
Abstract
Background:
Altered bone morphologies are considered risk factors for noncontact anterior cruciate ligament (ACL) injuries.
Purpose/Hypothesis:
This study aimed to investigate bone morphological characteristics as risk factors for ACL tears in contact injuries and compare these factors with those for noncontact ACL injuries. We hypothesized that altered bone morphologies would also be risk factors for contact ACL injury.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Enrolled were patients who underwent primary ACL reconstructions between January 2000 and December 2021 within 6 weeks after injury. Patients in the ACL group were classified according to injury mechanism (contact vs noncontact). During the same period, a control group of patients matched by age, height, and body mass index to the ACL group was selected. The lateral femoral condylar ratio (LFCR), notch width index (NWI), and lateral posterior tibial slope (PTS) were measured. Measured parameters were compared between the control, contact, and noncontact groups using analysis of variance.
Results:
There were 86 patients in the control group, 102 patients in the contact ACL group, and 105 patients in the noncontact ACL group. The demographic characteristics of the 3 groups did not differ significantly. The contact group had significantly higher LFCRs and lower NWIs compared with the control group (P < .001 and P = .001, respectively). The noncontact group had significantly higher LFCRs and PTSs and lower NWIs compared with the control group (P = .031; P < .001; and P < .001, respectively). The noncontact group had significantly higher PTSs and lower NWIs compared with the contact group (P = .003 and P =.014, respectively). In the contact group, the LFCR, PTS, and NWI were significant risk factors for ACL tears (odds ratio [OR], 1.25 [P < .001]; OR, 1.16 [P = .008]; and OR, 1.27 [P = .001], respectively), and in the noncontact group, the PTS and NWI were significant risk factors for ACL tears (OR, 1.20 [P < .001]; OR, 1.59 [P < .001], respectively).
Conclusion:
Altered bone morphological characteristics of the knee were found to be risk factors for ACL tears in contact injuries as well as noncontact injuries. Altered morphology has a more significant effect in noncontact ACL injuries.
As participation in recreational and competitive sports increases, the incidence of anterior cruciate ligament (ACL) injury increases. ACL injury mechanisms are classified into noncontact and contact injury. 26 Boden et al 2 reported on the mechanisms of 100 ACL injuries from basketball, American football, and soccer. A noncontact mechanism was reported in 72% and a contact injury in 28% of the cases. Most (70%) ACL injuries occur during landing or deceleration maneuvers with minimal to no contact. A systematic video analysis of ACL injuries in professional male soccer players demonstrated that 88% of ACL injuries occurred without direct knee contact. 6 Noncontact ACL injury is associated with a higher posterior tibial slope (PTS), and joint contact occurs on the flat, anterior portion of the lateral femoral condyle versus the round, posterior aspect. Anatomic conditions favor sliding (pivot shift) over rolling in the presence of an axial compressive force. 3
Larger quadriceps angle, greater knee valgus, and greater navicular drop are considered risk factors for noncontact ACL injuries. 11 In addition, nonmodifiable bone morphological characteristics such as narrower intercondylar notch width, 18,21,24 increased PTS, 8,17,22 higher trochlear sulcus angle, 18 and increased posterior condylar depth 15,20 have been reported as risk factors for noncontact ACL tears. However, there is a paucity of literature reporting bone morphology–related risk factors for contact ACL injury. This retrospective study aimed to investigate bone morphological characteristics as risk factors for ACL tears in contact injuries and compare these factors with those for noncontact ACL injuries. We hypothesized that altered bone morphologies would also be risk factors for contact ACL injury.
Methods
Study Population
The protocol for this study was reviewed and approved by an institutional review board. We enrolled consecutive patients who underwent primary ACL reconstruction (ACLR) within 6 weeks after injury. All surgeries occurred at a single institution between January 2000 and December 2021. The patients were classified according to injury mechanism as belonging to either the contact ACL or noncontact ACL group. 26 Patients with ACL injuries who underwent reconstruction within 6 weeks of the injury were eligible for inclusion. Patients with chronic ACL tears or concomitant ligamentous injuries were excluded from this study. Patients were also excluded if the lateral radiographs of their affected knee showed an overlap of >6 mm between the posterior halves of the medial and lateral femoral condyles, and if their magnetic resonance imaging (MRI) scans were not of acceptable quality.
