
Abstract
Background:
Existing systematic reviews have sought to characterize the relative donor-site morbidity of bone–patellar tendon–bone (BTB) and quadriceps tendon (QT) grafts after anterior cruciate ligament reconstruction (ACLR). However, no studies have reported the pooled proportions of patellar fractures and donor tendon ruptures across the body of literature.
Purpose:
To estimate the proportion of patellar fractures, patellar tendon ruptures, and QT ruptures associated with BTB or QT autograft harvest during ACLR using published data.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A meta-analysis was conducted according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines using 3 online databases (PubMed, Scopus, and Web of Science). A total of 800 manuscripts were included in the initial research of peer-reviewed articles in English that reported extensor mechanism complications associated with graft harvest in patients after ACLR. Pooled proportions of patellar fractures, patellar tendon ruptures, and QT ruptures were calculated for each graft type (BTB, QT) using a random-effects model for meta-analysis.
Results:
A total of 28 studies were analyzed. The pooled proportion of patellar fractures was 0.57% (95% CI, 0.34%-0.91%) for the BTB harvest and 2.03% (95% CI, 0.78%-3.89%) for the QT harvest. The proportion of patellar tendon ruptures was 0.22% (95% CI, 0.14%-0.33%) after the BTB harvest, and the proportion of QT ruptures was 0.52% (95% CI, 0.06%-1.91%) after the QT harvest. The majority of included studies (16/28 [57.1%]) had an evidence level of 4.
Conclusion:
Based on the current literature, the proportion of extensor mechanism complications after ACLR using either a BTB or a QT autograft is low, indicating that the extensor mechanism harvest remains a safe option. A higher proportion of patellar fractures was noted for QT grafts and a higher proportion of donor tendon ruptures was noted for QT grafts compared with BTB grafts.
Anterior cruciate ligament (ACL) reconstruction (ACLR) has been extensively studied over the past 3 decades to optimize techniques and improve patient outcomes. 51 Techniques for arthroscopic ACLR have evolved with progressively lower surgical revision rates. 41 Areas of research interest have included transtibial versus tibial-independent femoral tunnel drilling, 40 single- versus double-bundle reconstructions, 22 graft choice, 35 and graft fixation technique. 47
Graft choice during ACLR has been a particularly important area of research. 3,12,51 Graft options for ACLR include bone–patellar tendon–bone (BTB) autografts, quadriceps tendon (QT) autografts, hamstring tendon (HT) autografts, and a variety of allografts. 29 A recent survey analysis from the ACL Study Group found that BTB graphs were the most commonly used graft in the early 1990s, but over time, HT grafts have become more frequently used. 2 Since 2014, there has also been an increase in the utilization of QT grafts. 51 Each of these options has the potential to restore translational and rotational knee stability when performed using a proper technique. 12,15,36
The decision of which graft to utilize during ACLR involves shared decision-making between the surgeon and the patient. Important factors to discuss include the relative revision rates of graft options, 28 as well as the donor-site morbidity of autografts. For extensor mechanism autografts (eg, BTB and QT), reports of donor-site morbidity in the form of kneeling pain and anterior knee pain have found less morbidity with QT grafts when compared with BTB grafts. 27 A less frequent yet substantial source of morbidity using extensor mechanism grafts is the potential for extensor mechanism disruption in the form of postoperative patellar fracture or donor-site tendon rupture. While careful techniques can minimize these risks, their incidence cannot be ignored in clinical studies. 6
Existing systematic reviews have sought to characterize the relative donor-site morbidity of BTB and QT grafts. 9,12,23 However, those studies have focused on donor-site symptoms without reporting pooled proportions of patellar fractures and donor tendon ruptures across the body of literature. 9,12,23 The purpose of this study was to estimate the proportion of patellar fractures, patellar tendon ruptures, and QT ruptures after a BTB or QT autograft harvest in ACLR using pooled proportions of published data. We hypothesized that BTB and QT autografts would result in a similar proportion of extensor mechanism complications.
