
Abstract
Background:
Injury incidence is higher in the National Football League (NFL) than in other collision sports. Although previous research has identified that scheduling variations, including overseas games and bye week timing, does not affect concussion risk, data are currently lacking regarding the effects of scheduling variation on season-long musculoskeletal injury incidence.
Purpose:
To determine whether higher cumulative travel distance, overseas play, an early season bye week, and an expansion of the regular season is associated with higher injury rates in the NFL.
Study Design:
Descriptive epidemiology study.
Methods:
All 1275 injuries across 5 NFL seasons from 2017 to 2018 through 2021 to 2022 were reviewed retrospectively. Injury data and travel distances were extracted from publicly available sources, which were cross-referenced for validation. Injury rates were calculated per 1000 athletic-exposures (AEs). Cumulative team travel distances were compared statistically using a linear regression. Single factor analysis of variance was used to compare categorical variables.
Results:
Travel distance did not significantly predict injury rates (P = .47), and there was no difference in injury rates between teams that played a game overseas versus teams that did not (19.3 injuries per 1000 AEs for both; P = .96). In addition, no difference was found in injury rates (F[109,2100[ = 0.704; P = .73) or players placed on the injured reserve list (F[99,778] = 1.70; P = .077) between various bye weeks (P = .73). Injury rates did not differ between the new 17-game regular season (18.4 per 1000 AEs) versus the previous four 16-game regular seasons (19.7 per 1000 AEs; P = .12). However, teams that did not qualify for the playoffs had a significantly higher injury rate (19.9 per 1000 AEs) as well as players on injured reserve (8.0 per 1000 AEs) than playoff-qualifying teams (18.4 and 6.8 per 1000 AEs, respectively; P < .05 for both).
Conclusion:
Over 5 NFL seasons, cumulative travel distance, overseas play, bye week timing, and adding 1 regular season game were not associated with increased injury rates in NFL players. However, a lack of regular season success was associated with higher injury rates and more players on injured reserve.
The National Football League (NFL) is the among the most popular professional sport leagues in the United States. Injury incidence is higher in the NFL than in other team-based collision-heavy sports, including ice hockey and rugby. 20 Injuries to the lower extremity, including the knee, ankle, and hamstring, are the most common, followed by shoulder injuries and concussions. 3,20 From 2015 to 2018, a mean of 41% of NFL players had a time-loss injury to the lower extremity. 3,20,21 Defensive backs consistently have the highest number of all-cause injuries, time-loss injuries to the lower extremity, and in-game injuries among all positions. 3,21 Although technological advances and rule changes have been implemented over the past several years to curtail injury risk, 3,14 considerable concern remains regarding player safety.
There have been numerous investigations into the risk factors that contribute to the multifaceted etiology of NFL injuries. For example, significant ankle sprains, eversion ankle sprains of all severities, and anterior cruciate ligament sprains have been shown to occur more often in games played on artificial turf as opposed to natural grass, although 1 study found that there is a slightly greater risk of shoulder injuries on natural grass. 16,19,22,23 Evidence regarding temperature and injuries is mixed, with conflicting evidence regarding lower extremity injuries and 1 study reporting that colder temperatures may decrease concussion risk. 19,23 It has also been shown that more injuries occur on passing plays overall, though running backs and linemen are more likely to become injured on rushing plays. 11 Although it could be postulated that teams that must play on a shortened week for Thursday Night Football games (as opposed to the typical Sunday NFL games) may have increased injury incidence, 2 studies have shown that the number of days off between games is not associated with increased injury risk, with 1 of the studies demonstrating that the televised Thursday night games have fewer injuries than their weekend counterparts. 19,24
Regarding travel, 1 study found that defensive and offensive linemen who played in the Central time zone were placed on injured reserve more often than those from the Pacific time zone. 7 In contrast, although investigating the effect of a single trip rather than cumulative distance over the course of a season, studies in football and rugby found no association between relative distance traveled to games and injury risk in that game. 13,19 No association has been found between time of season, game outcome, altitude, or division opponents and injury risk. 19
Although some potential injury-promoting factors remain unknown in advance of competition, the scheduling characteristics of bye week timing, cumulative travel distance, and overseas games are known before the start of each season. It has been shown that unconventional schedules do not have an impact on concussion rates in the NFL. 28 However, there has not yet been a comprehensive analysis of the effect of scheduling factors on season-long musculoskeletal injury rates. This knowledge would be useful to NFL scheduling administrators, who could lead targeted scheduling initiatives to minimize the potential impact on player safety, and to team athletic trainers and physicians, who would be better prepared to assess athlete injury risk. Most importantly, this information would equip players to identify their own individual risk and initiate precaution to minimize potential harm. Players themselves have expressed their concern about injury risk. For example, the addition of a 17th regular season game to the schedule was a major player objection to the 2020 Collective Bargaining Agreement. 14
The present study addresses this gap in the literature by analyzing how scheduling factors may affect injury rates across 5 NFL seasons. The aim of the current study was to determine the relationship between scheduling factors and injury rates among professional athletes in the NFL. Based on the results of previous studies among other professional sports, 5,27 we hypothesized that higher cumulative travel distance, playing overseas games, having a bye week earlier in the season, and an expansion of the regular season would be associated with higher injury rates.
