
Abstract
Background:
The role of meniscal lesions and repair in combination with anterior cruciate ligament (ACL) injury and reconstruction has not been extensively investigated in vivo and under weightbearing conditions.
Purpose:
The purposes of this study were to (1) compare the in vivo knee kinematics between patients with ACL tear and those with combined ACL and medial meniscal tears and (2) investigate kinematic differences between isolated ACL reconstruction and ACL reconstruction plus medial meniscal repair (MR). It was hypothesized that concomitant posterior horn medial meniscal tear and ACL deficiency would affect knee internal-external rotation and anterior-posterior translation but MR would restore these parameters.
Study Design:
Controlled laboratory study.
Methods:
Nineteen patients who underwent ACL reconstruction were included: 10 had intact menisci (IM group) and 9 had a medial meniscal injury that was repaired during ACL reconstruction using an all-inside technique (MR group). Preoperatively and 18 months postoperatively, active knee kinematics under weightbearing conditions was evaluated during a single-leg squat using a dynamic biplane x-ray imaging system. The general linear model was used to investigate the differences between group (IM vs MR) and time (preoperative vs follow-up) and their interactions.
Results:
Tibial internal rotation was higher in the MR group than the IM group both before and after surgery (P = .007). Knee valgus rotation was higher in the MR group preoperatively (P < .001), while no differences were found postoperatively because of an increase of valgus rotation in the IM group, which was significant in the descendant phase (P < .001). Preoperatively, the IM group showed a more medial tibial translation compared with the MR group in the descendant phase (P = .006).
Conclusion:
When performing a single-leg squat, patients with ACL-deficient knees and a medial meniscal tear demonstrated a more valgus rotation, tibial internal rotation, and lateral tibial translation versus those with intact menisci. After ACL reconstruction and MR, these patients demonstrated significantly higher tibial internal rotation when compared with patients who underwent isolated ACL reconstruction.
Clinical Relevance:
Surgeons should be aware that MR does not fully restore knee kinematics in vivo and under weightbearing conditions in the context of ACL reconstruction.
The role of meniscal tear in the context of anterior cruciate ligament (ACL) injury and reconstruction is a debated topic, and for some authors, the status of the meniscus may have a fundamental prognostic role, because involvement of the meniscus is related to worse clinical scores and a higher risk of osteoarthritis development. 12,24 Moreover, several biomechanical studies demonstrated that the menisci play a role as knee stabilizers. 2,28 For these reasons, procedures aimed at preserving the menisci are preferred to partial meniscectomy, if permitted by the tear pattern. 2,9,21,29
Although the role of meniscal tear, meniscal repair (MR), or meniscectomy in influencing knee biomechanics has been widely investigated, 2,3,7,11,14,26,29,31,33 there is limited evidence of the biomechanical consequence of concomitant ACL and meniscal injuries, especially in vivo and under weightbearing conditions. Thus, it is difficult to draw a definitive conclusion about the topic. 3
Few studies have investigated the kinematic role of meniscal injury in vivo. Among them, Akpinar et al 3 demonstrated that a concomitant injury of the medial meniscus in the context of ACL reconstruction causes a more anterior tibial position in the initial 10% of the gait cycle during downhill running. Their results were in contrast to ones by Hall et al, 14 who reported no differences between ACL-reconstructed knees with or without a concomitant meniscal tear. These 2 studies had a substantial limitation; both of them analyzed in a unique group the kinematic data of MRs, meniscectomy, or untreated tears. Furthermore, the second study is based on motion capture based on on-skin markers, which are affected by movement artifacts, which can be up to 65% of the true translation and rotation of the joint. 4 For all these reasons, there is a lack of studies designed to accurately investigate the biomechanical effect of medial meniscal tears and repair on knee kinematics during in vivo activities.
The aims of the present study were to (1) compare in vivo knee kinematics of ACL tear with combined ACL and medial meniscal tears and (2) investigate differences between isolated ACL reconstruction and ACL reconstruction plus medial MR. We hypothesized that (1) concomitant posterior horn medial meniscal tear would influence knee internal-external rotation 13 and anterior-posterior (AP) translation, and (2) meniscal repair would restore these parameters.
