
Abstract
Background:
In patients with osteochondral lesion, defects of the medial talus, or failed cartilage surgery, a periarticular osteotomy can unload the medial compartment.
Purpose:
To compare the effects of supramalleolar osteotomy (SMOT) versus sliding calcaneal osteotomy (SCO) for pressure redistribution and unloading of the medial ankle joint in normal, varus-aligned, and valgus-aligned distal tibiae.
Study Design:
Controlled laboratory study.
Methods:
Included were 8 cadaveric lower legs with verified neutral ankle alignment (lateral distal tibial angle [LDTA] = 0°) and hindfoot valgus within normal range (0°-10°). SMOT was performed to modify LDTA between 5° valgus, neutral, and 5° varus. In addition, a 10-mm lateral SCO was performed and tested in each position in random order. Axial loading (700 N) of the tibia was applied with the foot in neutral alignment in a customized testing frame. Pressure distribution in the ankle joint and subtalar joint, center of force, and contact area were recorded using high-resolution Tekscan pressure sensors.
Results:
At neutral tibial alignment, SCO unloaded the medial joint by a mean of 10% ± 10% or 66 ± 51 N (P = .04) compared with 6% ± 12% or 55 ± 72 N with SMOT to 5° valgus (P = .12). The achieved deload was not significantly different (ns) between techniques. In ankles with 5° varus alignment at baseline, SMOT to correct LDTA to neutral insufficiently addressed pressure redistribution and increased medial load by 6% ± 9% or 34 ± 33 N (ns). LDTA correction to 5° valgus (10° SMOT) unloaded the medial joint by 0.4% ± 14% or 20 ± 75 N (ns) compared with 9% ± 11% or 36 ± 45 N with SCO (ns). SCO was significantly superior to 5° SMOT (P = .017) but not 10° SMOT. The subtalar joint was affected by both SCO and SMOT, where SCO unloaded but SMOT loaded the medial side.
Conclusion:
SCO reliably unloaded the medial compartment of the ankle joint for a neutral tibial axis. Changes in the LDTA by SMOT did not positively affect load distribution, especially in varus alignment. The subtalar joint was affected by SCO and SMOT in opposite ways, which should be considered in the treatment algorithm.
Clinical Relevance:
SCO may be considered a reliable option for beneficial load-shifting in ankles with neutral alignment or 5° varus malalignment.
Keywords
Osteochondral lesions of the talus (OLT) are common injuries in recreational and professional athletes, with the medial talar dome affected in up to 62% of cases. 6,21 Several surgical treatment modalities exist, such as microfracturing, 3,7,27 osteochondral autograft, 8,10,11,23 allograft, 9 transplantation, and autologous matrix-induced chondrogenesis, 28 all with varying success rates. In case of axis deformity, concomitant realignment surgery decreases local overload. 29 Ankle deformity is defined as follows: lateral distal tibia angle (LDTA) of >89° ± 3° (supramalleolar deformity), ≥10° of hindfoot valgus, or >0° of hindfoot varus (inframalleolar deformity). 26,29 Dictated by the location of the deformity, malalignment can either be addressed with a sliding calcaneal osteotomy (SCO) 5,24,26,29 or a supramalleolar osteotomy (SMOT). 14 Both options have proven successful in unloading the affected area and redistributing the pressure.
While previous applications focused mainly on asymmetric ankle osteoarthritis 1 or pes cavovarus, 22 there are no studies on the beneficial load-shifting effect in ankles without malalignment. Therefore, the purpose of this cadaveric study was to quantify the pressure redistribution after SMOT and SCO in the ankle joint as well as subtalar joint with neutral tibiotalar alignment. The goal was to investigate whether a concomitant realignment surgery might create a protective environment for improved cartilage healing. The hypothesis was that both osteotomies would comparably unload the medial ankle joint, but SMOT would limit any changes in the subtalar joint.
Methods
Specimen Preparation
The study protocol received ethics committee approval, and all testing procedures and specimen storage, handling, and disposal were performed according to institutional and international guidelines. A total of 8 fresh-frozen cadaveric lower leg and foot specimens (from 8 independent donors; knee exarticulated) were obtained from MedCure Inc and stored deep-frozen in our on-campus research facility. Before dissection, thawed specimens underwent computed tomography to confirm adequate bone quality and anatomic distal tibial alignment (LDTA of 89° ± 3°). 18 Exclusion criteria were as follows: osseous malalignment (eg, LDTA of >89° ± 3°), subtalar or ankle joint osteoarthritis (Takakura stage <2), limited ankle range of motion (<30°), talar tilt of >4°, 4,13 or inadequate bone mass density.
Biomechanical Setup
The lower leg was fixed in a customized testing frame (Figure 1). The foot was fixed in neutral position to the base plate by 2 mm Kirschner wires through the head of the first metatarsal and through the base of the fifth metatarsal, respectively. Leaving the heel free allowed compensatory translation of the calcaneal tuberosity when load was applied after SMOT. 14 Soft tissue was removed while preserving capsular and ligamentous structures. Arthrotomy of the ankle and subtalar joint was performed (while preserving the medial and lateral ligament complex) to place Tekscan pressure sensors in a standardized manner, which were then fixed with 2 mm Kirschner wires.

Biomechanical test setup: MicroScribe digitizer (left); Tekscan pressure sensors (right); external fixator device for change of supramalleolar osteotomy.
