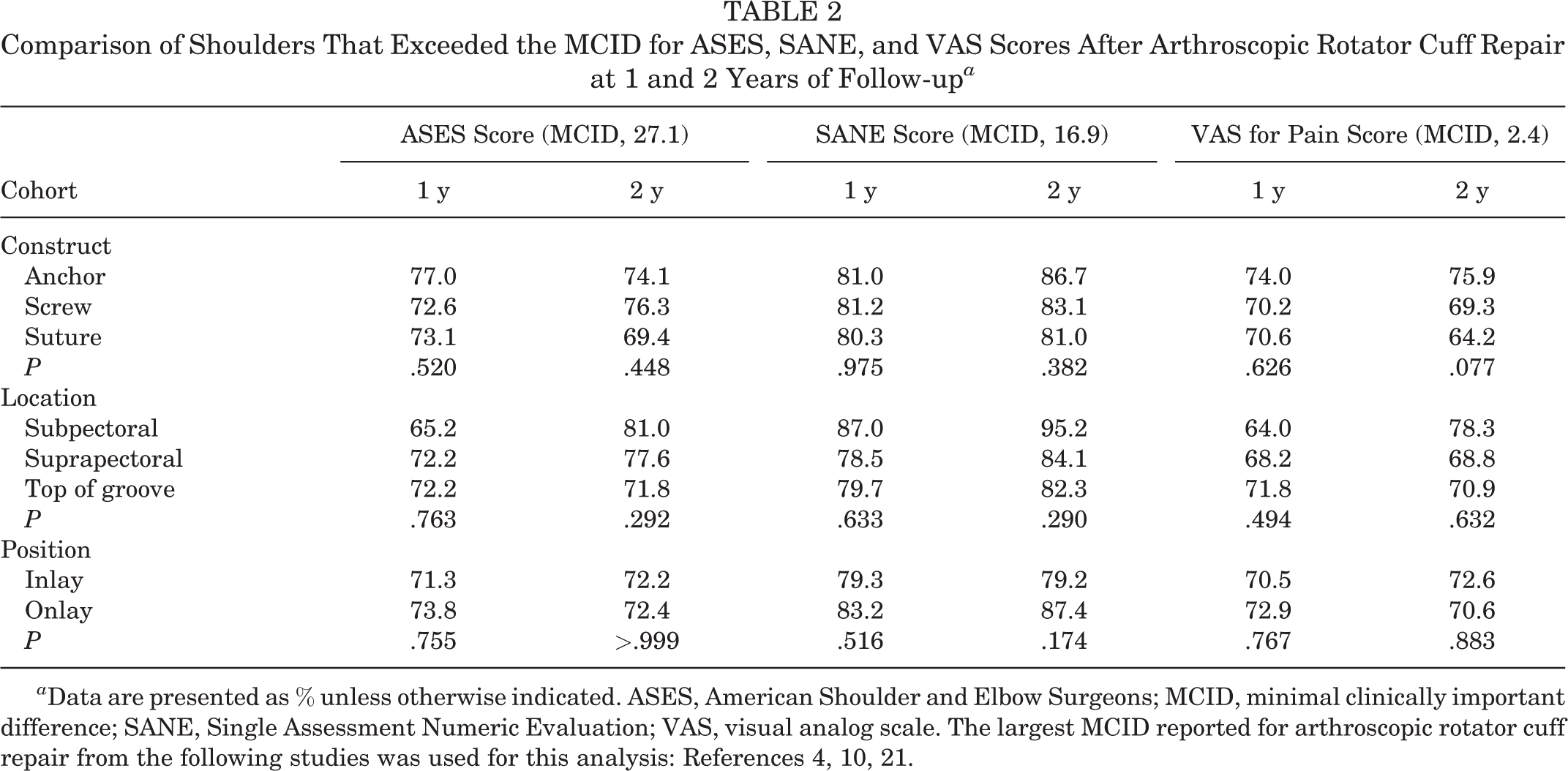
a Data are presented as % unless otherwise indicated. ASES, American Shoulder and Elbow Surgeons; MCID, minimal clinically important difference; SANE, Single Assessment Numeric Evaluation; VAS, visual analog scale. The largest MCID reported for arthroscopic rotator cuff repair from the following studies was used for this analysis: References 4, 10, 21.
Tenodesis Location
No statistically significant differences in outcome scores were found among tenodesis locations (Figure 3). Similarly, the proportion of patients with improvement exceeding the MCID did not differ based on tenodesis location for any outcome score assessed at the 1- or 2-year follow-up (Table 2).

Improvement in clinical outcome scores from the preoperative visit to the postoperative (A) 1- and (B) 2-year follow-ups based on fixation location (subpectoral [Sub] vs suprapectoral [Supra] vs top of groove [ToG]). ASES, American Shoulder and Elbow Surgeons; SANE, Single Assessment Numeric Evaluation; VAS, visual analog scale; VR-12, Veterans RAND 12-Item Health Survey.
