
Abstract
Background:
Knee arthroscopy is frequently performed to improve joint function and relieve pain. However, there is no consensus regarding the effect of prior arthroscopy on outcomes following medial opening-wedge high tibial osteotomy (MOWHTO).
Purpose:
To compare midterm clinical outcomes and survival rates after MOWHTO between patients with and without a history of knee arthroscopy.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
We enrolled patients who underwent MOWHTO between March 2008 and February 2017 and had ≥4 years of follow-up. Patients who had undergone knee arthroscopy were included in an arthroscopy group, and those who had not were included as controls. After propensity score matching based on age, sex, body mass index, and lesion size, 80 patients in each group were included. Clinical outcomes were assessed using the Knee injury and Osteoarthritis Outcome Score (KOOS), 36-Item Short Form Health Survey, and Tegner Activity Scale. Furthermore, survival rates and relevant risk factors that affected joint survivorship were analyzed, wherein conversion to total knee arthroplasty was considered the endpoint.
Results:
Although the pre- to postoperative improvement in clinical outcomes did not differ significantly between the groups, there were significant between-group differences in final postoperative scores on the KOOS–Activities of Daily Living (arthroscopy vs control, 78.1 ± 10.6 vs 81.0 ± 9.8; P = .031), KOOS–Sport and Recreation (45.4 ± 12.8 vs 48.7 ± 13.5; P = .045), 36-Item Short Form Health Survey Physical Component Summary (65.1 ± 12.7 vs 69.3 ± 11.8; P = .017), and Tegner Activity Scale (4.1 ± 1.1 vs 4.5 ± 1.0; P = .007). The survival rate was 96.8% at a mean follow-up of 8 years, and survival was not associated with a history of arthroscopy (P = .697; log-rank test).
Conclusion:
Although patients with prior arthroscopy had some inferior patient-reported outcome scores after MOWHTO, the overall clinical improvements were similar in the arthroscopy and control groups.
Keywords
High tibial osteotomy (HTO) is a reliable treatment option for young patients with medial compartment osteoarthritis of the knee with varus alignment. 32 Although the benefits of HTO have been demonstrated in multiple clinical studies, 10,38,46 several factors that lead to poor postoperative outcomes or survival have been identified. 18,19,38
Arthroscopy is safe and effective for the treatment of mechanical symptoms in the early stages of knee osteoarthritis. 26,28,33 Though the use of arthroscopy for the treatment of various knee conditions has grown rapidly over the past decade, little is known about the clinical impact of prior arthroscopy on HTO outcomes. 26,28 Knee arthroscopy is no longer recommended for the treatment of osteoarthritis. 21 Knee procedures cause changes in the knee joint and surrounding tissue; this may make subsequent procedures more challenging and even lead to inferior results, possibly attributed to the previous arthrotomy, scar tissue, potential disruption in the joint’s structures, and potential for bacterial seeding. 15,20,27,31,34 A systematic review by Winter et al 44 demonstrated that patients who underwent arthroscopic surgery for knee osteoarthritis showed a 2.6% annual rate of progression to total knee arthroplasty (TKA).
Several clinical studies have sought to investigate the influence of prior arthroscopic knee surgery on the outcomes of knee arthroplasties, with some reporting equivalent outcomes 17,41 and others a deleterious influence. 2,35,42 Since HTO is used to treat knee osteoarthritis in younger patients who are not candidates for TKA, a better understanding of whether prior arthroscopy is associated with the outcome of a subsequent HTO is necessary to better assess the candidacy of a patient for arthroscopy.
The primary aim of this study was to assess the influence of knee arthroscopy on HTO outcomes. We compared the midterm clinical outcomes and survival rates after medial opening-wedge HTO (MOWHTO) between patients with and without a history of knee arthroscopy. We also evaluated the association of knee arthroscopy with postoperative outcomes based on the time interval between prior arthroscopy and MOWHTO. Our hypothesis was that prior knee arthroscopy will have a significant association with worse postoperative outcomes after MOWHTO.