For the SMOT, a medially based 5° wedge of the tibia was removed, preserving the fibula and the lateral cortex of the tibia, and was fixed with an external fixator. 19,20 Herewith, LDTA was modifiable between 5° valgus, neutral (0°), and 5° varus. A correction in degrees was confirmed by MicroScribe MX digitizer (Revware Inc) by tracing the end points of the Schanz pins of the external fixator and measuring the change in the angle between the superior and inferior Schanz pins projected on the frontal plane. A standard oblique SCO was performed, perpendicular to the axis of the calcaneus; 10 mm lateralization was confirmed using a ruler. Fixation was achieved with two 6.5-mm spongiosa screws.
Biomechanical Testing
Testing work flow was randomized within the SMOT and SCO conditions (LDTA at 5° valgus, neutral [0°], and 5° varus). The proximal tibia was mounted in a uniaxial material testing machine (Zwick 1456; Zwick/Roell) equipped with a 20-kN load cell (Serie K; GTM Testing and Metrology GmbH). The force and displacement data were recorded at 10 Hz with the dedicated software (TestXpert Version 10.11; ZwickRoell). Limbs were preconditioned from 0 to 50 N for 20 cycles and then loaded to an ultimate load of 700 N at a speed of 1 mm/s, which corresponds to the body weight of a 75 kg person. 14 The loading was performed at 0° of flexion and was maintained for 20 seconds to allow for pressure recordings. This was followed by unloading.
Pressure-sensitive films (sensor No. 4000; Tekscan Inc) were used to capture pressure readings during loading at 4 Hz, the last 5 seconds of the recording was averaged to calculate center of force (defined as the location on the plane of the film at which the resultant force integrated from the distributed load acts), contact area, and pressure in the ankle and subtalar joint. Each sensor was calibrated after loading for 15 seconds using a 2-point calibration at 500 and 700 N. Sensors were split into equal medial and lateral sides along the midline of the sensor to assess the unloading of the medial side.
Outcome Measures
The primary outcome measure was the change in percentage of load on the medial side with respect to baseline, which was defined as neutral and 5° varus alignment in the ankle joint. The comparison of medial-side loads between reference and treatment conditions was not reported due to lack of clinical applicability. For daily clinical use, it was of greater interest to calculate the change in percentages and thereby compare the different treatment conditions with each other. Secondary outcome measures were the lateral shift in center of force from baseline calculated in the ankle joint and the change in percentage of load on the medial side with respect to the baseline in the subtalar joint. Calculation of mechanical parameters was performed with MATLAB (Release 2021a; The MathWorks, Inc).
Statistical Analysis
A power analysis based on a previous study showed a power of 86.5% with 6 specimens to detect a difference of 1 N/mm2 with a standard deviation of 0.8 and a significance level of .05, when 2-sided testing was selected. 14 In another study, lateral SCO led to a 4% increase in the average percentage pressure transmitted through the lateral joint compartment, which was statistically significant using 6 specimens. 5 Therefore, 8 specimens were tested for the current analysis; none of the specimens had to be excluded.
Continuous variables were described as means and standard deviations. All parameters were tested using the Shapiro-Wilk test for normality. Each osteotomy type at the specified LDTA (5° valgus, neutral, and 5° varus) was considered as a treatment. Differences between the treatments regarding lateral shift in center of force and changes of load on the medial side from the baseline to treated state were investigated with 1-way repeated-measures analysis of variance for both the ankle and subtalar joint. Similarly, comparison of load on medial side of treatments with baseline was analyzed. Significant factors were further investigated by pairwise comparison between each treatment at the baseline anatomic axis with Bonferroni-correction of P values. The Pearson/Spearman correlation coefficient (r) was used to measure the association between the treatment and changes in percentage of load on the medial side between ankle and subtalar joint. P < .05 was set for statistical significance. Data analysis was performed using GraphPad Prism (Release 2021, Prism 9 for Windows, Version 9.2.0; GraphPad Software LLC).
Results
Ankle Joint
Baseline: Neutral Anatomic Axis (LDTA Neutral, Normal Hindfoot Alignment)
SMOT to create protective valgus alignment (neutral to 5° valgus) unloaded the medial ankle joint by a mean of 6.4% ± 12% or 54.5 ± 72.3 N (not significant [ns]). SCO, on the other hand, led to a more pronounced unload of 10.3% ± 10% or 66.3 ± 51.2 N (P = .035) (Tables 1 and 2, Figure 2). Mean lateral shift of the center of force was 1.7 mm (range, -0.3 to 4.3 mm) after SMOT and 1.1 mm (range, -1.9 to 3.7 mm) after SCO (data not shown). There was no statistically significant difference between both techniques regarding their respective medial joint unloading effect when performed in a neutrally aligned ankle joint (Table 3).