Fixation Technique
Improvement in VR-12 Mental score favored the onlay over inlay tenodesis technique at the 2-year follow-up (5.1 ± 10.9 vs 2.1 ± 10.8; P = .029) (Figure 4B), but the remaining outcome scores demonstrated no significant differences (Figure 4). Again, the proportion of patients with improvement exceeding the MCID did not differ based on tenodesis technique for any outcome score assessed at the 1- or 2-year follow-up (Table 2).

Improvement in clinical outcome scores from the preoperative visit to the postoperative (A) 1- and (B) 2-year follow-ups based on fixation technique (inlay vs onlay). ASES, American Shoulder and Elbow Surgeons; SANE, Single Assessment Numeric Evaluation; VAS, visual analog scale; VR-12, Veterans RAND 12-Item Health Survey.
Discussion
There were improved postoperative outcome scores across tenodesis methods in the setting of concomitant arthroscopic RCR for medium and large tears with minimal differences among groups and no clinically significant differences. Improvement in the VR-12 Mental score portended a slight advantage to anchor and soft tissue suture fixation compared with screw at 1 year postoperatively (P = .042). We also demonstrated a slightly more favorable VR-12 Mental score at 2 years postoperatively for the onlay technique (P = .029). We found that patients receiving tenodesis via screw fixation tended to be older than those receiving anchor fixation (P = .028), and top-of-groove location was more frequently used in older patients than subpectoral and suprapectoral tenodesis (P < .001).
Throughout the history of shoulder arthroscopy, the optimal fixation construct, location, and technique for biceps tenodesis have been widely debated. Previous studies have found few or no differences in patient outcomes based on biceps tenodesis surgical characteristics. 1,15 In a study using the Surgical Outcomes System database comparing tenodesis versus tenotomy, tenodesis was shown to provide improved pain and functional scores compared with tenotomy at 2 years; however, the benefit did not exceed the previously reported MCID for the outcome scores. 19 In a 2021 study, Kilic et al 9 evaluated VAS and Constant scores as well as forearm supination and elbow flexion muscle strength pre- and postoperatively in the setting of biceps tenodesis with RCR. The cohort of 19 patients revealed a statistically significant increase in elbow flexion and forearm supination strength at postoperative evaluation. 8 This corroborates the current study’s findings of improved outcomes across tenodesis methods in concomitant RCR. We sought to further delineate any differences between tenodesis methods with concomitant RCR by leveraging a large patient cohort identified via an international, multicenter database. Outcomes such as the ASES score include items addressing pain and functional measures that can act as a proxy for biceps tenodesis integrity. As in prior studies, however, we found minimal statistically significant differences between outcome measures and no clinically significant differences. 13
We found that all fixation constructs led to improved outcomes with concomitant RCR with minimal differences among groups. This is in line with previously reported findings that clinical improvement is possible regardless of fixation construct. 1,15 Improvement in the VR-12 Mental score gave a slight advantage to anchor and soft tissue suture compared with screw at 1 year. Of note, Scheibel et al 17 previously recommended bony over soft tissue fixation given greater improvement in pain/cramps, cosmetic result, and elbow flexion strength. Hwang et al 7 found that bony fixation led to better elbow flexion strength and fewer “empty grooves” on ultrasound. Park et al 15 conducted a prospective randomized study (N = 80) comparing outcome scores (VAS for pain, ASES, and Constant scores) and the anatomic status of the biceps tendon (via magnetic resonance imaging [MRI] or ultrasound) between biceps tenodesis performed using anchor versus interference screw fixation in the setting of concomitant RCR. The authors found no significant differences in the outcome scores assessed at the 2-year follow-up. 11,15 Interestingly, Lacheta et al, 11 via a cadaveric study, concluded that humeral-sided fixation may not be as crucial as biceps tendon–sided suture technique for tenodesis integrity.
In addition to fixation construct, the benefits and drawbacks of various tenodesis locations have been widely explored in the literature; we found no differences in tenodesis outcome scores based on location. Previous literature has reported evidence of greater postoperative pain when the tendon is left in the groove and secured more proximally. 12,13 However, an important consideration is that high-in-groove biceps tenodesis allows for revision to subpectoral tenodesis if failure of proximal tenodesis occurs. 1 Peebles et al 16 effectively documented this concept when evaluating the outcomes of an active military population (N = 12) who underwent conversion of a failed proximal (suprapectoral) to distal (subpectoral) biceps tenodesis and found that all patients had a significant improvement in SANE and ASES scores, with no reported complications, and the ability to return to full active duty. To maximize pain relief and avoid the possibility of bicipital groove pain, subpectoral tenodesis can be performed with RCR; however, as this paper suggests, improvement in pain and functional outcomes can occur with more superior tenodesis locations.