Methods
Patients
This study was approved by the institutional review board of our institution, and all patients provided informed consent. This study was a retrospective comparative study wherein the baseline prognostic factors were equalized using propensity score matching (PSM). We retrospectively identified all patients who underwent MOWHTO at our institution for the treatment of knee osteoarthritis between March 2008 and February 2017. Patients were included if they underwent MOWHTO for isolated medial compartment osteoarthritis (Kellgren-Lawrence grade ≥2) and varus malalignment with intact cruciate ligament.
The exclusion criteria were (1) prior open knee procedures, (2) associated ligamentous insufficiency (anterior or posterior cruciate ligament) that required reconstruction, (3) knee range of motion <120° or flexion contracture >15°, (4) patellofemoral or lateral compartment osteoarthritis (Kellgren-Lawrence grade ≥2), (5) medial proximal tibial angle >90°, (6) inflammatory arthritis or traumatic osteoarthritis, (7) additional cartilage regenerative procedures, and (8) follow-up <4 years.
A total of 423 patients (423 knees) were identified, and 90 patients were selected according to a history of arthroscopic procedure (arthroscopy group). Arthroscopic procedures included any arthroscopic debridement, meniscectomy, meniscal repair, or chondroplasty. Each patient in the arthroscopy group was matched to a patient who did not undergo any prior arthroscopic procedures (control group) using PSM. One-to-one PSM was based on the following baseline covariates to identify comparable patients who underwent MOWHTO: age, sex, body mass index, operation side, preoperative hip-knee-ankle axis (HKA) angle, and preoperative grade of osteoarthritis. The balance of covariate distribution between groups was evaluated by calculating standardized mean differences. After PSM the study cohort consisted of 160 patients (80 each in the arthroscopy and control groups), with covariate distribution balanced between the groups (all standardized mean differences <0.2) (Figure 1).
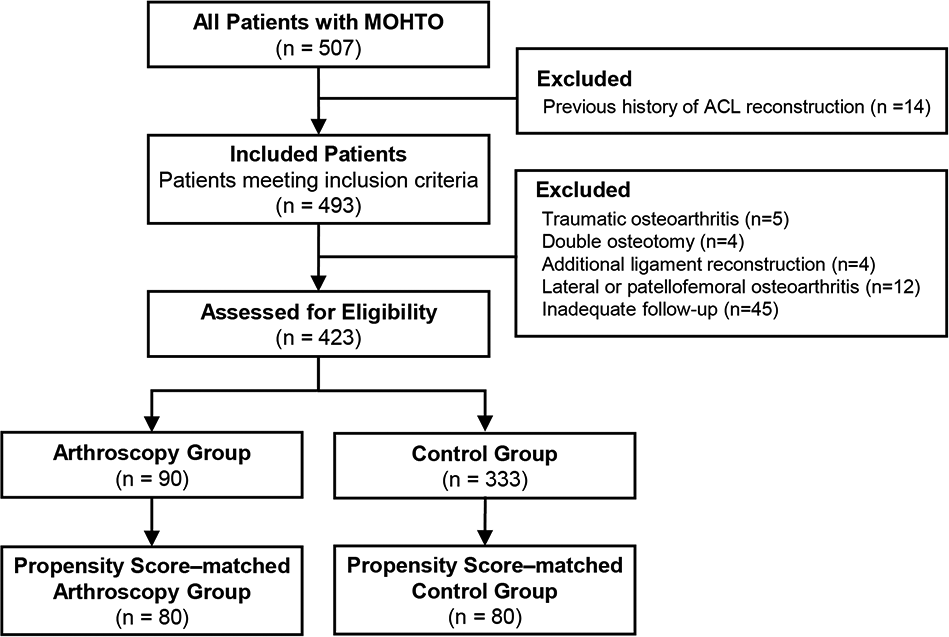
Patient enrollment process in the study. ACL, anterior cruciate ligament; MOWHTO, medial opening-wedge high tibial osteotomy.