Pressure Redistribution in the Ankle Joint a
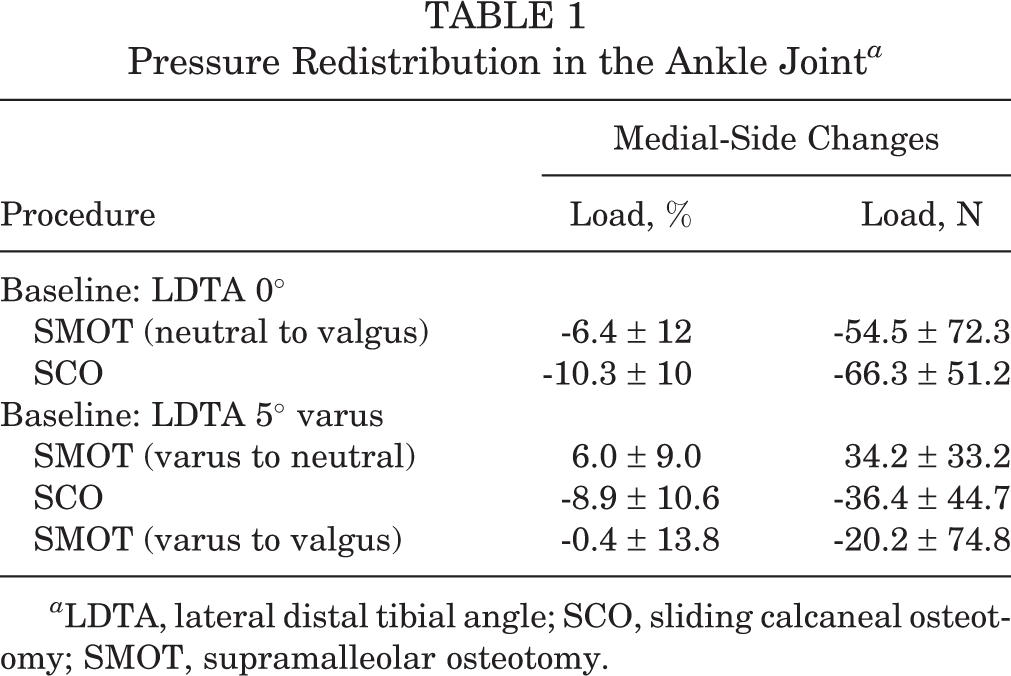
a LDTA, lateral distal tibial angle; SCO, sliding calcaneal osteotomy; SMOT, supramalleolar osteotomy.
Comparison of Load on Medial Side of Treatments to Baseline Conditions in the Ankle Joint With Parametric Statistical Test a

a ANOVA, analysis of variance; LDTA, lateral distal tibial angle; SCO, sliding calcaneal osteotomy; SMOT, supramalleolar osteotomy.
b Correction for 5 comparisons using Bonferroni multiple-comparisons test (P = .0268 with repeated-measures ANOVA). Boldface P value indicates statistically significant difference between comparisons (P < .05).
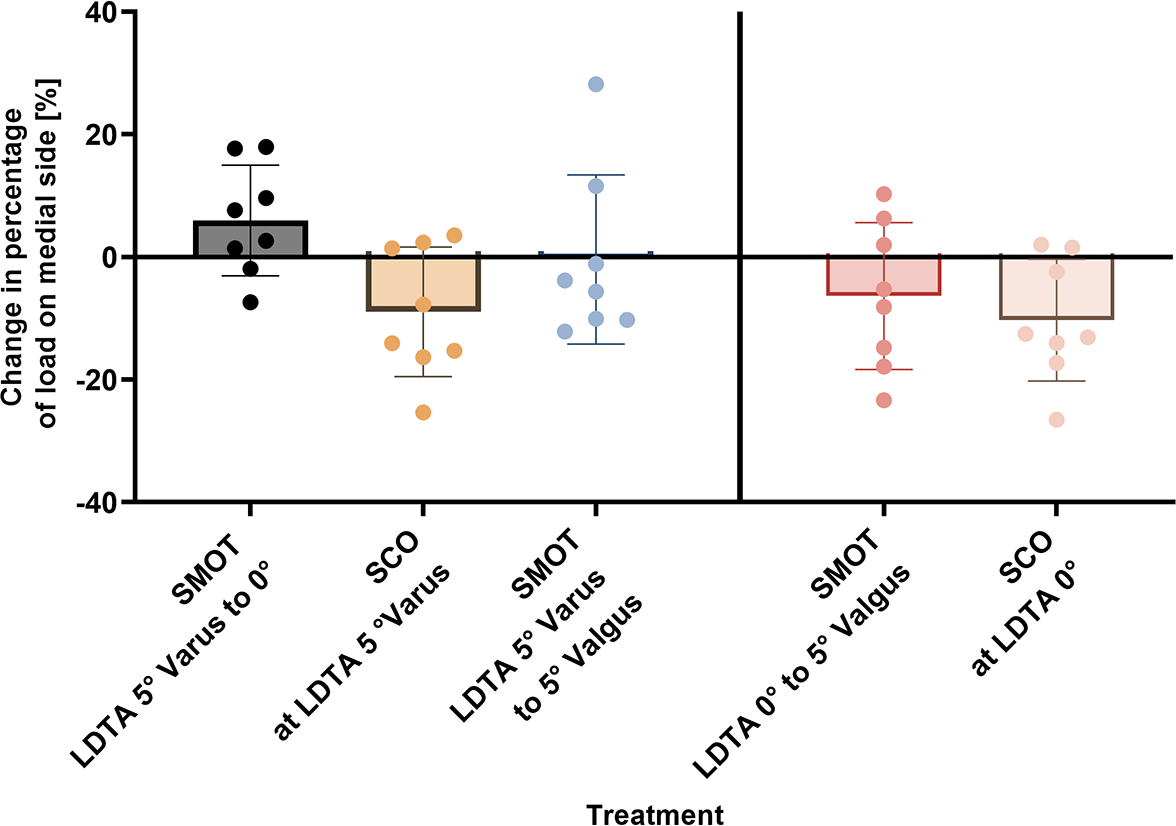
Pressure redistribution in the ankle joint. Bars indicate mean, and error bars show range. LDTA, lateral distal tibial angle; SCO, sliding calcaneal osteotomy; SMOT, supramalleolar osteotomy.