Methods
Injury surveillance
This study was a descriptive epidemiological study that retrospectively reviewed injuries in the 32 teams of the NFL across 5 seasons, from the 2017 to 2018 season through the 2021 to 2022 season. The study analyzed publicly available information and did not require institutional review board approval. Injury data extraction methods conformed to methods outlined in previous studies on the epidemiology of NFL injuries. 1 Injury data was extracted from a publicly available injury report (Pro-Football Reference, https://www.pro-football-reference.com/players/injuries.htm) and was cross-referenced with other publicly available sources (NFL, https://www.nfl.com/injuries and ESPN, https://www.espn.com/nfl/injuries). These methods are in line with previously published protocols. 1,2 The extracted data included player and team involved, week of the injury, playing status, games missed, and injured reserve status. This study only included sports-related musculoskeletal injuries that resulted in ≥1 missed games. Non–sports related medical issues, concussions, missed games due to personal reasons, and illnesses were excluded from the analysis. COVID-19 infections, and time lost due to COVID-19 infection, were also excluded from the analysis. Due to indistinguishable timing of injuries that occurred before the first regular season game, injuries and injured reserve placements that occurred before week 1 were excluded from the study.
Cumulative Travel Distance
Cumulative travel distance was defined as the total number of miles traveled in a given season from the team’s regular home stadium, which included playoff games. Distance was measured from the team’s regular home stadium and the stadium in which the game was played, analogous to the methodology used by Lawrence et al. 19 Games assigned a distance of zero included home games, road games against teams who share a stadium (ie, the 2019 New York Giants away game against the New York Jets), and the rare occasion of a team playing Super Bowl in its home stadium (the 2020 Tampa Bay Buccaneers and the 2021 Los Angeles Rams). For neutral site games (including the Super Bowl and games played at London’s Wembley Stadium, Twickenham Stadium, and Tottenham Hotspur Stadium, as well as Mexico City’s Estadio Azteca), travel distance was factored in for both sides. Likewise, the 2021 New Orleans Saints hosted their week 1 game against the Green Bay Packers in Jacksonville due to Hurricane Ida’s impact on New Orleans, 4 and the team's travel distance to Jacksonville’s TIAA Bank Field was included. The 2020 San Francisco 49ers hosted 3 games in Arizona’s State Farm Stadium due to local restrictions put in place during the ongoing COVID-19 pandemic, and in advance of their week 13 home game against the Buffalo Bills, it was announced that the 49ers would stay, practice, and play in Arizona for the remainder of the season. 8 Therefore, beginning with week 13, Arizona’s State Farm Stadium was considered the team’s “home stadium.” Thus, their 3 home games and a “road” game against the Cardinals afterward were assigned a distance of zero. Concurrently, distance traveled for their week 15 away game at AT&T Stadium in Dallas was calculated from State Farm Stadium in Arizona, rather than from Levi’s Stadium in San Francisco.