Surgical Techniques and Postoperative Management
The correction angle was calculated during preoperative planning in accordance with the method proposed by Dugdale et al. 9 The goal was to shift the weightbearing line to the Fujisawa point and create 3° to 5° of postoperative mechanical valgus. 11
All surgical procedures were performed by 2 experienced orthopaedic surgeons (E.K.S., J.K.S.). Arthroscopic examination was performed in all patients to evaluate the cartilage of the medial and lateral compartments and the patellofemoral joint at the time of MOWHTO. Detected meniscal tears or articular cartilage injuries were treated with debridement or microfracture, based on the surgeon’s judgment. Among the 160 patients, 18 (11.3%) underwent concurrent procedures to manage associated injuries, and there were no significant intergroup differences in the proportion of the various procedures performed.
After arthroscopy, MOWHTO was performed in a biplanar fashion according to the technique developed by Lobenhoffer and Agneskirchner 24 and using Aescula plates (Medyssey). Allograft cancellous bone chips were impacted into the osteotomy gap to promote bony union if the tibial opening exceeded 10 mm.
Postoperative rehabilitation included active and passive range of motion exercises from the first postoperative day. Patients were permitted to perform partial weightbearing ambulation for the first 6 weeks after surgery while wearing a hinged knee brace; subsequently, progressive weightbearing was encouraged.
Clinical Evaluation
Clinical examinations were documented at 1, 3, 6, and 12 months after surgery and annually thereafter. The primary clinical outcome measure was the Knee injury and Osteoarthritis Outcome Score (KOOS). 36 Secondary clinical outcome measures included the 36-Item Short Form Health Survey (SF-36) questionnaire 45 and the Tegner Activity Scale. 40 Improvement was defined as an improvement in postoperative scores. All clinical outcomes were assessed by 2 independent investigators (J.H.C., C.H.L.) blinded to the surgical procedures and radiographic analyses. Moreover, survivorship was analyzed using the Kaplan-Meier method, and the endpoint of survival was conversion to TKA.
Radiological Evaluation
For radiological evaluation, standardized anteroposterior, lateral, and Merchant views of the knee and full-length lower extremity weightbearing radiographs were obtained preoperatively and at each follow-up. The radiological evaluation included mechanical HKA angle, posterior tibial slope, medial proximal tibial angle, and Kellgren-Lawrence grading for preoperative planning. Radiographic results were measured by 2 independent investigators (J.H.C., C.H.L.) blinded to the study aim.
Arthroscopic Evaluation
Grading of the articular cartilage status was established for the medial femoral condyle using the International Cartilage Regeneration & Joint Preservation Society system at the time of primary MOWHTO. 5 In this system, superficial lesions, superficial fissures, and cracks are considered grade 1 cartilage defects; lesions extending to <50% of the cartilage depth are considered grade 2 defects; and lesions extending to >50% of the cartilage depth are considered grade 3 if they do not involve the subchondral bone and grade 4 if they do involve the subchondral bone. Grading was based on consensus between the senior surgeons (E.K.S., J.K.S.) and a trained orthopaedic fellow (C.H.L.) during surgery.
Statistical Analysis
For normally distributed variables, paired and independent t tests were performed for analysis. For nonnormally distributed variables, Kruskal-Wallis and Wilcoxon signed-rank tests were used to analyze differences. A 1-way analysis of variance was used to compare differences in continuous variables, and the chi-square test or Fisher exact test was used to compare differences in categorical variables. The Mann-Whitney U test with Bonferroni correction was used for post hoc comparisons.
Survival rates were evaluated using Kaplan-Meier analysis with 95% CIs. A log-rank test was carried out on the survival curves, which demonstrated significant intergroup differences in the survival rates based on the presence of a history of knee arthroscopy. The threshold for significance was P < .05.