Methods
This study represents the secondary analysis of data collected from a prospective study, the purpose of which was to evaluate the outcomes of ACL reconstruction. The study protocol received institutional review board approval, and all included patients provided written informed consent. This study was registered on ClinicalTrials.gov (ID: NCT02323386).
The inclusion criteria for the original study were age 16 to 50 years; complete and unilateral ACL injury; no previous knee ligament reconstruction or repair; no concomitant posterior cruciate ligament, posterolateral corner, lateral collateral ligament, or medial collateral ligament lesion; and absence of mild or advanced knee osteoarthritis (Kellgren-Lawrence grades 3 and 4). 17 For the purposes of the present study, the inclusion criteria were patients who underwent ACL reconstruction and who had either intact menisci or a medial meniscal injury that was surgically repairable. Excluded were patients who had concomitant other ligamentous injuries, lateral meniscal tear, irreparable medial meniscal tear, or incomplete kinematic data and those unwilling to take part in the study. Of 66 patients available from the original study, 19 patients met all inclusion criteria, completed the pre- and postoperative kinematic assessments, and were included in the final analysis (Figure 1).
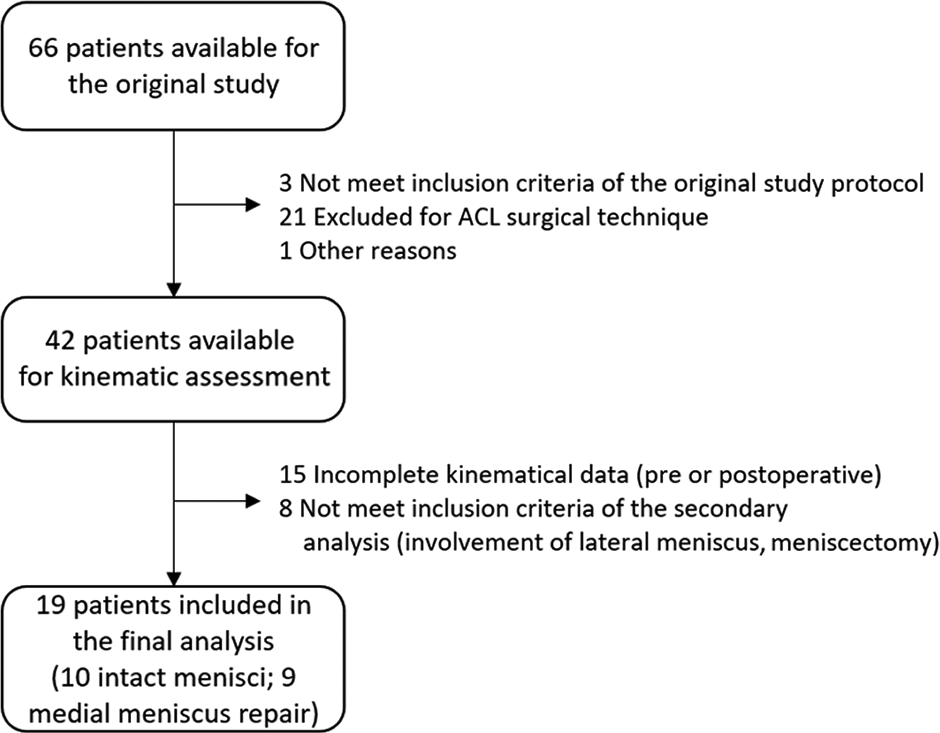
STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) diagram of the study. ACL, anterior cruciate ligament.
Surgical Procedure
A routine arthroscopic examination was performed to confirm the diagnosis of ACL injury and to assess meniscal status. Patients affected by reparable medial meniscal tear involving the posterior horn were allocated to the MR group, and patients with an isolated ACL injury and intact menisci were allocated to the intact meniscus (IM) group.
The location and stability of the tears were evaluated through an arthroscopic probe. All the patients in the MR group underwent an all-inside technique repair using the FasT-Fix all-inside meniscal suture device (Smith & Nephew Endoscopy). Following the manufacturer’s recommendations, before the repair, the edges of the tear were rasped using motorized instrumentation. After the repair, the stability of the repaired meniscus was assessed with a probe. Subsequently, patients underwent anatomic single-bundle ACL reconstruction with autologous hamstrings or over-the-top plus lateral extra-articular tenodesis ACL reconstruction described by Marcacci et al, 22 depending on the randomization of the original study protocol. A single experienced surgeon (S.Z.) performed all surgeries; he was not aware of the purposes of the study at the time of the surgery.