Comparison of Load on Medial Side Between Techniques in the Ankle Joint With Parametric Statistical Test a
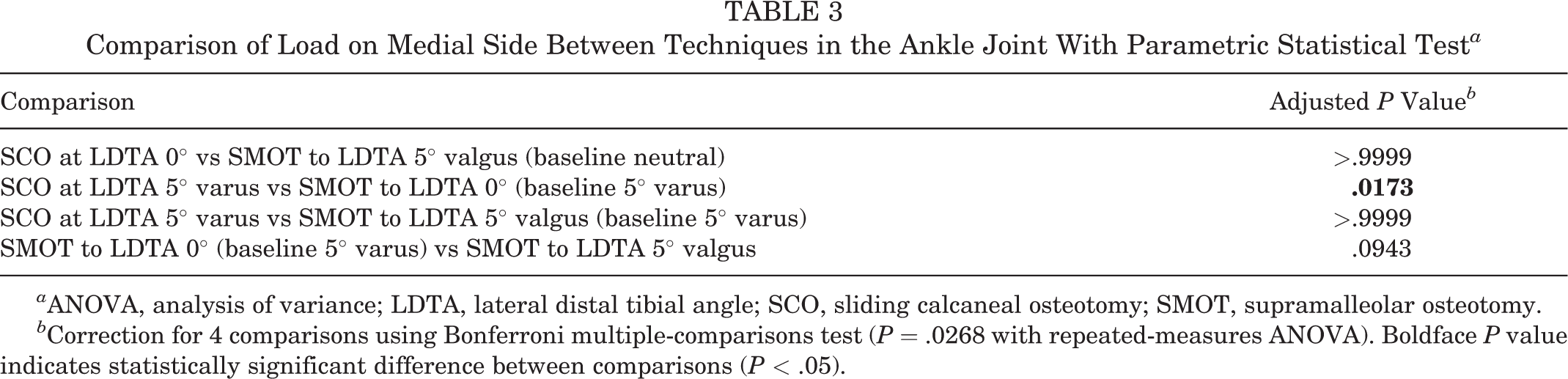
a ANOVA, analysis of variance; LDTA, lateral distal tibial angle; SCO, sliding calcaneal osteotomy; SMOT, supramalleolar osteotomy.
b Correction for 4 comparisons using Bonferroni multiple-comparisons test (P = .0268 with repeated-measures ANOVA). Boldface P value indicates statistically significant difference between comparisons (P < .05).
Baseline: 5° Varus Anatomic Axis (LDTA 5° Varus, Normal Hindfoot Alignment)
In case of a 5° varus alignment of the tibia, SMOT to correct LDTA to neutral insufficiently addressed pressure redistribution: load of the medial ankle joint even increased by 6% ± 9% or 34.2 ± 33.2 N (ns). SCO, on the other hand, unloaded the compartment by 8.9% ± 10.6% or 36.4 ± 44.7 N (ns) (Tables 1 and 2, Figure 2). Mean shift of the center of force was 1.9 mm (range, -0.6 to 4.1 mm) medial and 0.7 mm (range, -2.7 to 1.9 mm) lateral after SMOT and SCO, respectively (data not