A post hoc power analysis indicated that number of patients allocated to the good status group (n = 80) and poor status group (n = 80) was adequate to achieve >80% power for the primary outcome (power = 0.94).
Results
Among the 423 eligible patients before PSM analysis, 90 (21.3%) had a history of knee arthroscopy before MOWHTO. On average (mean ± SD), these patients had arthroscopy 29.2 ± 24.3 months before MOWHTO. A greater percentage of men (33.3%) had a history of knee arthroscopy as compared with women (15.9%). At the time of MOWHTO, patients with a history of arthroscopy were significantly younger than those without (54.8 vs 57.0 years; P = .002). Male patients with prior arthroscopy underwent MOWHTO at a significantly earlier age than male patients without (53.2 ± 8.4 vs 58.0 ± 5.1 years; P = .002), although there was no such difference in age among the women (55.7 ± 5.5 years for women with prior arthroscopy and 56.7 ± 5.2 years for women without; P = .177). There were no significant differences in baseline characteristics after PSM (Table 1).
Baseline Characteristics Before and After Propensity Score Matching a

a Data are presented as mean ± SD or No. (%). Bold P values indicate statistically significant differences between groups (P < .05). BMI, body mass index; HKA, hip-knee-ankle; K-L, Kellgren-Lawrence.
Clinical Outcomes
Pre- and postoperative outcome scores are shown in Table 2. As compared with the control group, the arthroscopy group had significantly worse postoperative scores on the KOOS–Activities of Daily Living and KOOS–Sport and Recreation, the SF-36 Physical Component Summary, and the Tegner Activity Scale (P = .031, .045, .017, and .007, respectively). However, there was no significant between-group difference on any outcome measure regarding improvement from baseline to final follow-up.
Clinical Outcomes Between the Control and Arthroscopy Groups a

a Values are presented as mean ± SD. Bold P values indicate statistically significant differences between groups (P < .05). ADL, Activities of Daily Living; KOOS, Knee injury and Osteoarthritis Outcome Score; MCS, Mental Component Summary; PCS, Physical Component Summary; SF-36, 36-Item Short Form Health Survey; Sport/Rec, Sport and Recreation.
Postoperative clinical outcome measures based on the interval between knee arthroscopy and MOWHTO are provided in Table 3. Among the patients in the arthroscopy group, 10 underwent MOWHTO within 6 months after knee arthroscopy; 18, within 1 year; 15, within 1 to 2 years; and 37, >2 years after arthroscopy. Based on the Kruskal-Wallis test and Mann-Whitney U test with Bonferroni correction for post hoc comparisons, there were no significant differences in postoperative clinical results between the control group and any arthroscopy subgroup (all P > .05).