Methods
Using the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, 33 studies investigating the extensor mechanism morbidity of various BTB and QT autografts for ACLR were identified. Extensor mechanism morbidity was defined as intra- and postoperative patellar fractures, patellar tendon ruptures, and QT ruptures.
Search Strategy
A systematic search of extensor mechanism morbidity after ACLR with BTB and QT autografts was conducted using 3 online databases (PubMed, Scopus, and Web of Science) from database inception to September 30, 2020. The search was conducted using multiple combinations of the following terms to retrieve potentially relevant articles: “ACL,” “ACLR,” “ACL reconstruction,” “anterior cruciate ligament reconstruction,” “bone-patellar-bone,” “quadriceps tendon,” “autograft,” “donor site morbidity,” “extensor mechanism,” “patellar fracture,” “patellar tendon tear,” “patellar tendon rupture,” “quadriceps tendon tear,” “quadriceps tendon rupture,” “complication,” and “complications.” Conditions were applied to each database search, as follows: “English articles,” “clinical studies,” “any publication date,” “peer-reviewed,” and “published in the journal.”
Study Criteria and Screening Process
Clinical studies reporting the extensor mechanism morbidity of patients receiving BTB or QT autografts for ACLR were included in this meta-analysis. Studies including the addition of nonstandard drugs or biologics, concurrent ligament procedures other than ACLR, only allografts, or non-BTB or non-QT autografts were excluded. The inclusion and exclusion criteria for the study are presented in Table 1.
Study Inclusion and Exclusion Criteria a

a ACLR, anterior cruciate ligament reconstruction; BTB, bone–patellar tendon–bone; intra, intraoperative; QT, quadriceps tendon.
After the removal of duplicate articles, potentially relevant articles retrieved from the 3 databases were screened for eligibility based on pre-established study criteria (Table 1). The title, abstract, and full-text screening was performed by 2 reviewers (R.L. and W.H.) independently. A third reviewer (N.A.T.) was consulted to resolve potential areas of disagreement. To ensure that all available studies were identified, all references from the included studies were reviewed and reconciled to verify that no relevant articles were missing from the systematic review. No further studies were identified during this step.
Data Collection and Data Items
A predesigned spreadsheet was created using Microsoft Excel (Version 2016; Microsoft) and used to extract data from the included articles. Two reviewers (R.L. and W.H.) independently extracted data from each of the included studies, and any discrepancies were resolved by consensus with a third independent reviewer (I.B.K.), of which there were none. The collected data included study design, level of evidence, number of patients analyzed, patient characteristics (age, sex), type of autograft used (BTB or QT), follow-up time, incidence of intraoperative patellar fractures, number of postoperative patellar fractures, number of patellar tendon ruptures, and number of QT ruptures. Studies containing data on multiple groups—for example, reporting patellar fractures after both BTB and QT autografts—were split into separate data sheets for analysis of each group. To determine the pooled proportions of fractures associated with QT and BTB ACLRs, intra- and postoperative fractures were combined. Additional qualitative data were collected on the graft harvest method, patellar fracture rehabilitation protocol, and tendon rupture rehabilitation protocol.
Quality Control
The level of evidence of the included articles was assigned based on the accepted classification by the American Academy of Orthopaedic Surgeons. 49 The methodological quality of studies was evaluated using the Mixed Methods Appraisal Tool (MMAT) Version 2018 (http://mixedmethodsappraisaltoolpublic.pbworks.com). The MMAT tool was originally developed in 2006 to evaluate the quality of 5 study categories, including qualitative research, randomized controlled trials, nonrandomized studies, quantitative descriptive studies, and mixed methods studies. The MMAT Version 2018 has been used in previously published reviews. 21
Statistical Analysis
Descriptive statistics, including the mean and standard deviation, for any numerical variable were recorded. Any missing standard deviation was estimated using pre-established methodologies. 50 Pooled rates of patellar fracture, patellar tendon rupture, and QT rupture were calculated using random-effects proportion meta-analysis (MedCalc Statistical Software Version 19.2.6; MedCalc Software). In the random-effects model, both the random variation within the studies and the variation between the different studies were incorporated to estimate an overall proportion for a specific complication. Heterogeneity was assessed using the I 2 statistic, 20 and the risk of bias was detected using a funnel plot. Because of the small sample size and lack of high-quality comparison studies reporting extensor mechanism morbidity after BTB and QT autografts, no statistical comparison between autograft types could be performed.