A control group with knee pain but no ligamentous or meniscal injuries and no trochlear dysplasia as determined by MRI was also included. The contact and control groups were matched to the noncontact group based on age, height, and body mass index (BMI).
A total of 1198 patients underwent ACLR at our institution. Of these, 496 patients with chronic ACL injury, 136 patients with combined ligamentous injury, 258 patients with inadequate radiographs or MRIs, and 101 patients with incomplete medical records were excluded, leaving 207 patients eligible for study inclusion. There were 102 patients in the contact ACL group and 105 patients in the noncontact ACL group. The matched control group consisted of 86 patients (Figure 1).
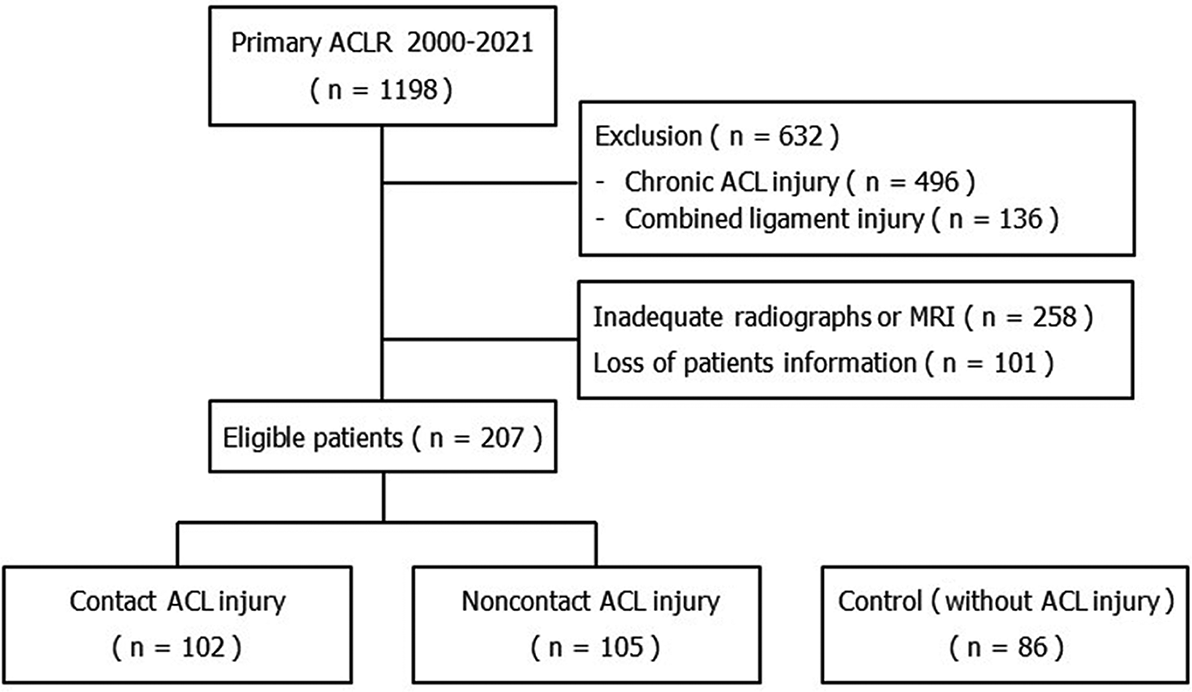
Flowchart of the study groups. ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction; MRI, magnetic resonance imaging.
Plain Radiographs and MRI Measurements
Lateral radiographs and preoperative MRIs were available for the included control, contact, and noncontact groups. All MRI examinations were performed on either a 1.5-T (Siemens Avanto) or a 3-T (Siemens Skyra) system. True or nearly true lateral radiographs of the knee were confirmed in all patients. The true lateral view showed superimposition of the medial and lateral condyles of the distal femur. The nearly true lateral view showed <6 mm of the overlap between the posterior halves of the medial and lateral condyles. 20
To evaluate the posterior femoral condylar depth, the lateral femoral condylar ratio (LFCR), reported as a percentage, was measured on true lateral radiographs as described in the literature 20 (Figure 2). The lateral PTS was measured on the central sagittal MRI as described previously 13 (Figure 3, A and B). An axial view MRI showing the intercondylar notch was used to measure the notch width index (NWI), reported as a percentage and calculated as the width of the central notch divided by the transcondylar width, as described in the literature 4 (Figure 3C).