Statistical Analysis
In accordance with previous studies that analyzed injury rates in professional athletes, injury incidence was normalized per 1000 athlete-exposures (AEs), with 1 AE equal to 1 game per athlete. 1,25 AEs were calculated for each individual team per year as total injuries × 1000/AEs (53-player in-season roster size × number of games played). Data analysis was conducted using Microsoft Office Excel. Cumulative team travel distances were compared statistically using a linear regression. Single factor analysis of variance was used to compare categorical variables, with statistical significance set at P ≤ .05.
Results
There were 1275 regular and postseason games in the 5 NFL seasons between 2017 to 2018 and 2021 to 2022. Over the 5 seasons, 4378 injuries were reported, for a mean of 34.42 (30.58-39.26) injuries per 1000 AEs per year.
Cumulative team travel distance did not significantly predict the number of injuries per 1000 AEs (β = -6.1 × 10-5; P = .47) (Figure 1). Furthermore, there was no statistically significant difference in injury rates between NFL teams that did (19.3 injuries per 1000 AEs) versus did not (19.3 injuries per 1000 AEs) play a game overseas in their season (F[1,158] = [0.00242]; P = .96) (Figure 2).
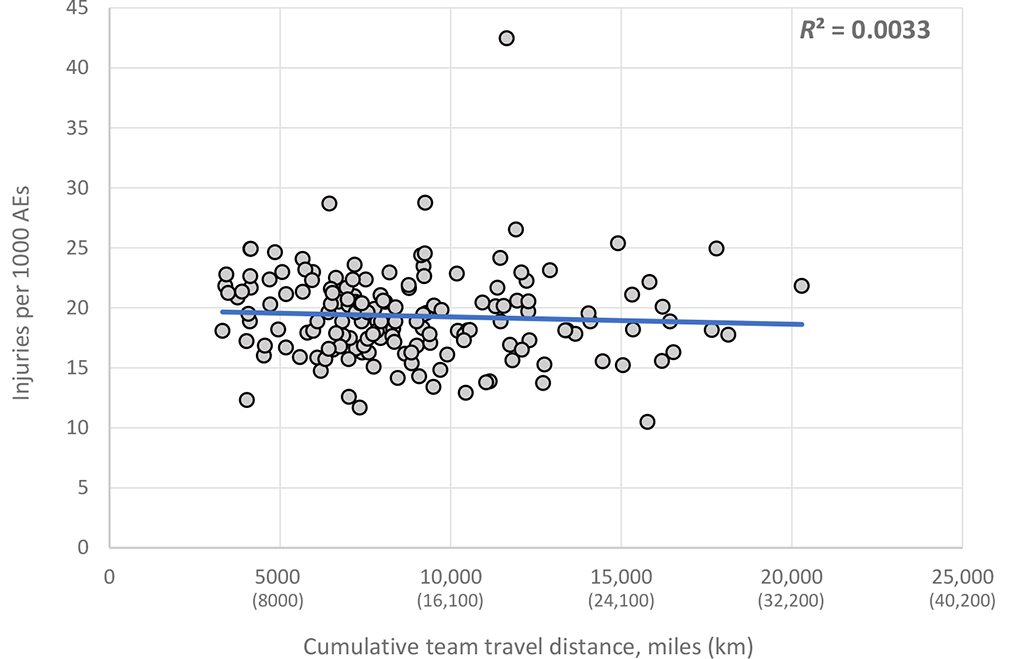
Cumulative team travel distance per season versus injuries per 1000 athletic exposures (AEs).

Injuries per 1000 athletic exposures (AEs) in National Football League teams that did versus did not play a game overseas in their season. Box represents 25-75th percentile, Line is median, x is mean, Dots are outliers, whiskers represent 1.5 x 25th-75th percentile interval.
In addition, there was no statistically significant difference in injuries per 1000 AEs between weeks that NFL teams had their bye week during the season (F[109,2100] = [0.704]; P = .73) (Figure 3A). Also, there was no statistically significant difference in the number of players on injured reserve per 1000 AEs between weeks that NFL teams had their bye week (F[99,778] = [1.70]; P = .077) (Figure 3B).

(A) Injuries per 1000 AEs between NFL bye weeks. (B) Number of players on injured reserve (IR) per 1000 AEs between NFL bye weeks. AE, athletic exposure; NFL, National Football League.