Rehabilitation
The rehabilitation protocol was the same for all the patients. No knee brace was used. Isometric quadriceps exercises and prone hamstring muscle stretching were begun on the first day after the surgery. Passive and active flexion-extension was begun on the third postsurgical day, initially limited to 30° of flexion, increasing 5° every day up to 90°; from the fourth week complete range of motion was permitted. Weightbearing was partially allowed in the first 2 weeks (about 20% of body weight), from the third week a progressive increase of bearing was allowed, and the patients reached complete weightbearing in the fourth week. Cyclette (stationary bike), active knee extension with weights, and one-quarter squats were introduced 4 weeks after surgery. Running on the treadmill was introduced at 2 months and more aggressive strengthening and sport-specific activities after 4 months. Return to competitive sport usually was not completed before the sixth month.
Magnetic Resonance Imaging Evaluation
Magnetic resonance imaging (MRI; 1.5 T) of the knees was acquired before surgery and at a minimum of 18 months after surgery. Tridimensional models of the femur and the tibia were extrapolated from sagittal T2-weighted sequences through dedicated software (Slicer Version 4.10.1; Slicer, Brigham and Women’s Hospital, Harvard University, NIH); the models were then used for kinematic data acquisition. Two experienced orthopaedic surgeons (A.G., S.Z.) evaluated postoperative MRI scans to estimate the healing of meniscus; T2-weighted and proton density sequences were used for this purpose. None of the patients showed no healing of the repaired tear. 32
Data Acquisition
We used a dynamic biplane x-ray imaging system (roentgen stereophotogrammetric analysis [RSA]) for data acquisition. Each patient performed a series of single-leg squats in a radiographic room equipped with 2 x-ray sources placed so that the beamlines were perpendicular to each other and synchronized to acquire a pair of simultaneous radiographs (8 frames per second). The specifics of the radiographic setup were analogous to those used in previous studies 1,6,13,25 : detector dimensions were 43 × 43 cm with a pixel matrix of 1440 × 1440 pixels, and each beamline had the source-to-detector distance set to 180 cm. Each patient performed 3 repetition tasks. To limit exposure to the x-rays, the radiographs were collected only for the third repetition. The patients were asked to maintain their foot in neutral alignment. After the motor task, radiographs of the calibration cage were acquired to perform the data analysis and a 3-dimensional (3D) reconstruction of the RSA scene.
The radiographs were then matched with 3D bone models of the femur and tibia obtained from a 1.5-T MRI system per each frame acquired (Figure 2). The 6 degrees of freedom kinematics was calculated through the Grood and Suntay decomposition in MATLAB (Version R2016a; MathWorks Inc). The workflow had been validated in previous studies in terms of accuracy (0.22 ± 0.46 mm and 0.26° ± 0.2° for the model position and orientation, respectively) and test-retest reliability (mean error, <0.48 mm [95% CI, 0.15-0.80 mm]). 1,5,6,13,15,25

Roentgen stereophotogrammetric analysis data elaboration: 3-dimensional models of bones were obtained from magnetic resonance imaging and were used in specific software to reproduce the joint movement through a validated tracking system that matched models and dynamic radiographs. The pink points correspond to the position of the markers needed for the virtual reconstruction of the radiological setup where the motor task was acquired.
Kinematic data were normalized to the peak knee flexion angle and divided into a descendant phase (from the initial standing position to peak knee flexion) and an ascendant phase (from peak knee flexion to the final standing position). The internal-external and varus-valgus rotation, and the AP and medial-lateral translation were processed.
Statistical Analysis
Knee kinematic data were presented as means and standard errors over the knee flexion angles, separately for the descendant and ascendant phases of the single-leg squat. Data were grouped every 15° of knee flexion for conciseness in presentation (eg, 0°-15°, 15°-30°, 30°-45°, and 45°-60° for the descendant phase).
The general linear model was used to assess the statistical differences between the groups in a repeated-measures design, with time (preoperative vs follow-up), group (IM vs MR), and time × group interaction effects. The partial eta-squared (ηp 2) measure was reported alongside the P value and was considered small, medium, and large for values of 0.01, 0.06, and 0.14, respectively. The 2-tailed Student t test was used to assess between-group differences, and the paired Student t test was used to assess within-group differences with Bonferroni correction for post hoc comparisons. Differences were considered statistically significant for P < .05.