Results
Search Results and Study Selection
After the removal of duplicates, a total of 550 potentially eligible studies were retrieved from the 3 databases. The title, abstract, and full-text screening resulted in 28 studies, § consisting of 14,709 patients who were eligible for the final inclusion in the meta-analysis. Figure 1 depicts the study selection process and reasons for exclusion at the full-text stage. Of the 28 studies, 19 studies (19/28 [67.9%]) reported patellar fracture data after BTB autografts, ∥ and 8 studies (8/28 [28.6%]) reported patellar fracture data after QT autografts. 3,7,14,15,17,18,26,43 Ten studies (10/28 [35.7%]) reported patellar tendon rupture data after BTB autografts, 3 –5,11,13,25,30 –32,45 and 3 studies (3/28 [10.7%]) reported QT rupture data after QT autografts. 3,15,44 The characteristics of the studies that investigated patellar fracture and patellar tendon rupture are shown in Tables 2 and 3, respectively.
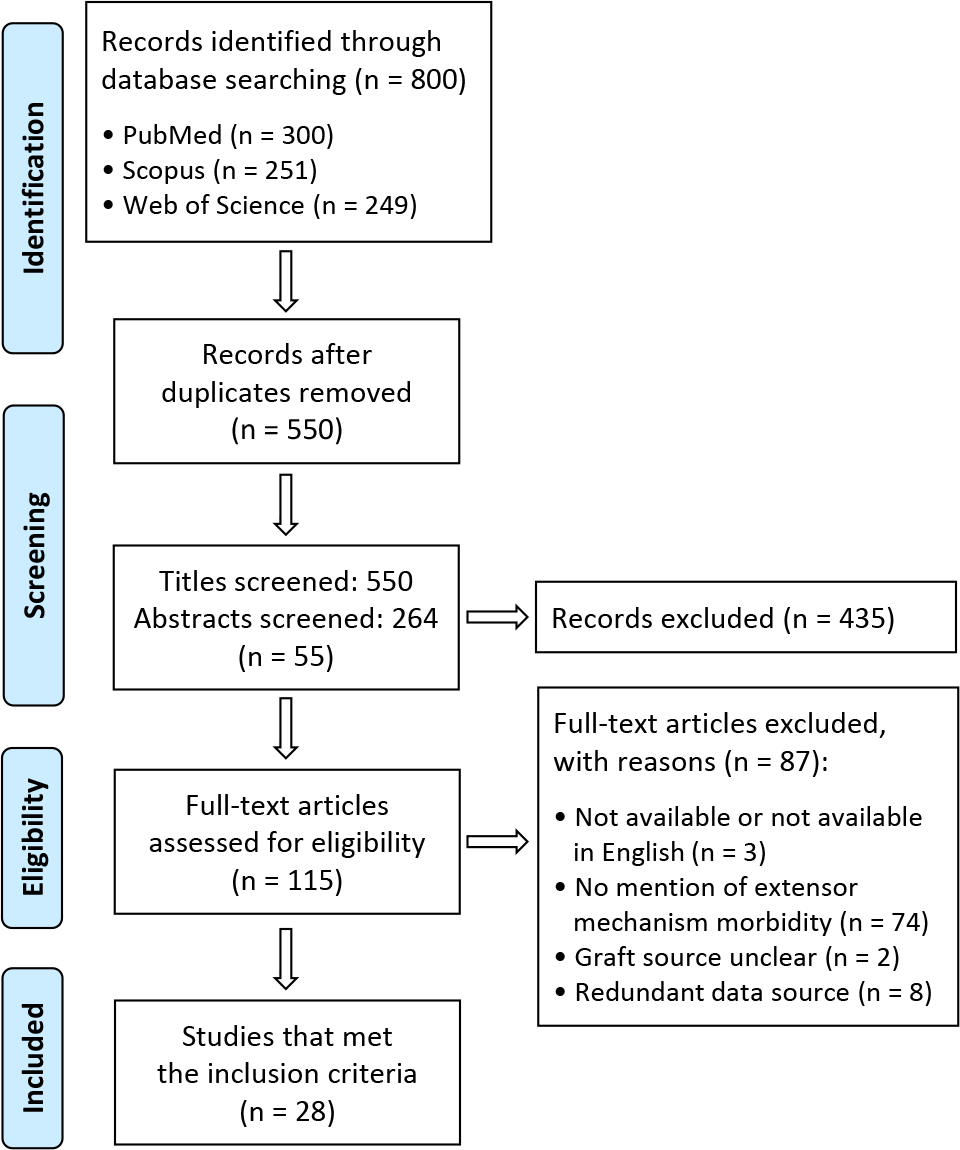
Study flowchart with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines.