shown). When the LDTA was corrected from 5° varus to 5° valgus (total 10° with SMOT), the medial ankle joint was unloaded by 0.4% ± 13.8% or 20.2 ± 74.8 N (ns) (Table 1 and 2, Figure 2). When comparing all 3 techniques according to their unloading effect on the medial joint, SCO was superior to 5° SMOT (P = .0173) but not to 10° SMOT (ns) (Table 3). Examples of Tekscan outcomes are shown in Figures 3 and 4.
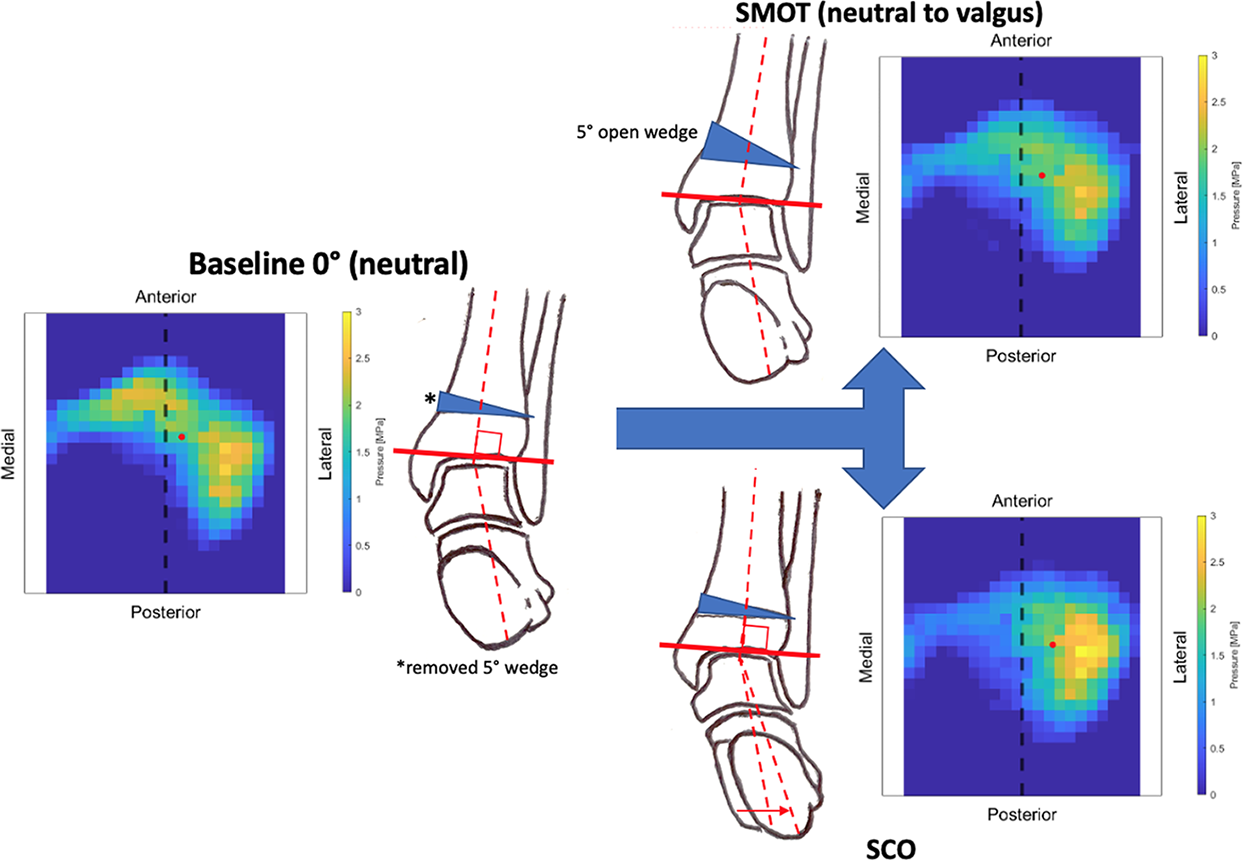
Schematic representation of the osteotomies performed starting from a neutral mechanical alignment. Pressure distribution is read from the Tekscan (specimen 6 is shown). The center of pressure is marked with a red dot. SCO, sliding calcaneal osteotomy; SMOT, supramalleolar osteotomy.
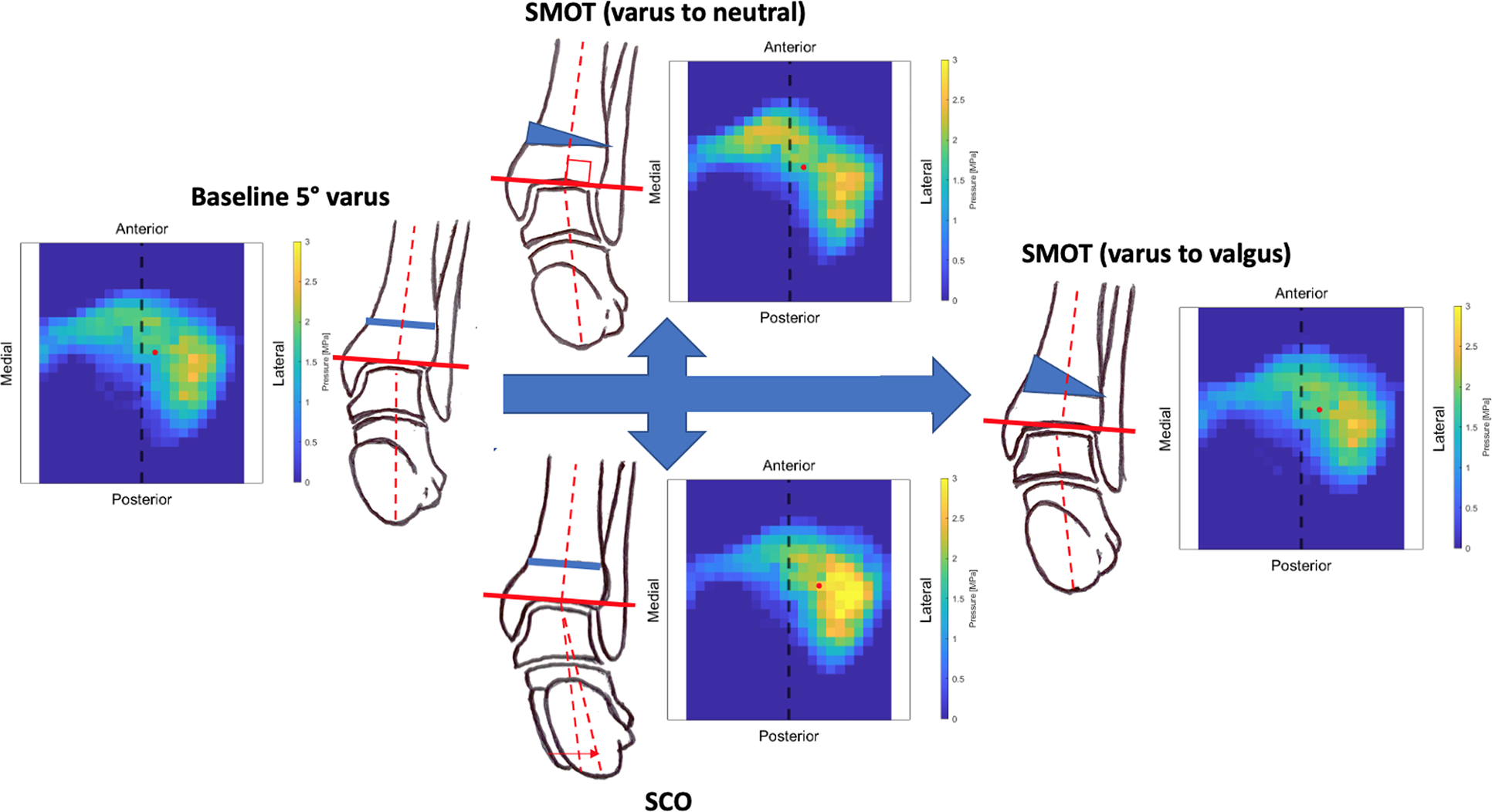
Schematic representation of the osteotomies performed starting from a 5° varus mechanical alignment. Pressure distribution is read from the Tekscan (specimen 6 is shown). The center of pressure is marked with a red dot. SCO, sliding calcaneal osteotomy; SMOT, supramalleolar osteotomy.