Postoperative Clinical Outcomes Based on Time Between Arthroscopy and MOWHTO a
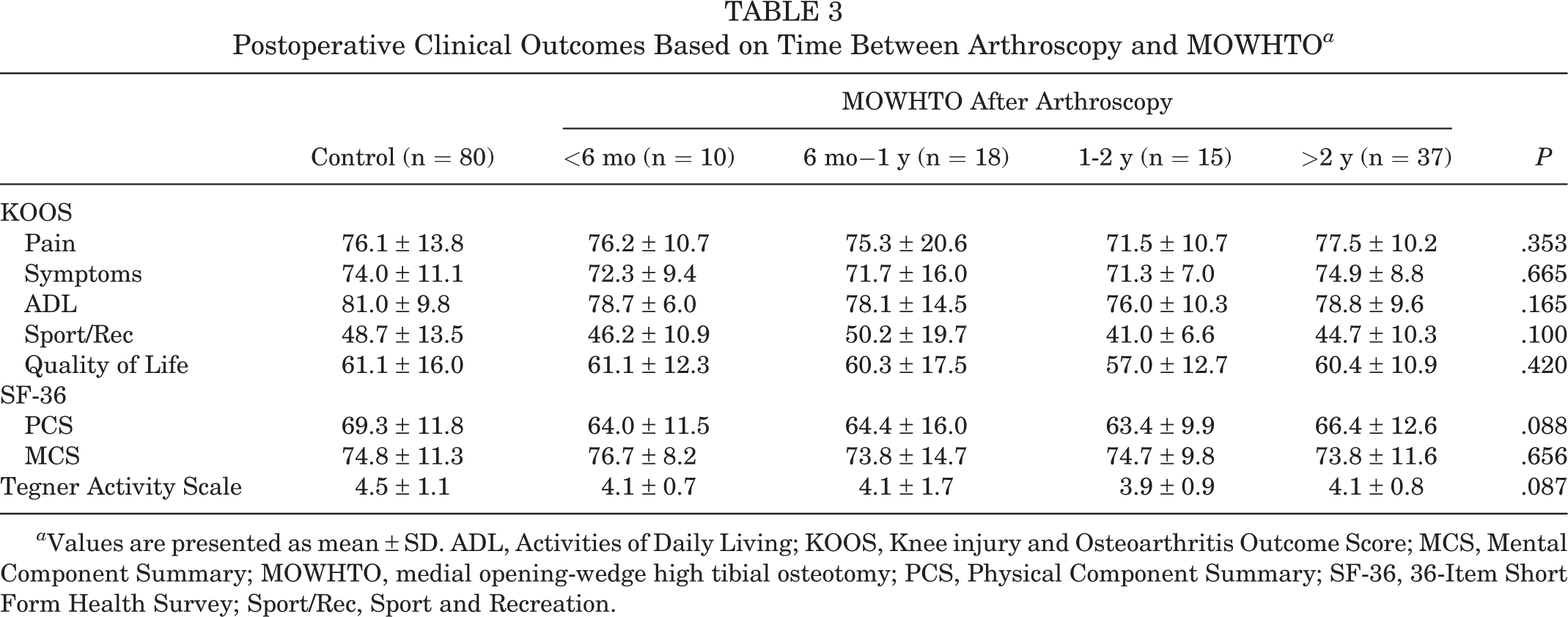
a Values are presented as mean ± SD. ADL, Activities of Daily Living; KOOS, Knee injury and Osteoarthritis Outcome Score; MCS, Mental Component Summary; MOWHTO, medial opening-wedge high tibial osteotomy; PCS, Physical Component Summary; SF-36, 36-Item Short Form Health Survey; Sport/Rec, Sport and Recreation.
Radiological Outcomes and Arthroscopic Findings
Radiological outcomes showed improved knee joint alignment at final follow-up, with no significant differences between the groups (Table 4). Moreover, there were no significant differences in the initial cartilage status findings between the groups.
