
Abstract
Background:
Fatty infiltration in the subscapularis muscle extends to the upper portion of the muscle first and then to the lower portion only after some degree of fatty change has taken place in the upper region. Although the Goutallier classification is the most widely used method to categorize fatty infiltration, how to accurately and reliably determine the extent of infiltration is controversial.
Purpose:
To examine a modified classification that is more reliable in (1) assessing fatty infiltration of the subscapularis muscle and (2) predicting the structural integrity of the repaired tendon by identifying cutoff points for retear.
Study Design:
Cohort study (diagnosis); Level of evidence, 3.
Methods:
This study retrospectively examined the records of 545 patients who underwent arthroscopic repair for a subscapularis tear. Two shoulder surgeons reviewed the preoperative magnetic resonance imaging scans of all enrolled patients and evaluated the fatty infiltration of the subscapularis muscle based on the original Goutallier classification, as well as a novel modified Goutallier classification designed to measure the proportion of fat and muscle in the upper and lower portions of the muscle separately. Intra- and interobserver agreement of the reviewers was calculated using κ statistics. Using receiver operating characteristic curve analysis, we determined the cutoff point for the particular fatty infiltration grade related to the occurrence of retear for each classification scheme.
Results:
The κ values for interobserver reliability were 0.743 and 0.856 for the original and modified Goutallier classifications, respectively, with the modified classification having significantly higher reliability (Z = 4.064; P < .001). Cutoff points for the fatty infiltration grade associated with retear were 2.5 for the original Goutallier classification (sensitivity, 65.3%; specificity, 95.6%; accuracy, 87.8%) and 3.5 for the modified classification (sensitivity, 52.5%; specificity, 97.8%; accuracy, 89.7%).
Conclusion:
In assessing fatty infiltration of the subscapularis muscle, the modified Goutallier classification showed higher reliability than the original Goutallier classification. The cutoff point for potential retear (grade 3.5) was at a point where the fatty infiltration extended to the lower portion of the subscapularis muscle.
Fatty infiltration in the rotator cuff muscles has been widely used to predict the reparability of the tendons, since it is known to reflect the chronicity of tears. 19,33,44,47,50 For a posterosuperior rotator cuff (PSRC) tear, preoperative magnetic resonance imaging (MRI) scans to determine findings such as tear size, extent of retraction, and tear configuration in addition to extent of fatty infiltration can be used to assess the possibility of repair. 4,25,39,41 However, since the retraction of a torn subscapularis tendon is less common than tears of the supraspinatus tendon, given the position of the transverse humeral ligament over the bicipital groove, the tear size or extent of retraction is difficult to accurately evaluate by MRI. 22,23,51,52 Thus, the use of MRI to assess the extent of muscle atrophy or fatty infiltration can predict the reparability of a tear, and it is imperative to accurately evaluate the degree of fatty infiltration in the subscapularis muscle.
A subscapularis tendon tear generally begins in the upper and intra-articular portion of the tendon and extends inferiorly over time 10,11,14,21,35,36 ; the natural course of fatty infiltration in a subscapularis tear differs from that in tears in other rotator cuff muscles, where fatty infiltration is evenly distributed. Although the Goutallier classification is the most widely used method to categorize fatty infiltration, 2,14,27,29,30 determining the extent of infiltration accurately and reliably is controversial among surgeons. Moreover, there has been no study on whether the classification can be appropriately used to determine fatty infiltration grade in the subscapularis muscle.
In this study, we aimed (1) to compare the reliability of a novel modified Goutallier classification for assessing fatty infiltration of the subscapularis muscle and for predicting the structural integrity of the repaired tendon and (2) to compare the cutoff points for retear between the modified and original Goutallier classifications. We hypothesized that a more detailed classification of fatty infiltration in the subscapularis muscle will provide greater reliability than the Goutallier classification and better prediction of postoperative tendon integrity.
