
Abstract
Background:
There are few sports-specific knee functional scales in the Arabic language. The Knee Outcome Survey–Sports Activities Scale (KOS-SAS) is a validated sports-specific patient-reported outcome measure that assesses knee function in an athletic population.
Purpose:
To provide a validated Arabic version of the KOS-SAS (KOS-SAS-Ar) while achieving cross-cultural adaptation for use in an Arabic-speaking population with sports-related knee disorders.
Study Design:
Cohort study (diagnosis); Level of evidence, 2.
Methods:
There were 2 independent translators who conducted a forward translation of the KOS-SAS, followed by a backward translation by different translators. Subsequently, researchers and expert invitees judged the conceptual content and cultural adaptations of the final translation. A total of 276 patients completed the KOS-SAS-Ar as well as the International Knee Documentation Committee (IKDC) subjective assessment of knee function and a visual analog scale (VAS) for pain. Statistical analysis was performed for test-retest reliability, convergent validity, construct validity, and factor analysis.
Results:
The test-retest reliability of the KOS-SAS-Ar was high (r = 0.9). The items of the KOS-SAS-Ar had statistically significant internal consistency, with a Cronbach alpha of .924 (P < .0001). The KOS-SAS-Ar Symptoms subscore correlated with the VAS pain score (P < .0001), and the KOS-SAS-Ar Functional Limitations subscore correlated with the IKDC subjective score (P < .0001). The construct validity of the KOS-SAS-Ar was satisfactory (Kaiser-Meyer-Olkin value = 0.868; Bartlett test: P < .0001). Factor analysis showed a statistical correlation among the 11 items of the KOS-SAS-Ar.
Conclusion:
The KOS-SAS-Ar demonstrated favorable reliability and validity, and it appears to be a suitable tool for Arabic-speaking patients with sports-related knee conditions.
Physical fitness is crucial for a healthy life. 6 Nowadays, more people tend to practice sports frequently. 8 The knee joint is highly susceptible to sports-related injuries, more so than other joints. 11,20 Knee disorders can affect overall performance in sports. 18,19 Clinically, a valid assessment scale that directly measures how patients perceive their own knee function may be useful in tracing progression rather than relying on physiological or laboratory examinations. 5 Various validated patient-reported outcome measures (PROMs) of knee function are available 4,17 ; however, general knee function scoring systems may not adequately address sports knee disorders. 8
The Knee Outcome Survey 13 (KOS) consists of 2 distinct sections: the Activities of Daily Living Scale (KOS-ADLS), which mainly measures regular knee functional levels in daily routines, and the Sports Activities Scale (KOS-SAS), which evaluates higher knee function in sports in the physically active population. 4 Both scales have been proven to be valid and reliable. 4 The KOS-ADLS has been translated and validated into numerous languages, including German, 3 Portuguese, 9 Turkish, 7 Greek, 14 French, 21 and Arabic. 1 Thus far, the KOS-SAS has been only translated into Portuguese. 8
As it is desirable that PROMs are available in the mother tongue of the patients for optimal results, we aimed to provide a validated Arabic version of the KOS-SAS (KOS-SAS-Ar) and achieve cross-cultural adaptation. The KOS-SAS-Ar is expected to offer an athletic knee assessment tool for the Arabic-speaking population across 22 countries globally but mainly in the Middle East and North Africa.
Methods
This study was conducted between June 2019 and January 2020. The study protocol was approved by our institutional review board, and all included patients provided written informed consent.
KOS-SAS Instrument
The KOS-SAS comprises 11 items that are subcategorized into 2 sections: the Symptoms subscale (7 items) and the Functional Limitations with Sports Activities (Functional Limitations) subscale (4 items) (Appendix Figure A1). The first 7 items evaluate knee symptoms in terms of severity, calibrated over 6 levels: “never have” (5 points), “have but does not affect sports activity” (4 points), “affects sports activity slightly” (3 points), “affects sports activity moderately” (2 points), “affects sports activity severely” (1 point), and “prevents me from all sports activity” (0 points). Items 8 to 11 assess the ability to perform specific knee athletic movements on a similar 6-level scale: “not difficult at all” (5 points), “minimally difficult” (4 points), “somewhat difficult” (3 points), “fairly difficult” (2 points), “very difficult” (1 point), and “unable to do” (0 points). 4 The final score is calculated by dividing the raw total score by 55 and multiplying the quotient by 100. The highest score (100) indicates normal knee function, while the lowest score (0) indicates the loss of knee function.