Measurement of the lateral femoral condylar ratio. On a true lateral radiograph, 2 circles were drawn along the distal femoral shaft, 5 cm apart, and the long axis of the distal femur was considered the line connecting the centers of the circles. Another line perpendicular to the long axis of the distal femur was drawn from between the most anterior point and the most posterior point of the lateral condyle (lateral condylar length; A + B). The distance from the intersection of the 2 lines to the most posterior point of the condyle, B, was divided by distance A + B. The lateral femoral condylar ratio was calculated as (B/ [A + B]) × 100%.

(A) The long axis of the proximal tibia (white line), created on the sagittal-view MRI, showing the tibial attachment of the posterior cruciate ligament, the intercondylar eminence, and the anterior and posterior tibial cortices. The axis is created by connecting the centers of a proximal circle bound by the anterior, posterior, and proximal tibial cortex bone and a distal circle bound by the anterior and posterior cortex border. (B) Measurement of the lateral posterior tibial slope (asterisk), created on the sagittal-view MRI at the mediolateral center of the lateral tibial plateau. The slope represents the angle between a line perpendicular to the longitudinal axis of the proximal tibia (thick white line) and another line tangential to the lateral tibial plateau (dashed line). (C) Measurement of the notch width index, calculated by dividing the central notch width, B, by the transcondylar width, A. MRI, magnetic resonance imaging.
All measurements were performed by an orthopaedic resident who was blind to the patient group. All measurements were repeated 4 weeks later to calculate the intraobserver correlation coefficient (ICC).
Statistical Analysis
The LFCR, PTS, and NWI were reported as mean and standard deviation. The LFCR, PTS, and NWI were compared between the control, contact, and noncontact groups using the analysis of variance test. The sample size was calculated using previously published literature. 13,15,16 The calculated sample sizes for the LFCR, PTS, and NWI were 25, 24, and 11 in each group, respectively. The primary outcome was the LFCR. Multiple regression analysis was performed to investigate whether the LFCR, PTS, and NWI were risk factors for the ACL tear. Data were analyzed using the SPSS statistical package Version 25.0 (SPSS Inc) and G*power program Version 3.1.5 (http://www.gpower.hhu.de/). The significance level was set at .05.
Results
The demographic characteristics of the control, contact ACL, and noncontact ACL groups are described in Table 1. Age, height, BMI, and sex did not differ significantly among the 3 groups. The ICCs for the intraobserver reliability for the LFCR, PTS, and NWI were 0.82 (95% CI, 0.63-0.90), 0.85 (95% CI, 0.78-0.90), and 0.90 (95% CI, 0.85-0.94), respectively, indicating good to excellent reliability.
Comparison of Preoperative Demographic Characteristics Among the Study Groups a

a Data are reported as mean ± SD or No. of patients. ACL, anterior cruciate ligament; BMI, body mass index.
Contact and noncontact groups had significantly higher LFCRs and PTSs and smaller NWIs than those of the control group (P < .001, P < .001, and P < .001, respectively) (Table 2). In subgroup analysis, the contact group had significantly higher LFCRs and lower NWIs than those of the control group (P < .001 and P = .001, respectively). The PTS did not differ between the control and contact groups. The noncontact group had significantly higher LFCRs and PTSs and lower NWIs than those of the control group (P = .031, P < .001, and P < .001, respectively). The noncontact group had significantly higher PTSs and lower NWIs than those of the contact group (P = .003 and P = .014, respectively). The LFCR did not differ between the contact and noncontact groups (Table 3).