Radiological Outcomes Between the Arthroscopy and Control Groups a
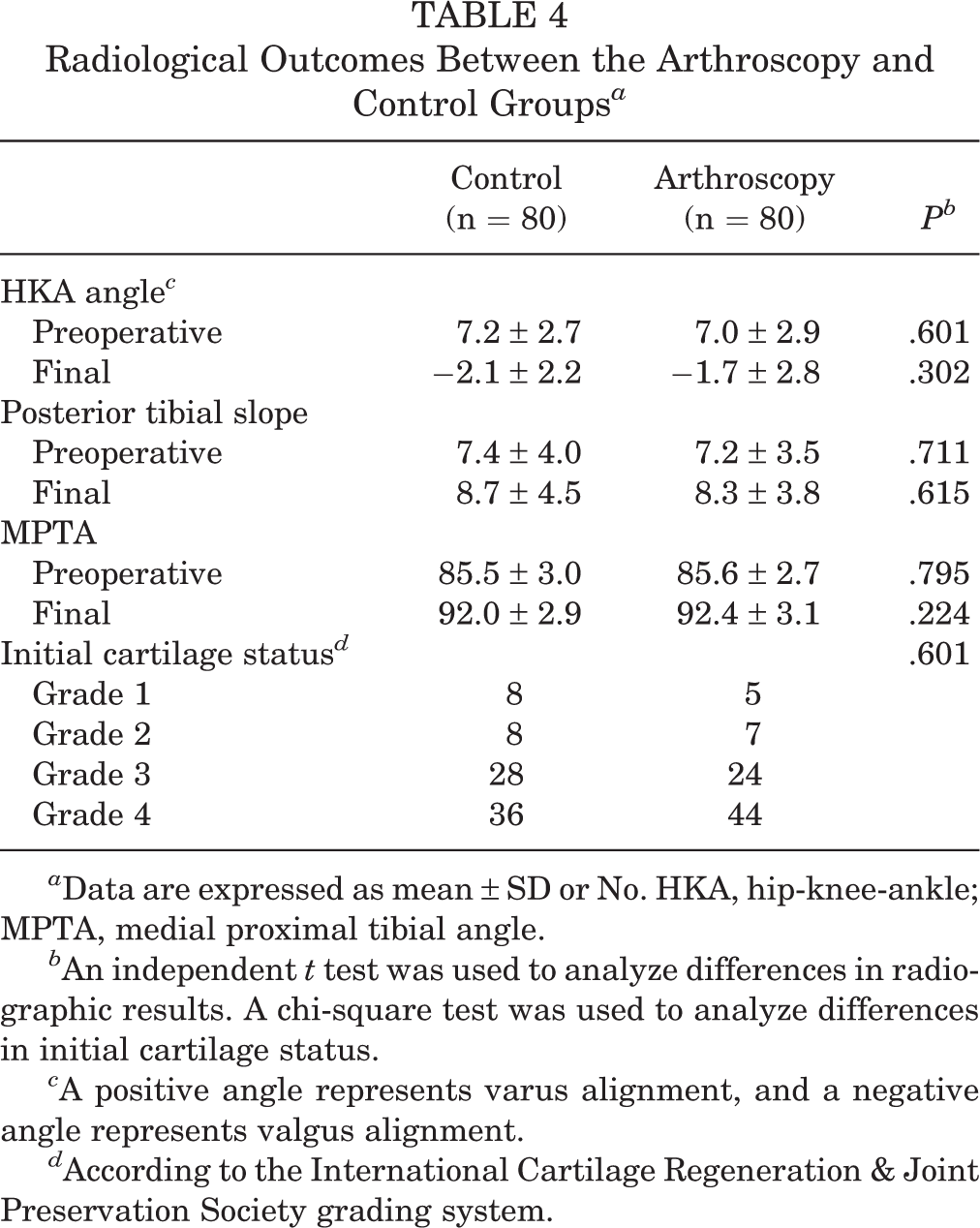
a Data are expressed as mean ± SD or No. HKA, hip-knee-ankle; MPTA, medial proximal tibial angle.
b An independent t test was used to analyze differences in radiographic results. A chi-square test was used to analyze differences in initial cartilage status.
c A positive angle represents varus alignment, and a negative angle represents valgus alignment.
d According to the International Cartilage Regeneration & Joint Preservation Society grading system.
Survival
Kaplan-Meier survival curves for the 160 MOWHTOs are outlined in Figure 2. Five patients underwent conversion to TKA (3 in the arthroscopy group and 2 in the control group), resulting in an overall survival rate of 96.8% (96.5% in the arthroscopy group and 97.3% in the control group) at a mean follow-up of 8 years. There were no significant differences in survival rates based on the presence of prior arthroscopy before MOWHTO (P = .697; log-rank test).