Studies Investigating Patellar Fracture After BTB or QT for ACLR a

a ACLR, anterior cruciate ligament reconstruction; BTB, bone–patellar tendon–bone; F, female; LOE, level of evidence; M, male; NR, not reported; QT, quadriceps tendon.
b Data are reported as mean ± SD.
Studies Investigating Patellar Tendon Rupture After BTB for ACLR a

a ACLR, anterior cruciate ligament reconstruction; BTB, bone–patellar tendon–bone; F, female; LOE, level of evidence; M, male; NR, not reported.
b Data are reported as mean ± SD.
Quality of the Included Studies
The majority of the included studies (16/28 [57.1%]) had an evidence level of 4; 1 study (3.6%) had an evidence level of 1; 3 studies (10.7%) had an evidence level of 2; and 8 studies (28.6%) had an evidence level of 3 (Tables 2 and 3). The majority of studies (25/28 [89.2%]) met ≥4 of the 5 MMAT criteria and received an MMAT rating of ≥80%; only 3 studies 15,17,32 did not meet these criteria.
Patellar Fractures After BTB Autograft
A total of 8424 patients were analyzed across 19 studies reporting patellar fracture data after BTB ACLR (Table 2). Out of these 19 studies, 13 (13/19 [68.4%]) studies reported patient sex; of the 4717 patients included in these 13 studies, the majority were men (74.3%). Fourteen studies (14/19 [73.7%]) reported patient age and 8 studies (8/19 [42.1%]) detailed follow-up time. The mean patient age was 28.9 ± 4.8 years, and the mean follow-up time was 5.5 ± 3.1 years (range, 1.8-13.1 years).
A total of 42 patellar fractures associated with BTB ACLR were identified. The pooled proportion of patellar fracture after BTB autografts was 0.57% (95% CI, 0.34%-0.91%) (Figure 2). Moderate heterogeneity was detected in this study group (I 2 = 58.2% [95% CI, 30.5%- 74.8%), although the funnel plot revealed no distinct asymmetry (Figure 3), indicating a low risk of publication bias. Zero patellar fractures were reported in 10 studies (10/19 [52.6%]), and 7 studies contained ≥1 patellar fracture specified the management of the fracture (7/9 [77.8%]) (Table 1). Additionally, 4 studies (4/9 [44.4%]) with patellar fractures detailed the mechanism of injury. Seven (7/20 [35%]) fractures occurred intraoperatively while removing the bone block, 8 (8/20 [40%]) were the result of trauma postoperatively, and the remaining 5 (5/20 [25%]) were postoperative nontraumatic fractures.

Forest plot of the estimated proportion of patellar fractures for bone–patellar tendon–bone autografts for anterior cruciate ligament reconstruction.