Comparison of Bone Morphological Characteristics Among the Study Groups a
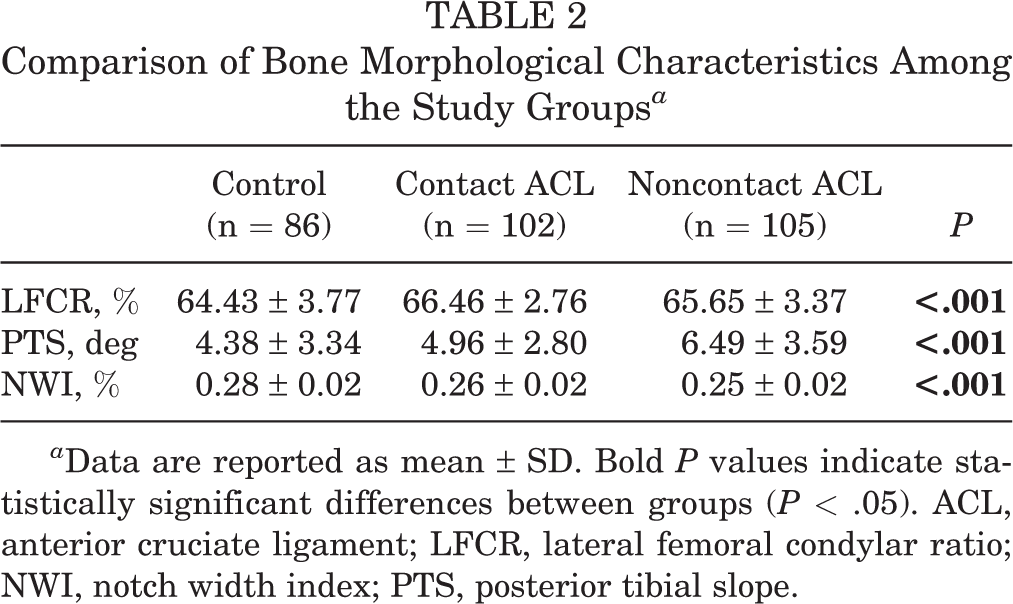
a Data are reported as mean ± SD. Bold P values indicate statistically significant differences between groups (P < .05). ACL, anterior cruciate ligament; LFCR, lateral femoral condylar ratio; NWI, notch width index; PTS, posterior tibial slope.
P Values for Comparisons of Bone Morphological Characteristics Among the Study Groups a

a Bold P values indicate statistical significance (P < .05). LFCR, lateral femoral condylar ratio; NWI, notch width index; PTS, posterior tibial slope.
In the contact group, logistic regression analysis demonstrated that the LFCR, PTS, and NWI were significantly associated factors for ACL tears (odds ratio [OR], 1.25 [P < .001]; OR, 1.16 [P = .008]; and OR, 1.27 [P = .001], respectively). When the LFCR and the NWI were present simultaneously, an ACL tear was more likely to occur (OR, 3.89 [95% CI, 1.99-7.58]). In the noncontact group, logistic regression analysis demonstrated that the PTS and the NWI were significant factors associated with ACL tears (OR, 1.20 [P < .001]; OR, 1.59 [P < .001], respectively). The risk of noncontact ACL tear was increased in patients with LFCRs and NWIs (OR, 8.82 [95% CI, 3.28-23.67]), LFCRs and PTSs (OR, 13.67 [95% CI, 4.66-40.12]), or with PTSs and NWIs (OR, 13.59 [95% CI, 5.45-33.88]).
Discussion
The most important finding of this study was that the bone morphological characteristics of the knee are risk factors for ACL tears in contact injuries as well as noncontact injuries. They were not as significant a risk factor in the contact group compared with the noncontact group. In the contact group, the LFCR, PTS, and NWI were significantly associated risk factors for ACL tears. ACL tears were associated with an increased risk when the LFCR and NWI were combined (OR, 3.89). The noncontact group had significantly higher PTSs and lower NWIs than those of the contact group. The LFCR did not differ between the contact and noncontact groups.
Risk factors for noncontact ACL injuries are divided into extrinsic and intrinsic (environmental, hormonal, anatomical, and neuromuscular) factors. 11 As anatomical factors, the intercondylar notch width and PTS have been extensively investigated as risk factors for noncontact ACL injuries. 5,9,19,21,25,27 Type A intercondylar notch, which is narrow from the base to the midsection as well as at the apex, was associated with a significantly increased probability of suffering a noncontact ACL injury in female (OR, 4.99) and male (OR, 5.50) patients. 1 An increased alpha angle between the long axis of the distal femur and the Blumensaat line was the most significant factor associated with an ACL injury. 1 A meta-analysis reported that the notch width was significantly narrower in patients with an ACL injury than in the control cases, and this finding persisted even when stratified by ethnicity and sex. 18 A steeper PTS may increase the axial compression load, which could lead to the lateral femoral condyle’s sliding posteriorly off from the lateral tibial plateau, increasing the strain on the ACL and the inherent risk of rupture. 10
Although studies reporting increased PTS as a risk factor for an ACL injury have been published with increasing frequency, the reported tibial slope values for control groups vary between studies. This may be because there are many methods to measure the PTS. A systematic review 27 reported that in controls, the mean value ranged from 0.3° ± 3.6° anterior slope to 9° ± 4° posterior slope. In ACL-injured groups, mean lateral PTS values ranged from 1.8° ± 3.2° to 11.5° ± 3.5° posterior slope.. There has also been disagreement regarding the actual values of the slope that would be considered “at risk.” 27
Previous studies have reported bone morphology–related risk factors associated with noncontact ACL injuries. 8,14,17,21,24 Regarding studies that reported these risk factors for contact ACL injuries, DePhillipo et al 7 found that the PTS increased significantly among patients with contact ACL tears as compared with controls. In the present study, the PTS did not differ between the control and contact groups. However, the contact group had significantly higher LFCRs and lower NWIs than those of the control group (P < .001 and P = .001, respectively). DePhillipo et al also reported that the PTS did not differ between patients who sustained contact versus noncontact ACL tears. In this study, the noncontact group had significantly higher PTS than that of the contact group (P = .003). Additionally, the noncontact group had a significantly narrower notch than that of the contact group (P = .014). However, the LFCR did not differ between the contact and noncontact groups.