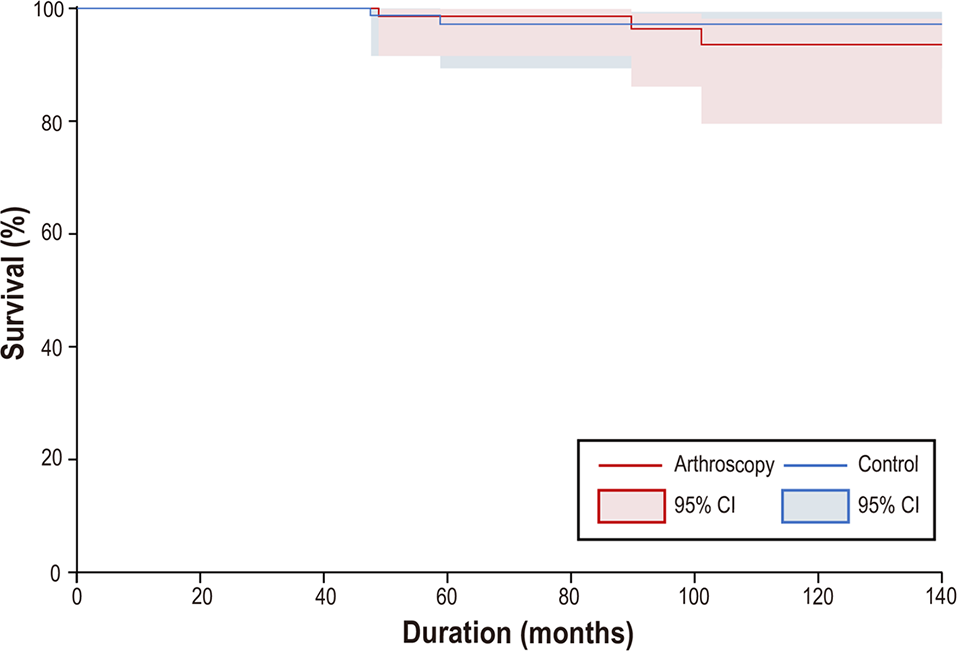
Survival curves (with 95% CIs) for medial opening-wedge high tibial osteotomies (160 knees), with total knee arthroplasty as the end point.
Discussion
This study’s principal findings were that although patients with prior arthroscopy had some inferior patient-reported outcome scores after MOWHTO with relatively small differences between groups, the overall clinical improvements were similar. There were also no significant differences in postoperative clinical results among the groups when subdivided by the interval between arthroscopy and MOWHTO. Regardless of prior arthroscopy, MOWHTO provided good clinical outcomes in terms of pain relief, functional scores, and quality of life and resulted in excellent survival rates during a mean follow-up of 8 years.
To our knowledge, this is the first study to elucidate the outcomes of patients who underwent MOWHTO with prior arthroscopy as compared with a match-controlled cohort with no history of arthroscopic procedures. Our results—specifically, the similar clinical improvement in patient-reported outcomes between patients with prior arthroscopy and those without—are expected to help orthopaedic surgeons establish more precise indications for MOWHTO with realistic expectations.