Methods
Study Population
We reviewed the records of 724 patients who underwent repair of the subscapularis tendon (an isolated or combined tear) between March 2009 and February 2019 at our institution. Indications for repair were signs of weakness during internal rotation on physical examination (belly press or modified belly press test) in the context of an evident subscapularis tendon tear on MRI and lack of response to nonoperative treatments after >3 months. In addition, for those without an apparent subscapularis tendon tear on preoperative MRI, repair of the tendon was performed when patients showed weakness during internal rotation and a partial-thickness subscapularis tear >50% intraoperatively.
Exclusion criteria were (1) a history of ipsilateral shoulder surgery (25 patients), (2) low-quality preoperative MRI for fatty infiltration grade determination (47 patients), (3) no follow-up MRI scan at 6 months after surgery for evaluation of tendon structural integrity (65 patients), and (4) partial repair of a large tear (48 patients). A total of 179 patients (6 patients met two exclusion criteria) were excluded, and the remaining 545 were included in the final evaluation. Our institutional review board approved this study and waived the requirement for patient informed consent.
Assessment and Repair of Subscapularis Tendon Tears
All surgical procedures were performed by a single surgeon (Y.-M.C.) with the patient in the beach-chair position under general anesthesia. The grade of the subscapularis tendon tear was assessed according to the Lafosse classification using a posterior portal and a 70° arthroscope. The full-thickness tear of the subscapularis tendon was also assessed in the subacromial space via a lateral viewing portal with use of a 70° arthroscope during the repair.
When the subscapularis tendon tear was classified as Lafosse type 1 with a partial-thickness tear >50%, a transtendon repair was performed by accessing the intra-articular space using a single suture anchor. Tears that were Lafosse type ≥2 were repaired by accessing the subacromial space in a single-row fashion with 1 or 2 suture anchors.
Goutallier and Modified Goutallier Classifications