The KOS-SAS has 9 additional items that are not included in numerical scoring. These add-on items represent a complementary subjective assessment section for rating knee function during sports and the level and frequency of sports activities at different stages: before the injury, before treatment, and at the time of the survey response.
Translation and Cross-cultural Adaptation
We obtained written permission to translate the original English KOS-SAS from the primary author. 13 Conceptual rather than literal translations were implemented throughout the translation process. The KOS-SAS-Ar was developed in Modern Standard Arabic (MSA). The translation process was performed in accordance with the guidelines for cross-cultural adaptation of self-reported measures. 2 First, 2 bilingual clinicians independently translated the original English version into Arabic. The translated version was then blindly converted back to English by 2 qualified translators from the College of Languages and Translation, King Saud University. Finally, we evaluated the quality of the final translation by comparing each Arabic-translated KOS-SAS item with its original English counterpart. The finalized KOS-SAS-Ar is available in Appendix Figure A2.
Patients and Study Design
The questionnaire was distributed to 276 patients with knee disorders. The participants were verbally invited and recruited from an orthopaedic clinic. The sampling method used was simple random sampling. After the exclusion of patients who did not fit inclusion criteria, participants were selected from a scheduled patient list of the outpatient orthopaedic sports clinic based on random numbers. The inclusion criteria were native Arabic speakers, patients with a history of sports injuries, and adults aged ≥18 years. The exclusion criteria were non-Arabic speakers, patients with degenerative abnormalities, patients with multiple joint injuries, and children.
The demographic data of the participants were collected, including their sex, age, height, weight, level of education, and duration of the knee condition. In addition to the KOS-SAS-Ar, the participants completed a visual analog scale (VAS) for pain 15 and the International Knee Documentation Committee (IKDC) subjective assessment of knee function. 10,12 Help was available for the patients who required assistance in completing the questionnaire.
Validation and Reliability
Test-retest reliability refers to the degree of consistency of the test results over time. A reliable test should provide consistent measurements each time that the test is performed. In our study, we ensured test-retest reliability by administering the KOS-SAS-Ar to 20 patients from the study sample twice within a week. All participants of the retest stated that their knee conditions remained the same since the primary test. The standard error of measurement (SEM) indicates how far the measurements of a certain test are, relative to the true measurement. As the SEM increases, the test reliability decreases and vice versa. The smallest detectable change (SDC) refers to the minimum amount of change that is required to result in a real difference in the outcomes. Any change less than the SDC value can be attributed to a random error.
Internal consistency reflects the degree of homogeneity among items of an instrument that share a common target measurement. We measured internal consistency using the Cronbach alpha. The Cronbach alpha is an index of internal consistency used to measure how 2 groups of items are related as a unit. The Cronbach alpha is expressed on a scale from 0 to 1, with higher values representing higher degrees of internal consistency.
Convergent validity describes how close 2 constructs are in terms of measuring relatively similar entities. For this purpose, we examined the participants’ scores on the VAS and KOS-SAS-Ar Symptoms subscale for convergent validity in reference to symptoms. Similarly, the participants’ scores on the IKDC subjective form and KOS-SAS-Ar Functional Limitations subscale were tested for convergent validity concerning function. Construct validity shows the extent to which a construct is valid for testing the target concept. The construct validity of the KOS-SAS-Ar was tested using confirmatory factor analysis.