There was a statistically significant difference in injury rates between NFL teams that did (18.4 injuries per 1000 AEs) versus did not (19.9 injuries per 1000 AEs) make the playoffs (F[85,2126] = [6.28]; P < .05) (Figure 4A). There was also a statistically significant difference in the number of players on injured reserve per 1000 AEs between NFL teams that did (6.8 players on injured reserve per 1000 AEs) versus did not (8.0 players on injured reserve per 1000 AEs) make the playoffs (F[56,820] = [10.8]; P < .05) (Figure 4B). NFL teams that did not make the playoffs had higher mean number of injuries for every week, except the final week of the season (Figure 4C).

(A) Injuries per 1,000 AEs between NFL teams that did versus did not make the playoffs. (B) Number of players on injured reserve (IR) per 1000 AEs between NFL teams that did versus did not make the playoffs. (C) Mean number of injuries per week between NFL teams that did versus did not make the playoffs. Error bars in (C) represent SDs. *Statistically significant difference (P ≤ .05). AE, athletic exposure; NFL, National Football League.
The 2021 season with the new 17-game regular season had a total of 984 injuries, compared with a mean of 940 total injuries during the previous four 16-game regular seasons (2017-2020) (Figure 5). Subsequently, there was no statistically significant difference in injury rates between the new 2021 season (18.4 injuries per 1000 AEs) versus the previous 4 seasons (19.7 injuries per 1000 AEs), 2017 to 2020 (F[39,2177] = [2.45]; P = .12). In addition, there was no statistically significant difference in injury rates between the 5 seasons (Figure 5).

Injuries per 1000 athletic exposures (AEs) between 5 National Football League seasons.
Discussion
This study is the first to analyze the effects of various NFL scheduling factors on player safety with respect to musculoskeletal injury. Results suggest that cumulative travel distance (P = .47), playing a game overseas (19.3 vs 19.3 per 1000 AEs; P = .96), having a bye week earlier in the regular season (P = .73), and having a 17-game regular season (18.4 vs 19.7 per 1000 AEs; P = .12) were not associated with increased injury rates. By contrast, missing the playoffs was associated with an increase in injury rate (19.9 vs 18.4 per 1000 AEs; P < .05). The analysis suggests that the NFL schedule over the past 5 seasons was not a risk factor for increased musculoskeletal injuries. However, the results do suggest that not qualifying for postseason play was associated with higher injury rates.
There are currently over 1700 players in the NFL, with each of the league’s 32 teams being allotted a 53-player active roster and a practice squad of up to 16 players. In addition, lists such as injured reserve, the Physically Unable to Perform list, and the Reserve/Commissioner Exempt List comprise players under contract with NFL teams who do not count against these numbers. 17 Although the exact length has not been officially supported by the NFL, it has been reported that the mean length of players’ careers to be as short as 3 years. 15 Furthermore, multiple studies have demonstrated that musculoskeletal injury can be associated with shortening a player’s career. 6,9,10,18,26 For those able to play in the league longer, Domb et al 12 showed that their longer careers are associated with increased postcareer whole-person impairment via analysis of symptomatic joints. There is also a financial cost to sustaining an injury as an NFL player, as 1 study found that players with ACL injuries earned over 2 million dollars less in the ensuing 4 years than salary-matched controls. In addition, these injuries disproportionately affect career length for players with lower salaries. 26
Given the impact that injury can have on a player’s safety, livelihood, and postcareer quality of life, team physicians, athletic trainers, and athletes must be aware of any potential factors, including those inherent in a team’s schedule, that may put players at further risk of injury. This knowledge of injury risk factors is essential for prophylactic care. For free agents, awareness of such risks would likely be a significant factor in their selection of employer. The initial hypothesis of this study was that analyzed scheduling parameters were modifiable risk factors that have a significant effect on professional football players’ health-safety, as measured by incidence of musculoskeletal injuries.
Scheduling Parameters
Across the 5 NFL seasons between 2017 to 2018 and 2021 to 2022, there was no association between cumulative team travel distance and injury rates (Figure 1). Playing a game overseas during a season was not associated with an increase in injury rate (Figure 2). There was no significant difference in injury rates or number of players on injured reserve between the NFL bye weeks (Figure 3A,B). In addition, although only 1 season of data is currently available to measure the impact of the addition of a regular season game, initial analysis suggests the move from a 16- to a 17-game season did not increase injury rates (Figure 5).