Since the original Goutallier classification assesses the proportion of fat and muscle over an entire muscle, the grades in the subscapularis muscle may not represent the actual state of fatty infiltration, especially for a Goutallier grade 3, where the proportion of muscle and fat is the same. The modified Goutallier method was designed to measure the proportion of fat and muscle in the upper and lower portions of the muscle separately. The original and novel modified Goutallier classifications are listed in Table 1, and examples of each modified Goutallier grade on MRI are shown in Figure 1.
Original and Novel Modified Goutallier Classifications for Fatty Infiltration of the Subscapularis

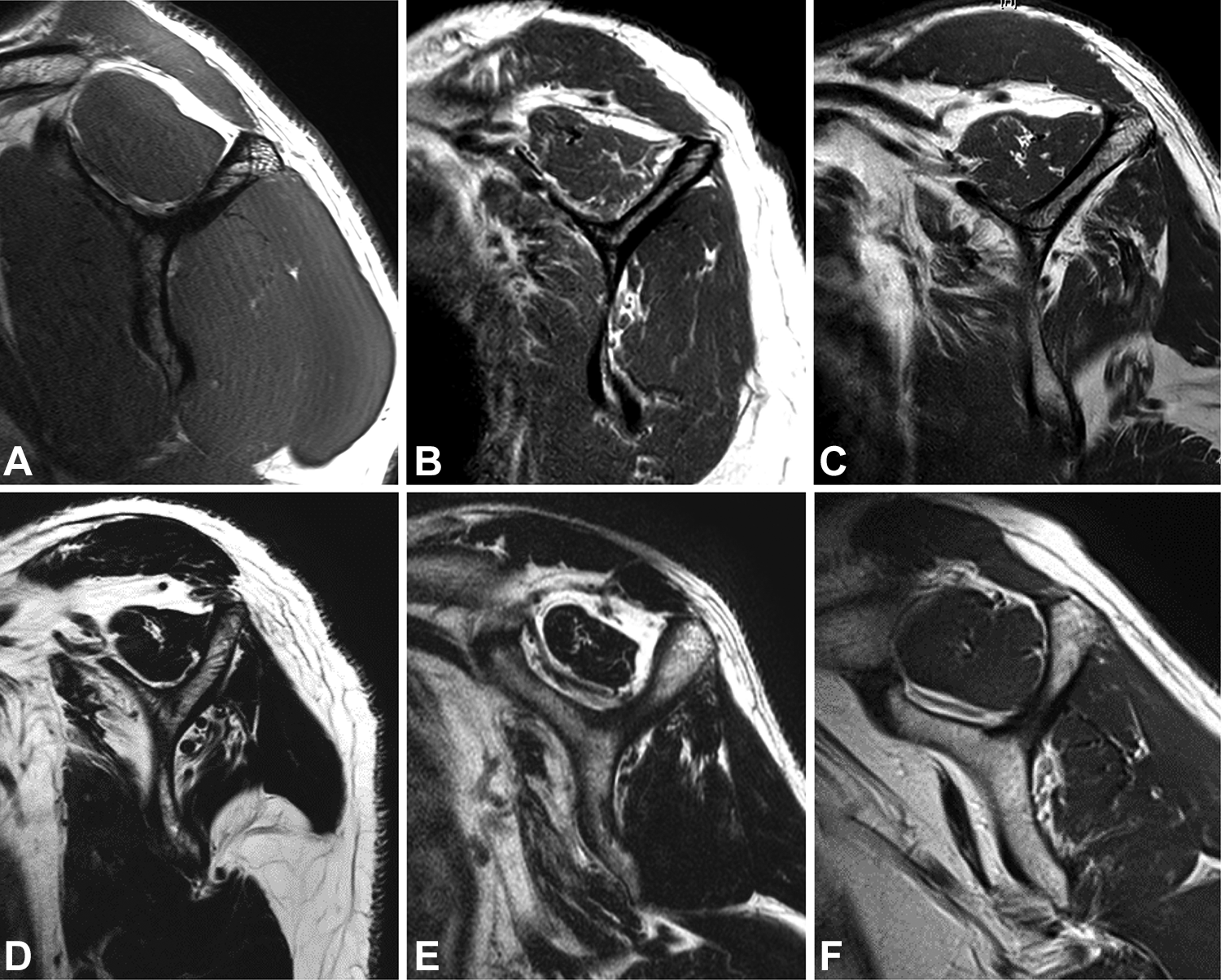
Examples of the modified Goutallier classification grades on sagittal T1-weighted magnetic resonance scans of the subscapularis muscle. (A) Grade 0: no fat. (B) Grade 1: some fatty streaks. (C) Grade 2: less fat than muscle in the upper half of the muscle. (D) Grade 3: more fat than muscle in the upper half of the muscle, with normal or fatty streaks in the lower half of the muscle. (E) Grade 4: more fat than muscle in the upper half of the muscle, with less fat than muscle in the lower half of the muscle. (F) Grade 5: more fat than muscle in the upper and lower halves of the muscle.
MRI Assessment
Two orthopaedic fellows who specialized in shoulder surgery (T.-H.Y., J.-H.O.) reviewed MRI scans of all enrolled patients and evaluated the grade of fatty infiltration in the subscapularis muscle using the original and modified Goutallier classifications. Measurements were made with the most lateral T1-weighted sagittal oblique image, in which the scapular spine contacted the scapular body (Y view). 24,45 Each examiner measured the fatty infiltration grades twice at an interval of 4 weeks. When the recorded grades differed between the observers, fatty infiltration was reevaluated, and a grade was determined by concurrence of both examiners.
Follow-up MRI scans (3.0 T, MAGNETOM Tim Trio; Siemens) were obtained 6 months after surgery to assess the integrity of the repaired subscapularis tendon: these were interpreted by the same orthopaedic fellows who graded fatty infiltration.