Subtalar Joint
SCO but not SMOT unloaded the medial compartment by 9.5% ± 10.1% (P < .01) and 6.7% ± 6.3% (P = .07) in case of neutral and 5° varus LDTA, respectively (Tables 4 and 5, Figure 5). In contrast, SMOT led to a medial pressure increase of 4.7% ± 9.1% (ns) and 1.4% ± 4.6% (ns), respectively. The larger the correction, the greater the pressure increase: 10° supramalleolar correction led to a 6.1% ± 10.6% load increase on the medial side (ns). Statistical comparisons between techniques are shown in Table 6.
Pressure Redistribution in the Subtalar Joint a
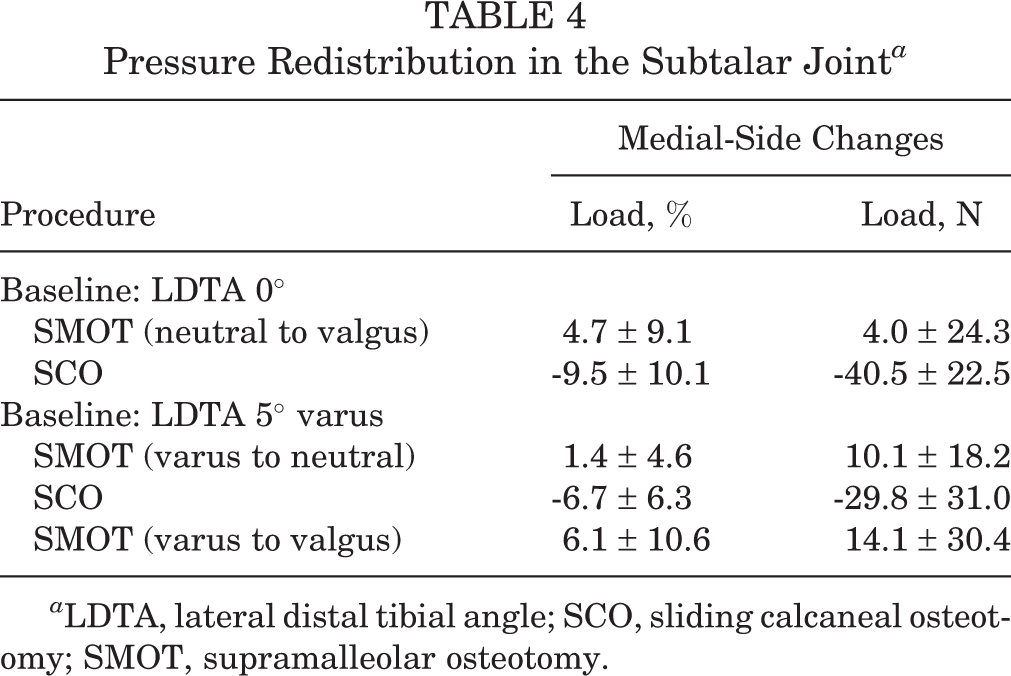
a LDTA, lateral distal tibial angle; SCO, sliding calcaneal osteotomy; SMOT, supramalleolar osteotomy.
Comparison of Load on Medial Side of Treatments With Baseline in the Subtalar Ankle Joint With Parametric Statistical Test a
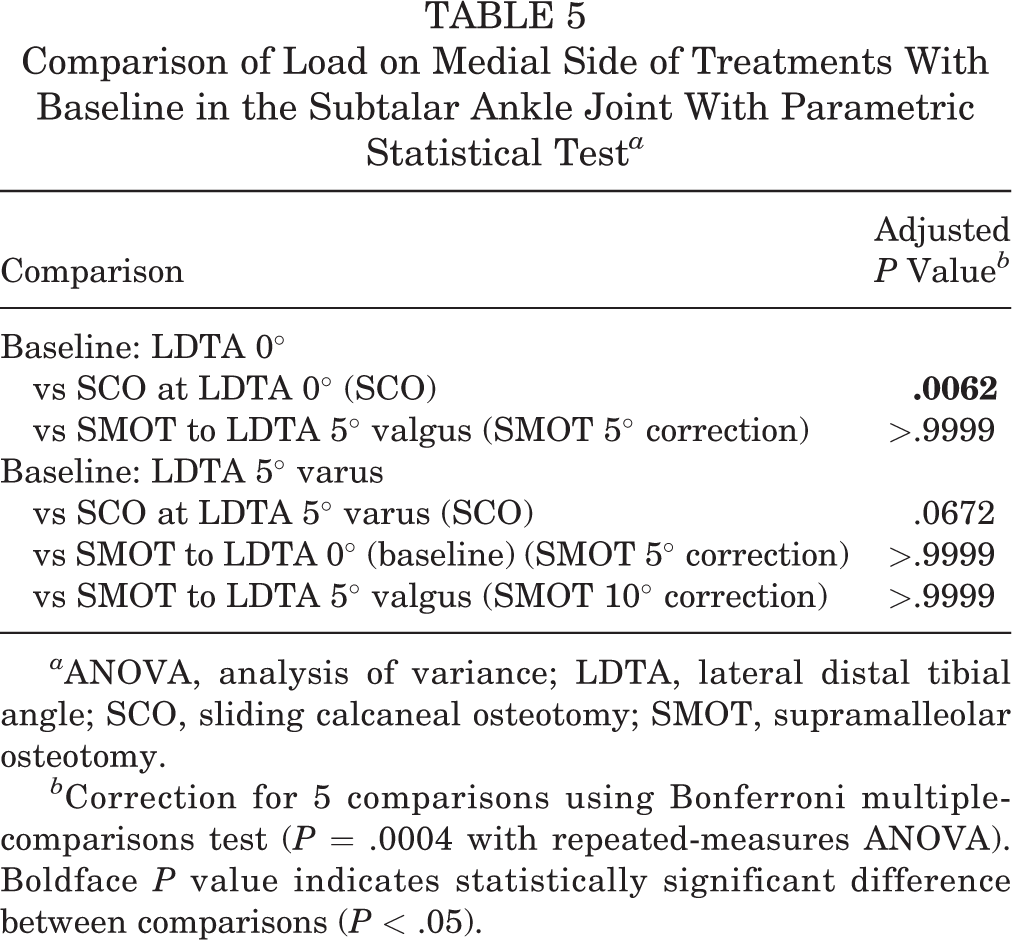
a ANOVA, analysis of variance; LDTA, lateral distal tibial angle; SCO, sliding calcaneal osteotomy; SMOT, supramalleolar osteotomy.