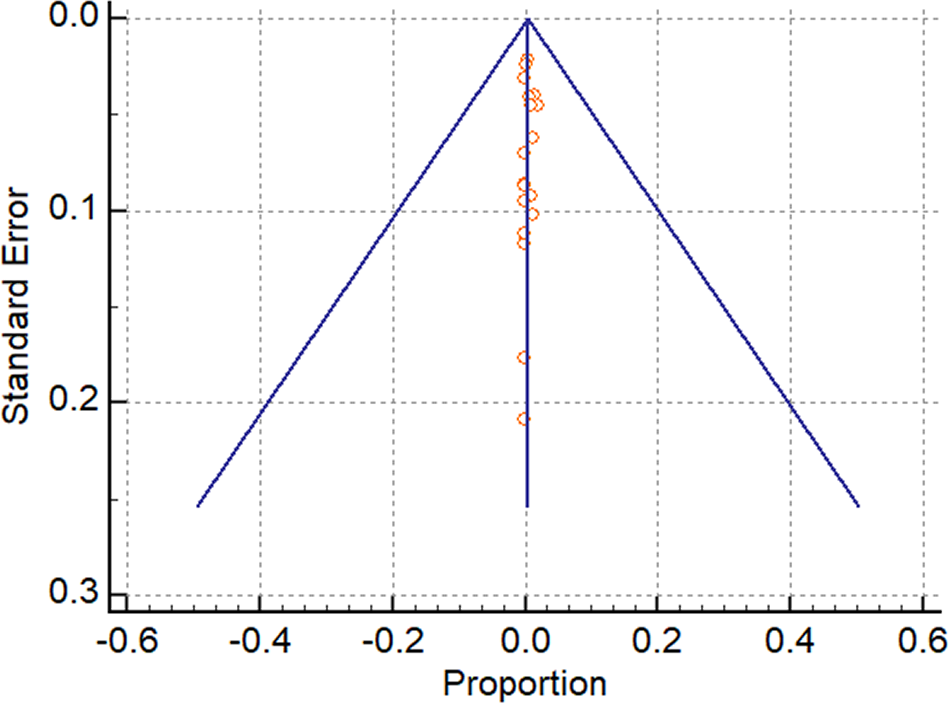
Funnel plot of the study proportion of patellar fractures after bone–patellar tendon–bone autografts against the SE.
Patellar Fractures After QT Autograft
Eight studies containing 766 patients reported patellar fracture data after QT ACLR (see Table 2). The majority of the 462 patients in the 6 studies that detailed patient sex were men (86.3%). The mean age was 28.5 ± 3.6 years (7/8 [87.5%]) in the studies that recorded patient age. The mean follow-up time was 2.8 ± 1.2 years (range, 2-3.8 years).
Twelve fractures associated with QT ACLR were identified. The pooled proportion of patellar fracture after a QT autograft was 2.03% (95% CI, 0.78%-3.89%). Moderate heterogeneity was detected in this study group (I 2 = 41% [95% CI, 0%-73.94%]), and 3 studies (3/8 [37.5%]) had zero patellar fractures. The majority (4/5 [80%]) of the studies with ≥1 patellar fracture reported fracture management (see Table 2). All 5 studies with patellar fractures detailed the mechanism of injury. Six fractures (6/12 [50%]) occurred during intraoperative graft harvesting, 2 (2/12 [16.7%]) resulted from postoperative trauma, and the remaining 4 (4/12 [33.3%]) were due to nontraumatic mechanisms postoperatively.
Patellar Tendon Tears After Patellar Tendon Autograft
Ten studies reported patellar tendon tear data after BTB ACLR, with a total sample size of 10,890 patients (see Table 3). Six studies (6/10 [60%]) containing 2122 patients detailed patient sex and age. The majority (70.7%) of these patients were men, with a mean age of 30 ± 3.1 years. Four (4/10 [40%]) studies recorded a mean follow-up time of 4.2 ± 0.8 years (range, 2-9.4 years).
A total of 22 patellar tendon ruptures associated with BTB ACLR were identified. The pooled proportion of patellar tendon ruptures was 0.22% (95% CI, 0.14%-0.33%). Four studies did not report any patellar tendon tears, and the I 2 was 0% (95% CI, 0%-50.13%). Most (5/6 [83.3%]) of the studies with ≥1 patellar tendon rupture detailed tendon rupture treatment (see Table 3). Of those studies, 4 (4/5 [80%]) reported the use of allograft tissue to augment the patellar tendon repair.