Statistical Analysis
To calculate the reliability of the 2 classification systems, the κ statistic was used to measure the intra- and interobserver agreement of the examiners. Agreement was categorized as nearly perfect (κ = 0.81-0.99), substantial (κ = 0.61-0.80), moderate (κ = 0.41-0.60), fair (κ = 0.21-0.40), or slight (κ ≤ 0.20). 8 In addition, the agreement rate for each grade provided by the 2 examiners was calculated. To compare the reliability between the classifications, a 2-sample Z test was performed for the κ comparison. 5,6,42,49
Univariate logistic regression analysis was performed to identify the relationship between each classification grade and the presence of subscapularis retear on 6-month follow-up MRI. Then, according to a receiver operating characteristic curve, the cutoff point for the particular grade of fatty infiltration related to the occurrence of a retear was determined for each classification scheme. Statistical analysis was performed with SPSS (Version 25.0; IBM), and P < .05 was defined as significant.
Results
Of the 545 patients (288 male, 257 female; mean ± SD age, 63.9 ± 6.9 years), combined subscapularis tendon and PSRC tears were found in 88.8%, while the rest (11.2%) had an isolated subscapularis tendon tear.
The grading of tears according to each classification is shown in Table 2. The κ values (± SE/SEM) for intraobserver reliability indicated substantial agreement for the Goutallier classification (0.693 ± 0.057 for examiner 1 and 0.721 ± 0.041 for examiner 2) and nearly perfect agreement for the modified classification (0.872 ± 0.026 and 0.847 ± 0.031, respectively). The κ values for interobserver reliability also indicated substantial agreement for the Goutallier classification (0.743 ± 0.043) and nearly perfect agreement for the modified classification (0.856 ± 0.033); the difference in interobserver reliability was significantly higher in the modified Goutallier classification (Z = 4.064; P < .001). The interobserver agreement rates for each grade of Goutallier classification showed an increased discrepancy between examiners for grade 2 (77.2%) and grade 3 (65.6%). Table 3 shows how tears for each grade according to original Goutallier classification were reclassified according to the modified classification.
Grading, Interobserver Agreement, and Retears on Follow-up Magnetic Resonance Imaging
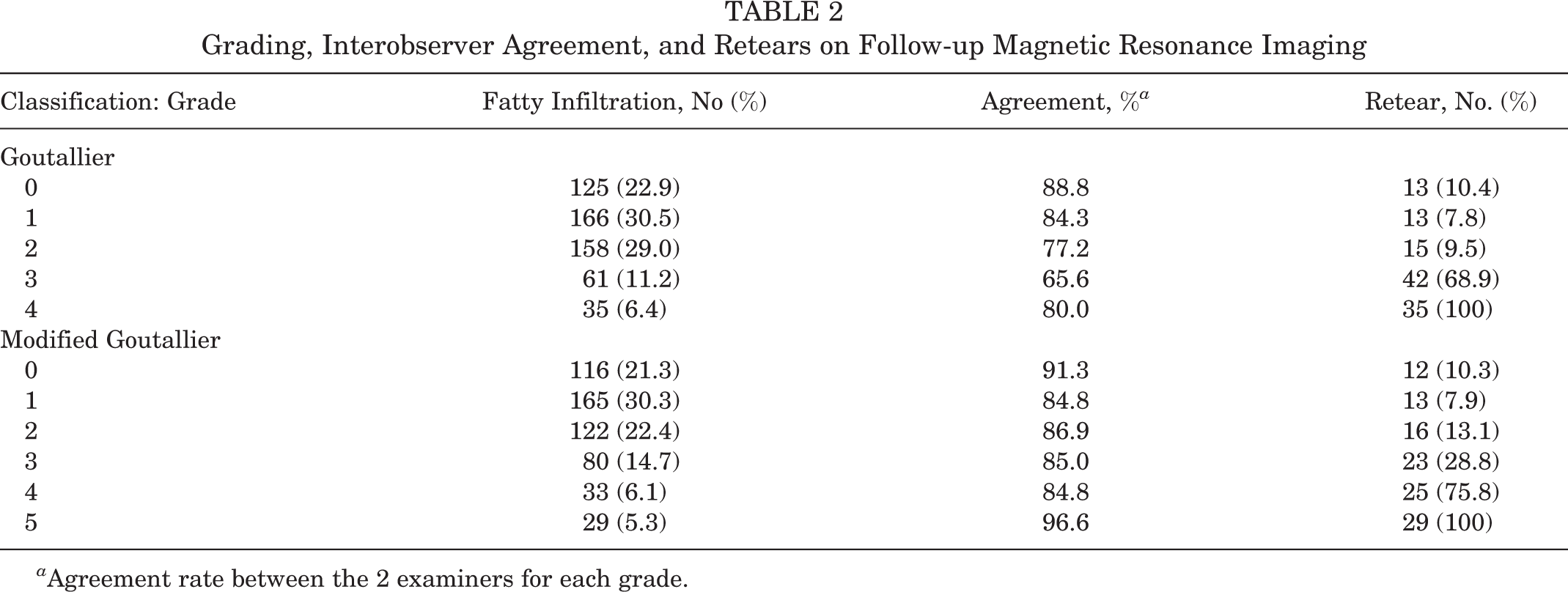
a Agreement rate between the 2 examiners for each grade.