b Correction for 5 comparisons using Bonferroni multiple-comparisons test (P = .0004 with repeated-measures ANOVA). Boldface P value indicates statistically significant difference between comparisons (P < .05).
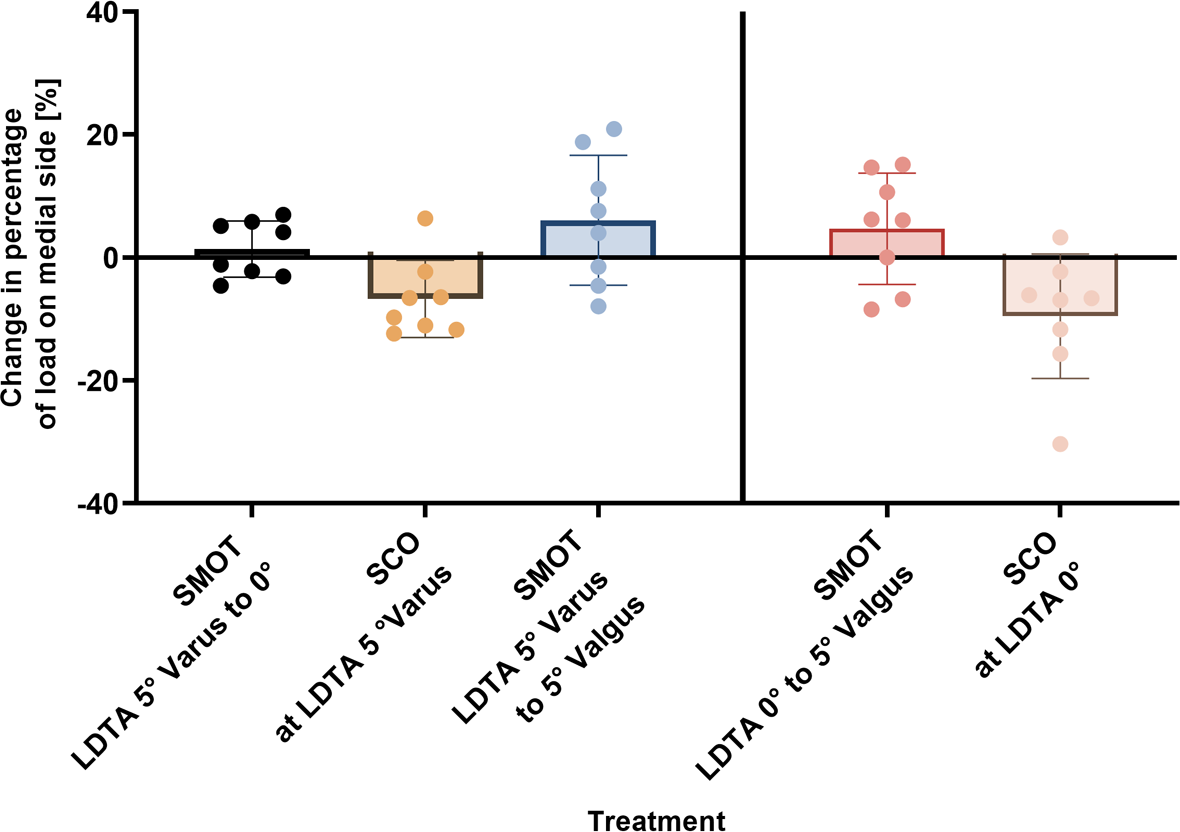
Pressure redistribution in the subtalar joint. Bars indicate mean, and error bars show range. LDTA, lateral distal tibial angle; SCO, sliding calcaneal osteotomy; SMOT, supramalleolar osteotomy.
Comparison of Load on Medial Side Between Techniques in the Subtalar Joint With Parametric Statistical Test a

a ANOVA, analysis of variance; LDTA, lateral distal tibial angle; SCO, sliding calcaneal osteotomy; SMOT, supramalleolar osteotomy.
b Correction for 4 comparisons using Bonferroni multiple-comparisons test (P = .0004 with repeated-measures ANOVA). Boldface P values indicate statistically significant difference between comparisons (P < .05).