QT Tears After QT ACLR
Three studies (3/28 [10.7%]), with a total of 376 patients, reported QT tears after QT ACLR. All 3 studies detailed patient sex and age. Also, 84% of patients were men and 16% were women, with a mean age of 28.5 ± 4.6 years. Only 1 study 44 (1/3 [33.3%]) specified a mean follow-up time of 2.5 ± 2.4 years (range, 2-3.2 years).
Only 1 QT rupture associated with QT ACLR was identified. The pooled proportion of QT ruptures after QT autografts was 0.52% (95% CI, 0.06%-1.91%). However, 2 studies 3,44 out of the 3 included studies (2/3 [66.7%]) did not have any QT tears, and the 1 study 15 (1/3 [33.3%]) that contained a QT rupture did not specify how the rupture was managed. The estimated I2 was 0% (95% CI, 0%-43.04%).
Comparisons Between QT and BTB Complications
Definitive statistical comparisons could not be made between QT and BTB ACLR because of the data heterogeneity. Qualitative differences were noted in the complication rates. Based on mixed effect proportions meta-analysis of the included studies in 1000 BTB ACLRs, one could expect 5.7 patellar fractures and 2.2 patellar tendon ruptures; in 1000 QT ACLRs, one could expect 20.3 patellar fractures and 5.2 QT ruptures. Four (4/10 [40%]) studies recorded a mean follow-up time of 4.2 ± 0.8 years.
Discussion
This meta-analysis of 28 studies examined the proportion of 3 specific knee extensor mechanism complications in 14,709 patients who underwent ACLR with BTB or QT autografts. The pooled proportion of patellar fracture associated with ACLR was 0.57% for BTB autografts and 2.03% for QT autografts. There was moderate heterogeneity in the reported results for fractures after BTB and QT ACLR, but overall, there was low risk of publication bias as evidenced by symmetric funnel plots for each complication. The pooled proportion of patellar tendon ruptures associated with BTB ACLR was 0.22% and the pooled proportion of QT ruptures associated with QT autografts was 0.52%. For these complications, there was low heterogeneity across studies.
Direct clinical comparisons of BTB ACLRs with QT ACLRs in the literature have reported that QT autografts result in similar clinical functional outcomes with lower rates of kneeling pain and anterior knee discomfort when compared with BTB autografts. 18,27,39 However, clinical studies have been unable to quantitatively compare the rate of patellar fracture or donor tendon rupture because of the limited sample size. In the present study, strict criteria were used to identify studies that explicitly reported the presence or absence of patellar fractures or donor tendon ruptures associated with ACLR using extensor mechanism autografts. While sample sizes remain modest for these rare complications and direct statistical comparisons could not be made, this meta-analysis found that in the current literature, both patellar fractures and donor tendon ruptures are more commonly reported after QT grafts when compared with BTB grafts.
The present study is not the first to report on the risk of patellar fractures after QT ACLR. In a systematic review of 24 studies comparing bone and soft tissue quadriceps grafts for ACLR, Crum et al 9 identified 8 patellar fractures in the bone-QT group versus none in the soft tissue QT group; however, the authors did not report a pooled proportion or discuss donor tendon ruptures. Another comprehensive systematic review of QT ACLR by Slone et al 46 included 14 studies and identified 3 patellar fractures without reporting any quantitative analysis of fracture rates.
Kanakamedala et al 23 investigated outcomes and complications of partial and full-thickness QT grafts after ACLR in a systematic review of 20 studies comprising 1212 patients. These authors reported that outcomes data were too heterogeneous for meta-analysis to be performed. However, the authors did report 2 patellar fractures with a reported total incidence of 0.7%. Both fractures occurred after partial thickness QT grafts with patellar bone blocks. In the present study, 12 patellar fractures associated with QT grafts were identified in 8 studies that explicitly reported the presence or absence of this complication. This allowed for a calculation of a pooled proportion of patellar fractures associated with a QT autograft harvest of 2.2%, which is notably higher than previously published. 23 While sample sizes remain limited, further investigations examining the incidence of patellar fractures during a BTB or QT graft harvest with ACLR are warranted.