Tears Classified as Goutallier and Modified Goutallier Classifications (N = 545)
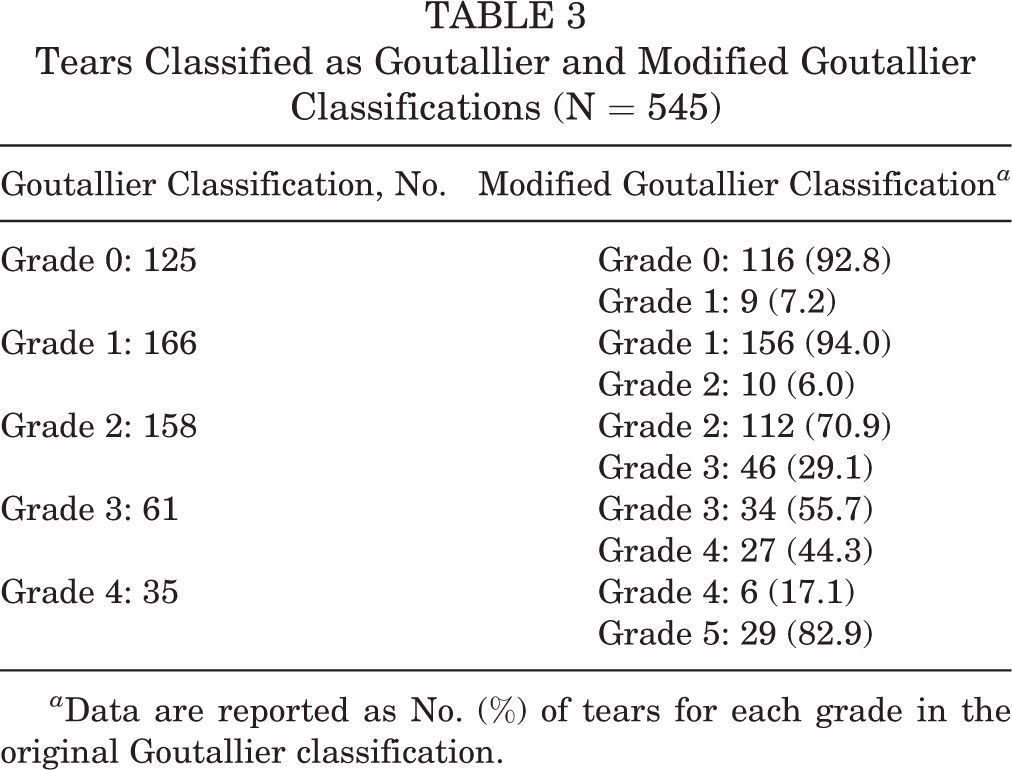
a Data are reported as No. (%) of tears for each grade in the original Goutallier classification.