There was no correlation between the unloading effect in the subtalar joint and ankle joint either with SMOT or SCO (Figure 6). However, there was a significant correlation between SCO at neutral LDTA and load distribution from medial to lateral (r = -0.58).

Pearson correlation values for association between osteotomy procedures and load changes in the subtalar joint and ankle joint. SCO, sliding calcaneal osteotomy; SMOT, supramalleolar osteotomy.
Discussion
The most important finding of this study is that reliable unloading of the medial talus can be achieved by SCO compared with SMOT, especially if a slight tibial varus is present.
Well-established indication for SMOT is asymmetric ankle osteoarthritis with varus or valgus deformity. Satisfactory mid- to long-term results have been reported. 15 –17 Inframalleolar correction, on the other hand, is performed if the main deformity lies below the ankle joint or if asymmetry remains after SMOT. 2,12 However, SCO is applied most to another entity: cavovarus deformities, where it shifts the force vector of the Achilles tendon and eliminates inversion. 25 Schmid et al 22 investigated ankle joint pressure changes in a pes cavovarus model and compared SMOT versus lateralizing SCO. In patients with fixed cavovarus feet, both SMOT and SCO provided equally good redistribution of ankle joint contact forces.
To date, it is however unclear whether similar results can be accomplished in normally aligned ankle joints. Usually, treatment of osteochondral lesions of the medial talus includes concomitant corrective osteotomies only if hindfoot malalignment is present. 29 No study, however, assessed whether (and to what extent) a simultaneous osteotomy might lead to local cartilage unloading despite absent osseous malalignment. This might be of interest, especially in case of revision OLT surgery.
In this experimental study, SCO unloaded the medial joint a mean of 10.3% (P = .04) and 8.9% (P = .6) in neutral or 5° varus tibial alignment, respectively. SMOT was beneficial only in case of neutral ankle alignment, where the medial side was unloaded by 6.4% on average (P = .12) (Tables 1 and 2). Comparing various surgical techniques, there was no statistically significant difference (Table 3), except for SCO versus 5° SMOT in case of a slight tibial varus alignment (P = .0173).
The amount of pressure relief needed to support cartilage healing is unknown. At the level of the knee, mechanical axis is usually overcorrected to 30% to 40% lateral to the midpoint (Fujisawa point), which was suggested to represent the best environment for cartilage defect healing. Decreasing the pressure transmitted through the affected compartment might therefore prove beneficial in cartilage revision surgery, also in the ankle joint. Further studies are however needed to prove its applicability as well as influence on clinical outcomes.
Guided by clinical interest, the most minimally invasive option was investigated. To leave the fibula intact, a medial distal tibial osteotomy was chosen by default. Knupp et al 14 suggested that an intact fibula leads to a paradox shift of the center of force due to a tension band effect of the collateral ligaments. This, however, was not the case if the neutral axis was changed into valgus, possibly owing to the fact that we investigated specimens without deformities. SMOT into varus and back, however, caused indeed an unexpected shift in the opposite direction. It must therefore be assumed that the fibula has indeed a protecting function to keep the talus in neutral position, thus counteracting the attempted load shift into varus. On a trial basis, however, the fibula was osteotomized in 2 patients without a significant effect. Another possible explanation might be that the calcaneus did not realign properly after SMOT compared with SCO, even though the heel was not fixed to allow translation.
Attention must be paid to the possible deleterious effects of overloading the lateral ankle with medial unloading osteotomies. One can assume that decentration may cause further instability to the syndesmotic band and medial collateral ligament complex. Furthermore, overloading of the tibiospring ligament and insufficiency of the tibialis posterior tendon should be avoided.
Regarding the subtalar joint, a decentration due to valgus overload might lead to subtalar osteoarthritis and unfavorable biomechanical changes to the forefoot.
Overall, the question remains unanswered whether these findings are true only in the biomechanical setup or also in real life. The fact is that SCO unloaded the medial compartment successfully regardless of the distal tibial joint angle (neutral or 5° varus) and should therefore be considered the surgical technique of choice.
Limitations
This study should be interpreted in light of its potential limitations. First, positions of sensors in the subtalar joint were not perfectly aligned with the ankle joint. Ligaments and capsule were preserved as well as possible, having influence on the joints’ access. Therefore, some sensors were at an angle, explaining the lack of correlation between the unloading effect in the subtalar joint and ankle joint. Second, ankle flexion was limited and fixed to 0° in this biomechanical setup to provide a standardized testing method while frontal angles were changed. However, different amounts of plantarflexion or dorsiflexion might have different loading patterns. Moreover, several values showed a clear trend that might have become significant with a larger sample size. Therefore, further research is needed to conclude clinical applicability and allow guidance of foot/ankle surgeons.
Conclusion
A lateral SCO can unload the medial compartment of the ankle joint successfully in case of neutral tibial axis. Change in the LDTA by SMOT did not significantly affect load distribution, especially in varus alignment. The subtalar joint was affected by both SCO and SMOT in opposite ways, which should be considered in the treatment algorithm.
Footnotes
Acknowledgment
The authors sincerely thank Mrs Nathalie Kuehne, the clinical study coordinator, for the tremendous support that she provided in the current work. Imaging was performed with support of the Swiss Center for Musculoskeletal Imaging, SCMI, Balgrist Campus AG, Zurich.
Final revision submitted January 11, 2023; accepted January 25, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: The study was funded by Balgrist University Hospital and Balgrist Campus and the Swiss Center for Musculoskeletal Imaging, SCMI, Balgrist Campus AG, Zürich, Switzerland. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the regional ethics committee of Zürich Canton (ref No. 2020-00653).