Statistical Analysis
The data were analyzed using SPSS (Version 24.0; IBM). Descriptive statistics (mean, standard deviation, frequency, and percentage) were used to define quantitative and categorical variables. The SEM was calculated from the standard deviation of a set of scores and the reliability coefficient using the formula SEM = S√1-r, where S is the standard deviation and r is the reliability coefficient of the measurement. The SDC was calculated based on the SEM and a given degree of confidence, for instance, 95% (SDC = SEM × 1.96√2). The intraclass correlation for internal consistency of the KOS-SAS-Ar was evaluated using the Cronbach alpha in which values were interpreted as excellent (≥0.9), good (<0.9 to ≥0.8), acceptable (<0.8 to ≥0.7), questionable (<0.7 to ≥0.6), poor (<0.6 to ≥0.5), or unacceptable (<0.5). Convergent validity was assessed using Pearson correlation analysis between the KOS-SAS-Ar Symptoms subscale items and VAS scores as well as between the KOS-SAS-Ar Functional Limitations subscale items and IKDC subjective scores.
Simple regression analysis was used to observe the linear relationship between the KOS-SAS-Ar subscores for symptoms and sports activities. The construct validity of the KOS-SAS-Ar was determined by performing confirmatory factor analysis. A correlation matrix, the Kaiser-Meyer-Olkin (KMO) test of sampling adequacy, and the Bartlett test of sphericity were used to obtain 11-item factorability. In factor analysis, the principal component method was used, and the proportion of variance was estimated through initial eigenvalues expressed by each of the factors. Varimax rotation was used to obtain rotated factors. A P value ≤.05 was used to indicate statistical significance.
Results
Among the 276 participants who completed the KOS-SAS-Ar, 164 (59.4%) were male and 112 (40.6%) were female. The mean age of these participants was 28.03 ± 8.70 years. The mean height and weight of the participants were 169.76 ± 5.46 cm and 80.62 ± 9.74 kg, respectively. Additionally, 68% of the participants were college graduates, and the remaining participants held either postgraduate degrees (7%) or undergraduate-level degrees (25%). The mean duration of the knee condition among the patients was 6.53 ± 3.44 months. Various knee disorders were observed among the participants, including knee sprain (n = 176 [63.8%]), anterior cruciate ligament injury (n = 59 [21.4%]), patellofemoral maltracking (n = 14 [5.1%]), meniscal injury (n = 12 [4.3%]), medial collateral ligament injury (n = 8 [2.9%]), lateral collateral ligament injury (n = 5 [1.8%]), and multiligamentous injury (n = 2 [0.7%]). The mean VAS pain score was 6.76 ± 2.60, and the mean IKDC subjective score was 87.30.
As demonstrated in Table 1, the patients’ responses to the KOS-SAS-Ar subjective assessment section items regarding sports-related activities revealed that they estimated the current function of their knees as 66.8% ± 27.0%. The overall level of knee function in sports was judged to be “nearly normal” by 40.6% (n = 112) of the participants, and 41.3% (n = 114) of the participants chose “nearly normal” to describe their current level of knee function in sports. Regarding the highest level of sports activity, 68.5% (n = 189) showed an ability to participate in strenuous sports before the injury. That rate decreased before receiving treatment to 28.3% (n = 78). At the time of the questionnaire, 38.4% (n = 106) of the participants stated an ability to partake in strenuous sports. Regarding the frequency of sports participation before the injury, 39.1% (n = 108) of the patients reported a mean of 1 to 3 times weekly. The sports frequency dropped before treatment to less than once per month among 37.7% (n = 104) of the participants. The mean frequency of sports participation during the survey was 1 to 3 times monthly, as stated by 32.6% (n = 90) of the respondents.
Participants’ Responses on KOS-SAS-Ar Subjective Assessment Section a

a Data are reported as mean ± SD or n (%). KOS-SAS-Ar, Arabic version of the Knee Outcome Survey–Sports Activities Scale.
b Examples: football, soccer, basketball.
c Examples: tennis, skiing.
d Examples: cycling, swimming, golf.
e 0% = unable to perform sports activities, 100% = preinjury level.