Prior comparative meta-analyses of BTB and QT grafts have also evaluated donor-site morbidity in terms of knee pain and kneeling discomfort, identifying a lower risk of these complications with QT grafts in ACLR. 36,39 Mouarbes et al 36 analyzed 27 clinical studies encompassing 2856 ACLR patients and calculated a risk ratio of 0.25 in favor of QT grafts with regard to donor-site pain. The authors did not report data on patellar fractures or donor tendon ruptures. A similar meta-analysis by Riaz et al 39 included 5 studies of 806 patients, concluding that donor-site and kneeling pain were less frequent with QT ACLR compared with BTB ACLR with odds ratios of 0.1 and 0.16, respectively. No formal analysis of fracture risk or donor tendon rupture was reported. With the literature on donor-site pain symptoms sufficiently summarized in these 2 aforementioned meta-analyses, 36,39 the present study sought to analyze only fractures and donor tendon ruptures.
Additional areas of donor-site morbidity outside the scope of this review include anterior knee pain, kneeling pain, and anterior knee numbness, which may all be less frequent for QT grafts than BTB grafts. 16 These more subjective measures of morbidity were not analyzed because of heterogeneous reporting, the lack of a standardized assessment of those outcomes across studies, and existing meta-analyses previously published on the topic. 36,39 Consequently, this review was limited to specific, well-defined injuries and complications and should not be considered a comprehensive comparison of all complications related to the harvest and use of extensor mechanism autografts. Nevertheless, the narrower scope allowed for confident and accurate reporting of the pooled proportions of patellar fractures and donor tendon ruptures after autograft harvest.
Limitations
This study was not without limitations. There was a qualitatively elevated morbidity for QT autografts when compared with BTB autografts for both patellar fractures and donor tendon ruptures. However, the data should be interpreted with caution. Fewer quadriceps studies were available with fewer included patients and fewer total complications, increasing the relative effect of each injury on the pooled proportions and increasing the fragility of quantitative comparisons. There was a significant risk of selection bias because our inclusion criteria required a report of patellar fractures, patellar tendon tears, or quadriceps tears after ACLR. Because these complications are rare, the actual number of complications may be much lower. All data were extracted from published works, each with its own set of limitations. Namely, the level of evidence was heterogeneous, with only a minority (3.6%) of studies reporting level 1 data. Additionally, a small number of the studies included in this review were index cases with the knee extensor mechanism complications of interest. There is a significant risk of recall bias with the majority of studies reporting retrospective data. While there has been extensive research performed over the past 3 decades on surgical outcomes of ACLR with mentions of these complications after ACLR, the specific complications of interest were infrequently reported and, to our knowledge, no study has reported a meta-analysis of this information. More explicit attention to these complications in future published works would help to further clarify the relative risk of the QT and BTB harvest.
Conclusion
Based on the current literature, our study revealed that the proportion of extensor mechanism complications after ACLR using either a BTP or a QT autograft is low, indicating that the extensor mechanism harvest remains a safe option. A higher proportion of patellar fractures was noted for QT grafts than for BTB grafts. A higher proportion of donor tendon ruptures was noted for QT grafts compared with BTB grafts. Surgeons can use these data to better inform their patients on the relative morbidity of autograft options in ACLR.
Footnotes
Notes
Final revision submitted January 31, 2023; accepted March 9, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: N.A.T. has received grant support from Arthrex; education payments from Medwest, Smith & Nephew, and SouthTech Ortho; honoraria from Encore Medical; and hospitality payments from Stryker. D.M.K. has received grant support from Arthrex; education payments from Arthrex and Smith & Nephew; honoraria from Encore Medical; and hospitality payments from Stryker. B.J.C. has received education payments from Endo Pharmaceuticals and Medwest; consulting fees from Acumed, Aesculap, Arthrex, Endo Pharmaceuticals, Flexion Therapeutics, Ossio, Pacira Pharmaceuticals, and Vericel; speaking fees from Arthrex, Pacira Pharmaceuticals, and Terumo BCT; honoraria from Vericel; royalties from Arthrex; and hospitality payments from GE Healthcare. A.E.W. has received consulting fees from Stryker and speaking fees from Synthes. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.