In the present study, both the contact and noncontact groups had significantly higher LFCRs and lower NWIs compared with the control group. In addition, both LFCRs and NWIs were associated with an increased risk for ACL tears in the contact group (OR, 1.25 and 1.27, respectively). Increased lateral condylar depth has been investigated recently as a risk factor for noncontact ACL injuries. 15,20 Increased lateral condylar depth can exaggerate the pivoting mechanism that is the rolling of the lateral femur from its round flexion radius to its more flattened part near extension on the convex lateral tibial plateau. 12 An LFCR >63% has been significantly associated with a higher risk of ACL injury when compared with the control group. 20 Exaggerated pivoting by increased lateral condylar depth during a contact injury may push the ACL within a narrow intercondylar notch. Additionally, an altered relationship between the shape of the lateral posterior condyle and the lateral tibial plateau can exaggerate the pivoting mechanism. A decreased anteroposterior distance of the tibial plateau in relation to an increased distal flattened femoral surface may predispose to a higher risk of ACL injuries. 10 However, the ratio between the distance of the distal flattened femoral surface and the anteroposterior distance of the lateral tibial plateau was not measured in this study.
The present study demonstrated that the combination of the LFCR and NWI increased the risk of an ACL tear (OR, 3.89) in the contact group and that the combination of the LFCR and NWI (OR, 8.82), the LFCR and PTS (OR, 13.67), and the PTS and NWI (OR, 13.59) increased the risk of ACL tears in the noncontact group. Therefore, altered morphologies of the knee may have a greater effect on the increased risk for ACL injury in noncontact injuries. 23
Some contact ACL injuries may be preventable. Contact ACL injuries may be potentially mitigated or decreased with bracing and injury prevention programs. Some of the contact injuries are attributed to the contact only; however, there may be noncontact mechanisms, which may contribute significantly to an injury in the contact setting as well. The combination of the force of contact and the shift in knee kinematics caused by altered knee morphology may cause contact ACL injuries. It is helpful to elaborate on the knowledge of contact and noncontact types of injuries for sports medicine clinicians. The association between 3 bone morphology–related risk factors (large LFCR, high PTS, and narrow intercondylar notch) and the type of contact injury (hyperextension, twisting, and valgus or varus) should be investigated in the future.
Limitations
There were limitations in this study. First, many patients with ACL injuries who had chronic injuries or unacceptable radiographs or MRIs were excluded from this study, and the excluded patients could affect the results of this study. Second, the injury mechanism was dependent on the recall memory of the patients. Incorrect memory of the patients could affect the number of patients in the contact or noncontact injury groups. Third, the risk for an ACL tear in women may increase because of other intrinsic factors, such as larger pelvic widths, increased quadriceps angles, lower hamstring-to-quadriceps ratios, and differences in knee and hip range of motion. However, sex differences and other intrinsic factors were not investigated in this study. Fourth, interobserver reliability was not evaluated because only a single observer measured all parameters. Fifth, all patients and controls were Asian. Thus, ethnic differences in the morphology and dimensions of the distal femur may exist.
Conclusion
Altered bone morphological characteristics of the knee were found to be risk factors for ACL tears in contact injuries as well as noncontact injuries. Altered morphology has a more significant effect in noncontact ACL injuries.
Footnotes
Final revision submitted February 25, 2023; accepted March 9, 2023.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Nowon Eulji Medical Center, Eulji University (No. EMCS 2022-01-021).