The final KOS-SAS-Ar showed a high level of test-retest reliability (Pearson r = 0.9). The data showed a normal distribution. As shown in Table 2, high internal consistency was demonstrated for the items of the KOS-SAS-Ar Symptoms subscale (Cronbach α = .869; P < .0001) and the KOS-SAS-Ar Functional Limitations subscale (Cronbach α = .943; P < .0001). Furthermore, the overall internal consistency of the KOS-SAS-Ar was high (Cronbach α = .924; P < .0001). The SEM and SDC of the KOS-SAS-Ar were 3.369 and 9.338, respectively.
Internal Consistency of All Items and Subscales of KOS-SAS-Ar a

a Dashes indicate not applicable. KOS-SAS-Ar, Arabic version of the Knee Outcome Survey–Sports Activities Scale.
Regression analysis indicated a moderate linear relationship between the scores on the KOS-SAS-Ar Symptoms subscale and VAS pain scores (R 2 = 0.341; P < .0001) (Table 3). A change of 48.85% in the VAS score was elucidated using the KOS-SAS-Ar Symptoms subscore. Moreover, a moderate linear relationship was demonstrated between the scores on the KOS-SAS-Ar Functional Limitations subscale and IKDC subjective scores (R 2 = 0.489; P < .0001) (Table 4).
Relationship of KOS-SAS-Ar Symptoms Subscore With VAS Pain Score a

a KOS-SAS-Ar, Arabic version of the Knee Outcome Survey–Sports Activities Scale; VAS, visual analog scale.
Relationship of KOS-SAS-Ar Functional Limitations Subscore With IKDC Subjective Score a
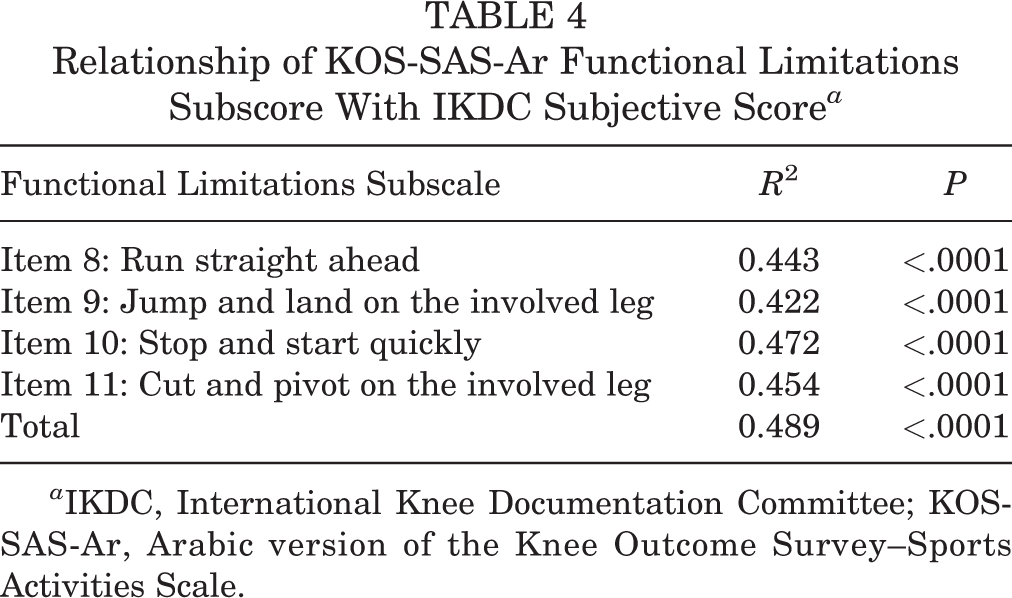
a IKDC, International Knee Documentation Committee; KOS-SAS-Ar, Arabic version of the Knee Outcome Survey–Sports Activities Scale.
Construct validity was verified using factor analysis. The correlation among the 11 items of the KOS-SAS-Ar displayed statistical significance. There was no multicollinearity, as the determinant of the correlation matrix was 0.0001. The KMO value was 0.868, greater than the accepted level of >0.5, allowing us to proceed with factor analysis. The result of the Bartlett test of sphericity was also significant (P < .0001), indicating that the correlation matrix was not an identity matrix. Analysis of communalities showed that the variance among variables was accounted for by the extracted factors (Table 5).