The sample size was in line with previous studies with analogous methodology and was based on a priori power analysis performed in G*Power (Erdfelder, Faul & Buchner; Version 3.1). 1,13 A minimum of 7 patients was required to obtain a power of 0.8 with a difference of 3.8° ± 2.3° in internal-external rotation and an alpha level of .05. All the statistical analyses were performed in MATLAB.
Results
There were 10 patients in the IM group (8 male; mean age, 24.7 ± 5.5 years) and 9 patients in the MR group (all male; mean age, 28.7 ± 11.7 years). Meniscal lesions consisted of 2 at the body and posterior horn and 7 at the posterior horn. The mean follow-up time was 21.5 ± 3.2 months.
Kinematics
Rotations
Preoperatively, patients in the MR group showed greater tibial internal rotation compared with the IM group during the entire movement (large effect size; P < .001) (Table 1, Figure 3A). Greater tibial internal rotation in the MR group persisted at follow-up in the descendant phase (mean difference [MD], –2.1° to –6.2°; P = .008) (Appendix Table A1, Figure 3A).
Internal-External Tibial Rotation During the Single-Leg Squat a

a GLM, general linear model; IM, intact meniscus; MR, meniscal repair; NS, not significant; Preop, preoperative.
b Values are presented as mean (SEM). Positive values indicate internal rotation.

Graphical representation of the kinematic parameters investigated: (A) internal-external rotation, (B) varus-valgus rotation, (C) anterior-posterior translation, and (D) medial-lateral translation. Asterisks indicate statistically significant differences (P < .05). Error bars indicate standard error. Note