The role and effectiveness of knee arthroscopy for osteoarthritis have recently been questioned because arthroscopic debridement was found to have no benefit over sham procedures or physical therapy for select patients with this diagnosis. 21,29 Indeed, arthroscopy is still associated with risk and cost and cannot be considered a benign procedure. Prior arthroscopic procedures can lead to intra-articular adhesions, soft tissue scarring, and further cartilage degeneration, thereby possibly leading to impaired functional results. 14,25,37,43 Previous studies have reported conflicting results on the impact of prior knee arthroscopy on TKA outcomes: 1 study showed higher complication and failure rates, whereas another presented no difference in clinical outcomes or survival rates. 17,35
In our study, we evaluated only Korean patients, and their demographic characteristics should be noted before extrapolating our findings to other populations. In Asian populations, MOWHTO tends to be performed more frequently in female than male patients. The results of the present study might have been biased by the disproportionate female sex predominance. 7,12,22,30 In the current study, men were more likely than women to have had knee arthroscopy before MOWHTO, and the effect of prior arthroscopy seemed to be more profound in men, as they underwent MOWHTO nearly 5 years earlier than men without prior arthroscopy. Moreover, patients with prior knee arthroscopy underwent MOWHTO nearly 3 years earlier than patients without prior knee arthroscopy. The potential implications are concerning given the increasing prevalence of arthroscopy as a treatment modality in knee osteoarthritis. The increasing volume of arthroscopic procedures may be a contributing factor in the rising demand for TKA and MOWHTO in younger populations. 6
The benefits of HTO in the significant improvement of patient-reported outcomes with satisfactory survival have been established. 3,10,16,23,46,47 Despite its advantages, several authors have reported the deterioration of outcomes over time, 1,38,39,48 and a probable relationship between prior arthroscopy and inferior MOWHTO outcomes is concerning. Any arthroscopic procedure can influence postoperative clinical results attributed to persistent effusion, pain, or synovitis. 42 Moreover, secondary surgery at the same site may be more difficult, owing to scar tissue formation and changes in tissue relations. 13 In the current study, there were significant between-group differences at the final follow-up regarding the KOOS–Activities of Daily Living, KOOS–Sport and Recreation, SF-36 Physical Component Summary, and Tegner Activity Scale. These results suggest an association between prior arthroscopy and MOWHTO outcomes; however, the improvement in clinical outcome scores did not differ significantly between the groups. Thus, our findings indicated that there was no detrimental effect of prior arthroscopy on postoperative clinical outcomes regardless of gap between arthroscopy and MOWHTO, and we achieved clinical improvements by most measures of outcome, which is in agreement with previous reports. 3,10,15,16,46,47 Yet, a larger prospective study would allow for more comprehensive analysis to determine the optimal timing of MOWHTO.
We found an overall survival rate of 96.8% over a mean follow-up of 8 years, which is comparable with previous reports. 4,8,10,46,47 MOWHTO provided a satisfactory survival rate and stable outcomes throughout the study period, despite the presence of prior arthroscopy. There were no intergroup differences in the survival rate based on prior arthroscopy, although a prospective study with a longer follow-up duration is needed to verify this correlation.
Limitations
Our study has certain limitations. First, all arthroscopic procedures are not identical. We attempted to decrease this bias by including only nonligamentous arthroscopic procedures. Second, this study was based on a retrospective review of a relatively small population. Third, as this study recruited patients from a single center, observer or selection biases cannot be eliminated. Finally, although we performed a match-controlled study to minimize selection bias, it is possible that there are other variables, including the tibial bone varus angle, that could have been controlled for that may have led to alternative results. Nevertheless, we believe that our study provides a reasonable evaluation of the effects of arthroscopy on midterm clinical outcomes and survival rates after MOWHTO. Our findings are clinically relevant and can help with clinical decision making during the management of knee osteoarthritis using MOWHTO in patients with prior knee arthroscopy.
Conclusion
Although patients with prior arthroscopy had some inferior patient-reported outcome scores after MOWHTO with relatively small differences between groups, the overall clinical improvements were similar. We found no difference in regard to time from arthroscopy. This is potentially useful information that orthopaedic surgeons should consider when counseling patients undergoing knee arthroscopy. These findings provide evidence that surgeons should not eliminate MOWHTO as a treatment modality based on prior arthroscopy alone, as our study shows excellent survival rates regardless of arthroscopic history.
Footnotes
Final revision submitted February 10, 2023; accepted March 2, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by a Korea Medical Device Development Fund grant, which is funded by the Korean government (the Ministry of Science and ICT, the Ministry of Trade, Industry and Energy, the Ministry of Health and Welfare, the Ministry of Food and Drug Safety; project 9991007120, KMDF_PR_20210525_0001). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Chonnam National University Hwasun Hospital (No. CNUHH-2022-040).