Communalities of 11 Items and Rotated Component Matrix of KOS-SAS-Ar a
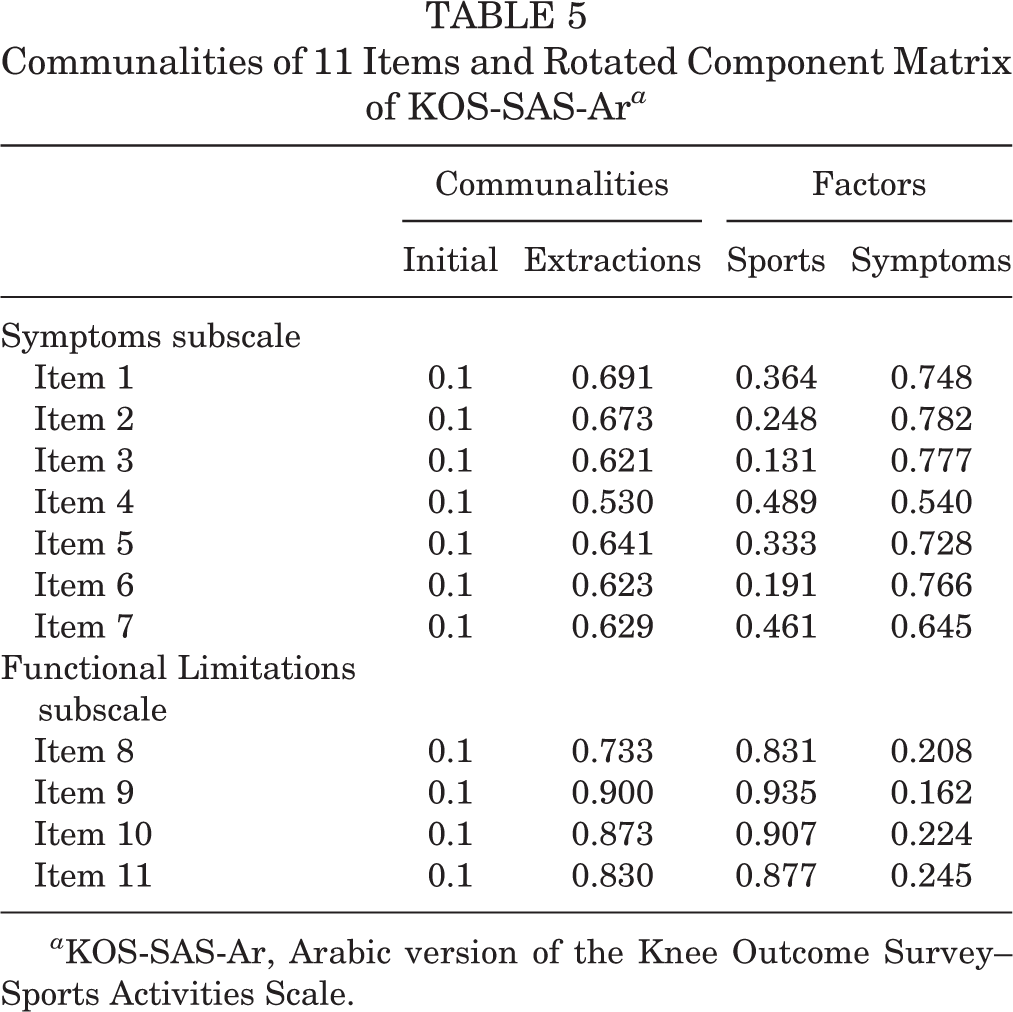
a KOS-SAS-Ar, Arabic version of the Knee Outcome Survey–Sports Activities Scale.
There were 2 factors identified: sports and symptoms. Analysis of the 2-factor extraction along with their eigenvalues, percentage of variance attributable to each factor, and cumulative variance of the factors showed that sports accounted for 56.94% of the variance, while symptoms accounted for 13.46% of the variance, with a cumulative variance of 70.40%. From the scree plot, the curve began to flatten after factor number 2; thus, only 2 factors were retained (Figure 1). Table 5 also illustrates the loading of the 11 items on the 2 factors extracted. The higher the absolute value of the loading, the greater the factor contributing to the variable. The loading indicated that 2 factors independently contributed to each of the items without any overlap.