the preoperative differences in internal-external rotation, varus-valgus rotation, and medial-lateral translation between the 2 groups and the persistence of greater tibial internal rotation after surgical intervention (descendant phase). FU, follow-up; PRE, preoperative.
A greater valgus rotation was observed in the MR group compared with the IM group preoperatively (medium to large effect size; P = .009) (Table 2, Figure 3B). Greater valgus rotation at follow-up was noted in the IM group in the descendant phase between 15° and 45° (MD, 3.9°-4.5°; P < .001) (Appendix Table A2, Figure 3B).
Varus-Valgus Rotation During the Single-Leg Squat a
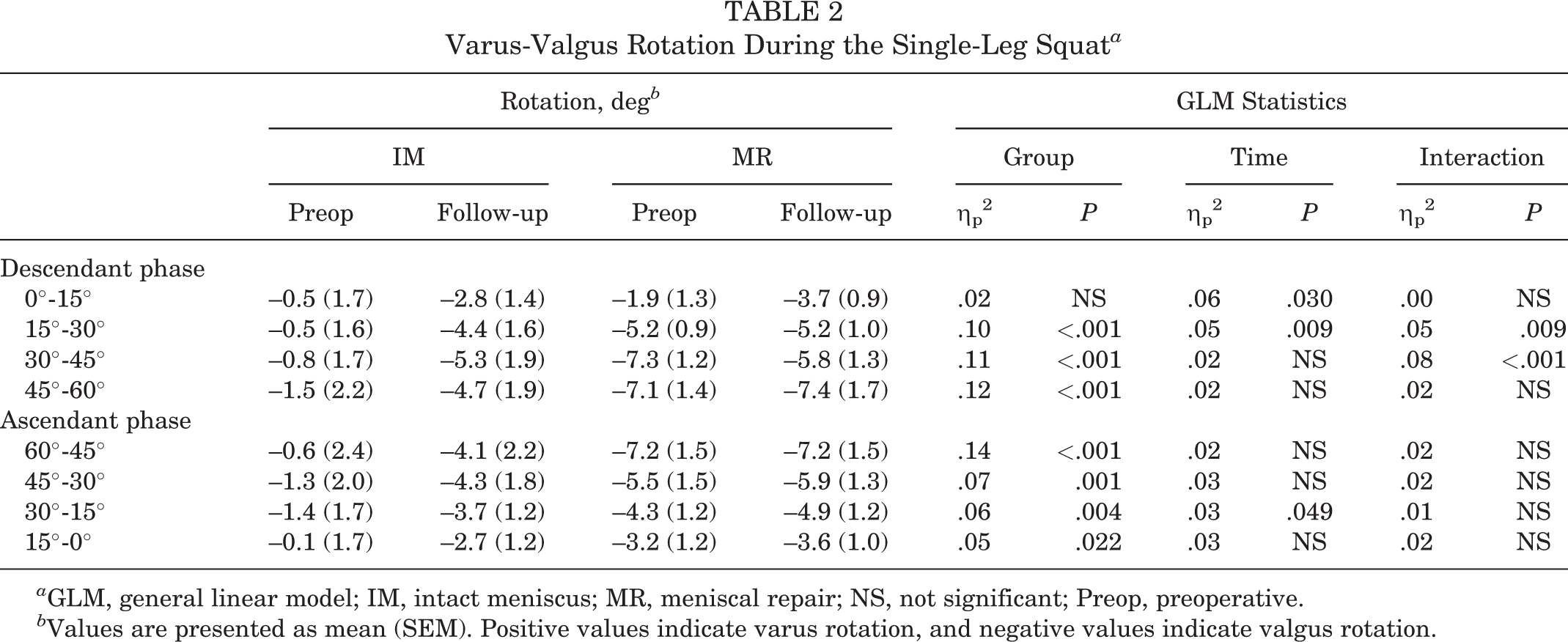
a GLM, general linear model; IM, intact meniscus; MR, meniscal repair; NS, not significant; Preop, preoperative.
b Values are presented as mean (SEM). Positive values indicate varus rotation, and negative values indicate valgus rotation.
Translations
In the MR group, a less anterior tibial translation at 15° to 30° of knee flexion (MD, 5.0 mm [95% CI, 0.7-9.4 mm]; P = .015) and greater anterior tibial translation at 60° to 45° (MD, –3.6 mm [95% CI, –6.6 to –0.5 mm]; P = .014) were noted at follow-up compared with preoperatively (Table 3, Figure 3C, Appendix Table A3). MR group patients also showed less anterior translation at 60° to 45° compared with the IM group preoperatively (MD, 4.0 mm [95% CI, 0.9-7.1 mm]; P = .005).
Anterior-Posterior Tibial Translation During the Single-Leg Squat a
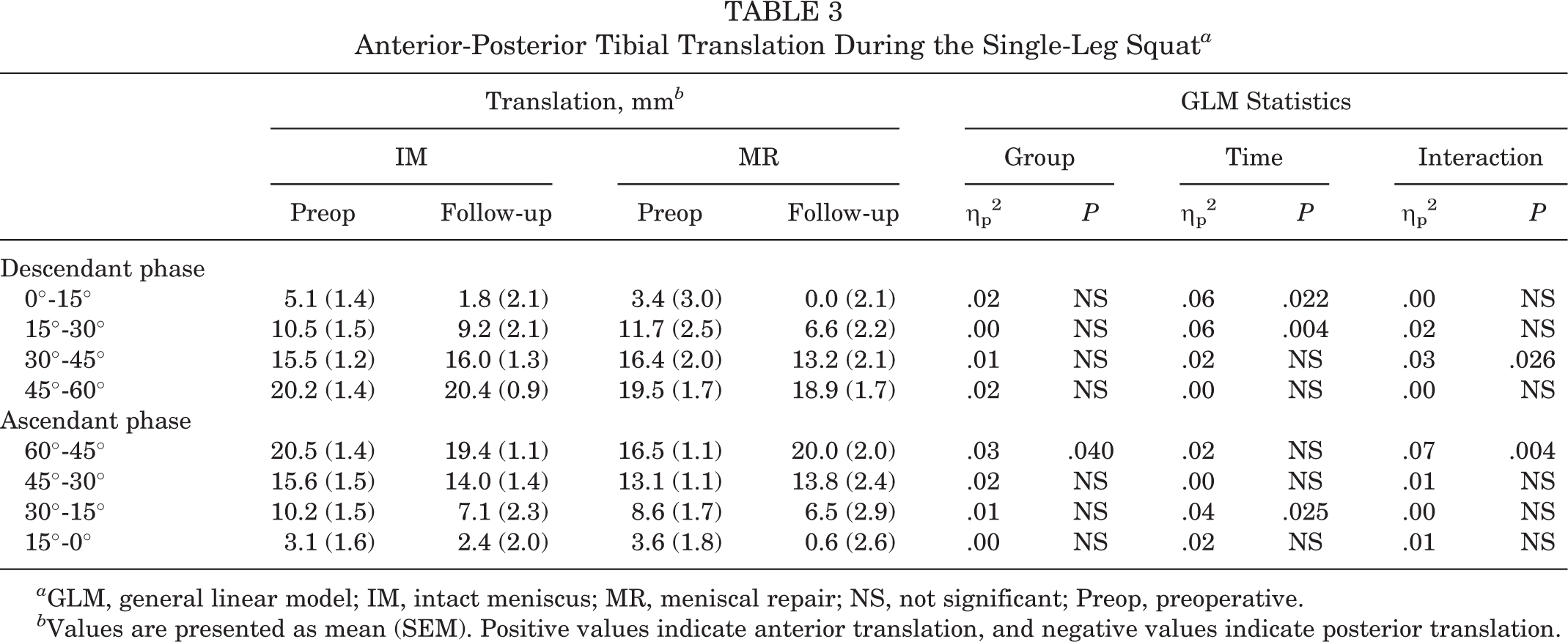
a GLM, general linear model; IM, intact meniscus; MR, meniscal repair; NS, not significant; Preop, preoperative.