These results do not support the initial hypothesis and suggest that the scheduling parameters analyzed are not risk factors for musculoskeletal injuries in the NFL. The results of this study echo findings from Teramoto et al 28 who found that scheduling considerations, including overseas games and bye week timing, did not increase the risk of concussions in the NFL. However, they do not align with studies of the National Hockey League (NHL) and National Basketball Association (NBA), which found an increased risk of injury with schedule condensation and away games on consecutive days, respectively. 5,27 This underscores the unique nature of the NFL schedule among American team sports, in which teams invariably play 1 game per week, half of which are at home, and therefore travel a maximum of once per week for half of the season. In contrast, an NBA or NHL team may play on consecutive days and multiple times per week in different cities. Previous research has shown that Thursday Night Football games, which are the NFL’s version of schedule condensation, are not associated with increased risk of injury, 19,24,28 and, although an early or late bye week is also a potential “schedule condenser” in the NFL, our results show that the timing of a team’s bye week does not have an impact on its incidence of musculoskeletal injuries or number of players put on injured reserve due to musculoskeletal injury.
Playoff Qualification
Not qualifying for the NFL postseason play was associated with both an increased injury rate and an increased number of players on injured reserve. However, no causative conclusions can directly be drawn from this analysis. It is possible that a decreased number of injuries may lead to improved team performance and subsequent playoff qualification. However, it is also possible that injury rates on successful teams may be underreported. On a successful team, each game holds high significance. Players on these teams may avoid missing critical games by playing through injury or underreporting injuries to avoid missing critical game time. In contrast, there is less incentive on unsuccessful teams for players to return to play and leave injured reserve, and teams that have been eliminated mathematically from postseason contention may be more likely to place players on injured reserve in the latter stages of the season. The current study’s results do highlight that a team’s competitive success is an important factor to consider when analyzing the epidemiology of sports injuries. Sports epidemiology studies that fail to control for team records may be misreporting the effect size of their measured parameters. Future investigation is necessary to elucidate the effect of team competitive success on reported injuries and player injured reserve status.
Limitations
Similar to other sports epidemiology publications that rely upon publicly available data, there are several limitations to the current study. The accuracy and precision of data collection methods for the database are not able to be verified, and potential omission of data may confound the study’s results. The data also lacked specific details about injury diagnoses, as factors such as severity and medical clearance were not available. Thus, the current study addresses only factors that affect time-loss musculoskeletal injuries of ≥1 game. It is possible that the measured parameters could be risk factors for more insidious injuries that do not remove an athlete from play. Furthermore, only musculoskeletal injuries were assessed; the study did not include all causes of time-loss injuries, as non–sports related medical issues, illnesses, and concussions were excluded from the analysis. A primary data source with direct medical information about injuries would alleviate these limitations. However, without direct collaboration with the NFL to access the players’ personal health information, the study’s well-established protocol represents the best available method for analyzing the epidemiology of professional football injuries. In addition, at the time of the conduction of the analysis, only 1 17-game season had been completed. Additional years of surveillance would aid in drawing stronger conclusions about whether the additional regular season game has implications for NFL injury rates. However, insights from the initial analysis of the schedule change are still beneficial to the athletes that will continue to play with the new schedule as more data are collected. Finally, the study’s sample size of 32 NFL teams over 5 seasons, for a total of 1275 regular and postseason games, helps minimize bias in this retrospective data analysis.
Conclusion
Over 5 NFL seasons, cumulative travel distance, overseas play, bye week timing, and adding 1 regular season game were not associated with increased injury rates in NFL players. However, a lack of regular season success was associated with higher injury rates and more players on injured reserve. Overall, the analysis suggests that the analyzed parameters in the current NFL schedule were not risk factors for musculoskeletal injuries over the past 5 seasons, although lack of regular season success was associated with higher injury rates and more players on the injured reserve list.
Footnotes
Final revision submitted January 27, 2023; accepted March 9, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: V.K.T. has received education payments from Medwest Associates and consulting and nonconsulting fees from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.