Screen plot of eigenvalues toward the extraction of the number of factors.
Discussion
The KOS-SAS-Ar showed favorable results in terms of internal consistency (Cronbach α = .924) and construct validity (KMO value = 0.868; Bartlett test: P < .0001). As Arabic is a widely spoken language among more than 400 million people, 22 the KOS-SAS-Ar will be useful for Arabic-speaking athletes with knee complaints. Furthermore, utilizing the MSA style for the Arabic KOS-SAS renders it to be readily understood and answered appropriately by patients. Currently, MSA is the dominant form of spoken and written Arabic in classrooms, media, and publications. 16
To the best of our knowledge, apart from the Portuguese version, 8 no other non-English version of the KOS-SAS exists. In the current study, the KOS-SAS-Ar was completed by 276 patients with multiple sports-related knee abnormalities, and excellent test-retest reliability (r = 0.9) was demonstrated over a 1-week interval. Similarly, the Portuguese KOS-SAS showed high intraobserver reliability (correlation coefficient = 0.9778; P < .001). 8 The low SEM of the KOS-SAS-Ar (3.369) reflects its high reliability, and the SDC of 9.338 indicates that, for a given patient, any change in the KOS-SAS-Ar score >9.338 can be considered a true change rather than resulting from a random variation. Regarding the KOS-SAS, the SEM and SDC have not been determined yet in the previous literature. For the sake of comparison, the KOS-ADLS can be taken as a reasonably similar knee functional scale. The present study findings were comparable with the published SEM and SDC values for the English, 13 German, 3 and Turkish 7 versions of the KOS-ADLS. Moreover, the items of the KOS-SAS-Ar appeared to be coherently related, with a high degree of internal consistency (Cronbach α = .924).
The validity of each KOS-SAS-Ar item was assessed by quantifying the correlation between relatively related items obtained from similar measures. A significant correlation was observed between the KOS-SAS-Ar Symptoms subscore and the VAS pain score. A similar correlation was observed between the Portuguese version of the KOS-SAS and the VAS. 8 It was not possible to further test the convergent validity of the KOS-SAS-Ar Symptoms subscale with any other instrument besides the VAS because of a lack of Arabic-validated knee symptom scales at the time of this study. A statistically significant correlation was also found between the KOS-SAS-Ar Functional Limitations subscore and the IKDC subjective score. Likewise, the Portuguese KOS-SAS correlated well with the functional capacity section of the 36-item Short Form Health Survey. 8
Both KOS-SAS-Ar subscales appeared to be linearly related in regression analysis. Similarly, regression analysis demonstrated a significant linear relationship between the IKDC subjective score and the VAS pain score. The construct validity of the KOS-SAS-Ar was favorable. Factor analysis showed a statistical correlation among the 11 items of the KOS-SAS-Ar.
Limitations
The main limitation of this study was the relative lack of validated sports-focused knee functional scoring systems in the Arabic language. There is a remarkable scarcity of validated Arabic PROMs, indicating an existing gap in the literature. The availability of corresponding Arabic knee function scales for athletes can provide more rational comparisons. However, certain elements of the KOS-SAS-Ar have been matched with corresponding elements from similar scales for the sake of correlation and validation processes. It could be a limitation that convergent validity for the symptoms-related items of the KOS-SAS-Ar was tested using the VAS only. A further potential limitation of this study was the difficulty of including many participants from various geographic locations where certain Arabic dialects are predominantly spoken. However, the widespread use of MSA makes it the best available medium for communication among Arabic speakers.
Conclusion
The KOS-SAS-Ar demonstrated favorable reliability and validity, and it appears to be a suitable tool for Arabic-speaking patients with sports-related knee conditions.
Footnotes
Final revision submitted February 18, 2023; accepted March 2, 2023.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from King Saud University (No. 13/3811/IRB).