b Values are presented as mean (SEM). Positive values indicate anterior translation, and negative values indicate posterior translation.
A more medial position of the tibia was observed preoperatively in IM group patients compared with the IM group at follow-up (MD, 2.0-2.8 mm; P < .001) and the combined MR group preoperatively (MD, 2.0-2.3 mm; P = .006) in the descendant phase (Table 4, Figure 3D, Appendix Table A4).
Medial-Lateral Tibial Translation During the Single-Leg Squat a

a GLM, general linear model; IM, intact meniscus; MR, meniscal repair; NS, not significant; Preop, preoperative.
b Values are presented as mean (SEM). Positive values indicate medial translation, and negative values indicate lateral translation.
Discussion
The main findings of the present study were that a medial meniscal posterior horn tear was associated with altered knee kinematics in ACL-deficient knees versus knees with intact menisci, in terms of more internal and valgus rotation and lateral tibial translation; after ACL reconstruction, patients who underwent concomitant meniscal suturing showed a persistent tibial internal rotation. Thus, the first hypothesis was partially confirmed, while the second one was proven wrong.
The medial meniscus is believed to be a secondary restraint of the anterior knee laxity, with a relevant role in the case of ACL deficiency. 19 The posterior horn could be considered the main stability agent, as demonstrated by the cadaveric study with the robot by Ahn et al. 2 However, most of the biomechanical knowledge derives from cadaveric studies or from in vivo studies performed in static conditions. 9,27 To our knowledge, this is the first study that analyzed the effects of medial MR on knee kinematics in the context of ACL injury with a highly accurate tool, based on a biplane radiographical system.
Motion capture systems have provided new insight into the biomechanics of the meniscus. Hall et al 14 found no gait differences between patients with and those without meniscal injury 16 months after ACL reconstruction. Conversely, Akpinar et al 3 demonstrated that patients with associated medial meniscal injury had an increased anterior tibial translation 24 months after ACL surgery, in performing downhill running. The second study was based on a more accurate tool and investigated a more stressful motor task. This could explain the different findings they reported. The main limitation of both studies was that the authors did not analyze patients with meniscal tears in subgroups according to the treatment performed. Our data were in contrast with the above mentioned, because our data revealed preoperatively a more anterior tibial position for the IM group at the beginning of the squat ascendant phase. However, the motor task investigated by the present study was substantially different because the squat is a closed-chain activity, while walking and running are open-chain activities. Moreover, previous studies demonstrated no influence of ACL deficiency in AP tibial translation during the squat, probably because of a stabilizing effect of quadriceps and hamstring co-contraction in executing the motor task. 1,18
In the present study, the combined lesions of the ACL and the posterior horn of the medial meniscus caused a significant increase in knee tibial internal rotation when compared with isolated ACL tear. The recently increased interest in ramp lesions has highlighted the new concept of the posterior portion of the medial meniscus as a restraint of knee rotatory laxity. 11,23 However, previous gait analysis studies demonstrated no differences in knee rotation between medial MR and intact menisci in ACL-reconstructed knees. 7,31 The latter was performed with motion capture tools based on optical devices and skin markers; thus, more investigations are needed to understand if MR in ACL-reconstructed knees leads to altered rotations only in selected motor tasks with highly accurate tools. The influence of medial meniscectomy on gait has been already proved by Wang et al, 31 who showed a significantly larger tibial external rotation in patients who underwent partial medial meniscectomy with respect to intact menisci or medial MR. Interestingly, the authors also registered an increased anterior tibial translation in patients with meniscectomy and, to a lesser degree, also in the MR group. Thus, a suboptimal result of MR in restoring sagittal laxity could be speculated.