More recently, interest in inlay versus onlay biceps tenodesis technique outcomes has increased given the greater number of available surgical tools. We demonstrated a slightly more favorable VR-12 Mental score at 2 years for onlay, but otherwise there were equivalent outcomes. Tan et al 20 used a rabbit model to compare inlay (bone tunnel) versus onlay (cortical surface) fixation and found that an onlay technique with a cortical surface to the tendon interface led to greater tendon-bone interdigitation and fibrocartilaginous zone formation. Haidamous et al 6 reported that inlay led to increased revision compared with onlay (10.8% vs 0%, respectively; P = .015) in 37 patients. Additionally, the inlay technique is more likely to create a long-term stress riser because of the larger cortical hole needed and increase the risk of iatrogenic proximal humeral fracture. 1 Jackson et al 8 performed a systematic review and meta-analysis comparing onlay versus inlay tenodesis in the setting of biceps tendinopathy. Patients with concomitant RCR were included in the study; VAS for pain, Constant, and ASES scores and rates of Popeye deformity, cramping, and tenodesis failure did not differ between techniques. 8
Proximal biceps pathology can occur at any age, but the origins tend to differ between young and old cohorts. 22 We found that patients receiving tenodesis via screw fixation tended to be older than those receiving anchor fixation. Furthermore, top-of-groove location was more frequently used in older patients than subpectoral and suprapectoral tenodesis. These findings likely relate to the differing pathologies and functional requirements between younger and older patients. The slightly greater proportion of female patients undergoing top-of-groove fixation does not appear to be a consistent finding in the literature or pertinent to the current study.
Limitations
There are several strengths and limitations of this study. The use of large multicenter databases can contribute to the literature by enabling the study of larger patient cohorts, thereby providing greater statistical power, which is often needed to detect subtle differences in patient outcomes. Furthermore, analysis of patients from multiple surgeons spanning large geographic regions improves the generalizability of our results. However, large databases are intrinsically limited by variable surgeon experience and variations of data input into the system as well as loss to follow-up. Certainly, coding bias can occur with any procedural database. 23 More specifically to the current study, because of the limitations in our data source, we were not able to assess rotator cuff fixation methods or rotator cuff fixation failure, and these results are assumed to have been included in the outcome data. We were unable to assess the influence of RCR method on tenodesis method. Additionally, we were unable to assess RCR healing, which is a confounding factor in the assessment of outcome scores. Furthermore, postoperative protocols likely vary by institution and surgeon. Although we demonstrate minimal differences among study groups, it is possible that complications not captured in the database were present, such as downstream loss of tenodesis fixation resulting in Popeye deformity, cramping, or loss of strength. Objective imaging data (MRI or ultrasound) on tenodesis or RCR integrity at follow-up were not available; therefore, we were unable to assess the incidence of failure of either. However, we expect we would have captured clinically relevant changes in patients’ treatment outcome through collected outcome scores if failure of the tenodesis caused pain or dysfunction. Our study provides important contributions to the existing literature by strengthening previously reported minimal differences among tenodesis types in the setting of concomitant RCR, with only slight advantages to anchor fixation and onlay technique. 7,12,13,17
Conclusion
Biceps tenodesis with concomitant RCR leads to improved outcomes regardless of tenodesis fixation construct, location, or technique. A clear optimal tenodesis method with RCR remains to be determined. Surgeon preference and experience with various tenodesis methods as well as patient clinical presentation should continue to guide surgical decision-making.
Supplemental material for this article is available at https://journals.sagepub.com/doi/full/10.1177/23259671231180173#supplementary-materials
Supplemental Material
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671231180173 - Outcomes of Biceps Tenodesis Variations With Concomitant Rotator Cuff Repair: A Multicenter Database Analysis
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671231180173 for Outcomes of Biceps Tenodesis Variations With Concomitant Rotator Cuff Repair: A Multicenter Database Analysis by David P. Hagan, Kevin A. Hao, Joseph J. King, Ramesh C. Srinivasan, Thomas W. Wright, Michael W. Moser, Kevin W. Farmer, Jonathan O. Wright, Marissa Pazik and Ryan P. Roach in Orthopaedic Journal of Sports Medicine
Footnotes
Acknowledgment
The authors thank the OMeGA Medical Grants Association for supporting the University of Florida Shoulder and Elbow surgery fellowship, thus helping make this work possible.
Final revision submitted February 2, 2023; accepted March 9, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.J.K. has received consulting fees from Exactech and LinkBio. R.C.S. has received education payments from Medinc of Texas, consulting fees and nonconsulting fees from Acumed, and hospitality payments from Exactech and Integra LifeSciences. T.W.W. has received consulting fees and royalties from Exactech. M.W.M. has received education payments from Fortis Surgical. K.W.F. has received education payments from Arthrex and CCG Medical; consulting fees from Exactech, Pacira Therapeutics and Arthrex; nonconsulting fees from Arthrex, Baudex, CCG Medical, and Arthrosurface; and honoraria from Baudex. J.O.W. has received education payments from Pinnacle and hospitality payments from Acumed, Stryker, and Zimmer Biomet. R.P.R. has received grant support from Arthrex and education payments from Arthrex and Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Florida (study No. 202100420).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.