In the present study, differences among the investigated groups were reported for varus-valgus preoperatively, in terms of a more varus rotation for the IM group; moreover, the same group showed a significant increase of knee valgus at follow-up. This finding could be considered in contrast with previous studies that reported increased adduction during gait in the case of partial medial meniscectomy. 7,31 However, the preoperative difference seemed to be related to a more varus rotation in the IM group rather than a more valgus rotation in the MR group; in fact, the difference postoperatively disappeared because of an increase of valgus rotation in the IM group. This finding was difficult to explain and probably derived from confounding factors, such as the role of ACL in constraining varus 1,13 and the role of knee flexion and axial load in eliciting meniscal tear pain. 16 With regard to the second factor, the squatting position was proven to elicit pain in the case of medial meniscal posterior horn tear 8,30 ; in this context, the coronal knee rotation could vary in order to reduce symptoms. Thus, our opinion is that ACL deficiency is the cause of more varus, while the medial meniscus involvement leads to translating the forces on the lateral plateau to avoid pain. These factors probably covered the real kinematic effect of medial meniscal lesions and repair on varus-valgus rotation.
The other parameter that differed only preoperatively was the mediolateral alignment. A more medial tibial position was found in the patients with an intact medial meniscus compared with patients with meniscal tears preoperatively. Previous papers investigated the role of ACL injury and medial meniscal tear in mediolateral knee alignment. The isolated ACL deficiency was proved to cause a medial shift of the tibia under weightbearing 1,10,20 ; moreover, a previous study of gait analysis proved that, although isolated ACL injury caused tibial medial translation, curiously, the association between ACL and medial meniscal tear caused a mediolateral alignment similar to that of the healthy status. 33 Based on the abovementioned evidence, it could be speculated that a medial meniscal tear entails lateralization of the tibia, while on the contrary ACL injury causes a tibial medialization.
Limitations
There are several limitations to this study. The first one is the small sample size; however, the high accuracy of the biplane x-ray–based motion capture system permitted the identification of significant differences among the groups investigated. Moreover, failure of meniscal suturing in the MR group could not be arthroscopically excluded at the follow-up time. However, there were no signs suggestive of meniscal treatment failure on MRI, and an arthroscopic second look would be unethical in the absence of clinical indication. Another limitation was the presence of 2 different surgical techniques for ACL reconstruction, but a previous study demonstrated no kinematic differences in performing a single-leg squat for this procedure. 13 In addition, the motor task investigated could be considered a limitation of the study, because the squat did not permit us to appropriately investigate the AP knee laxity; however, interesting kinematic findings were discovered, especially regarding the role of the medial meniscus in providing rotational stability and appropriate coronal alignment. Lastly, confounding factors such as meniscal pain could have influenced kinematic data, leading to results not strictly related to meniscal biomechanics. However, the strength of the present study resides in its being an in vivo investigation under weightbearing, and most of the knowledge about biomechanics of menisci derived from in vitro studies, although not influenced by clinical factors, was affected by the absence of loading and muscular activation.
Conclusion
In patients with medial meniscal posterior horn tear and ACL deficiency, the knees showed a more valgus rotation, tibial internal rotation, and tibial lateral translation in performing a single-leg squat when compared with patients with isolated ACL injury. For the same motor task, after ACL reconstruction, patients with the concomitant presence of repaired medial meniscal tear demonstrated higher tibial internal rotation.
Footnotes
Final revision submitted February 4, 2023; accepted March 9, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding was received from the Italian National Health Service to perform this study. S.Z. has received consulting fees from De Puy Synthes and Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from IRCCS Istituto Ortopedico Rizzoli (ID: 40/CE/US/ml).