Of the 545 patients, 21.7% had a retear on follow-up MRI. Logistic regression analysis showed a statistically significant increase in retears as the fatty infiltration grade increased in the Goutallier classification (P < .001; odds ratio, 3.805 [95% CI, 2.937-4.929]) and modified Goutallier classification (P < .001; odds ratio, 2.877 [95% CI, 2.352-3.519]). Based on receiver operating characteristic curve analysis, the area under the curve was 0.808 for the original Goutallier classification and 0.800 for the modified classification, and the cutoff point for the fatty infiltration grade associated with a retear was 2.5 (sensitivity, 65.3%; specificity, 95.6%; accuracy, 87.8%) for the original Goutallier classification and 3.5 (sensitivity, 52.5%; specificity, 97.8%; accuracy, 89.7%) for the modified classification.
Discussion
The purpose of this study was to evaluate whether the Goutallier classification is appropriate for assessing fatty infiltration of the subscapularis muscle. As hypothesized, the modified Goutallier classification resulted in significantly higher interobserver reliability than the original classification (Z = 4.064; P < .001).
Among the many methods of assessing fatty infiltration, the Goutallier classification is used most widely in clinical and research settings. Currently, instead of axial images on computed tomography, investigators modify and apply sagittal Y views of MRI scans where the grades are established by visualizing the proportions of muscle and fat. 12 However, because the classification is based on semiquantitative criteria, there have been discrepancies in interobserver reliability, with a broad range of κ values reported (0.24-0.82). 15,18,26,31,34,38 Hence, some have suggested the need for new classification systems. Slabaugh et al 40 proposed a simplified Goutallier classification that merges grades 0 and 1 and grades 2 and 3. In addition, most studies have examined the reliability of grading supra- and infraspinatus muscles. Although the initiation and configuration of tears in the supra- and infraspinatus tendons vary, fatty infiltration in these muscles appears to progress and spread over the entire muscle uniformly. In contrast, since most tears of the subscapularis tendon begin at the upper margin and progress to the lower portion, fatty infiltration of this muscle characteristically progresses throughout the upper portion first and later extends to the lower portion as well. Thus, fatty infiltration of the subscapularis muscle should be considered and evaluated differently from that of the supra- and infraspinatus muscles.
Another particular characteristic of the subscapularis muscle is that fatty infiltration seems to eventually progress to the lower portion of the muscle after fatty infiltration of the upper portion is advanced. The upper two-thirds of the subscapularis muscle is anatomically composed of a tendinous region that is inserted into the superior and middle portions of the lesser tuberosity of the humerus. Yet, the muscle’s inferior one-third is composed of a thin membranous structure that is inserted into the inferior aspect of the lesser tuberosity and metaphysis of the humerus. 1,7,9,28,48 In addition, studies on neuromuscular partitioning noted that diverse nerves innervate different portions of the muscle. 3,17,37,43,46 The superior and middle portions are innervated by a branch that originates from the posterior cord, and the inferior portion is innervated by different branches originating from the axillary nerve. Hence, the upper and lower portions of the subscapularis muscle appear to function as independent muscle units, and fatty infiltration thus appears to develop and progress differently in the superior and inferior parts of the muscle. For this reason, assessing fatty infiltration of the subscapularis muscle with the Goutallier classification can be ambiguous. The modified Goutallier classification was designed to measure the proportion of fat and muscle in both portions of the subscapularis separately.
In this study, a Goutallier grade of 2.5 and a modified Goutallier grade of 3.5 were found to be the cutoff points to predict a potential retear of a repaired subscapularis tendon. Thus, a Goutallier grade 3 can be regarded as an important clinical indicator. However, in this study, the agreement rate between the examiners using the existing Goutallier classification was only 65.6%; the grade should be more specifically defined to minimize an under- or overassessment and to raise the concurrence rate among examiners during preoperative planning. Considering that the cutoff point for a retear was grade 3.5 in the modified classification, the possibility of a retear increases in the presence of advanced fatty infiltration in the upper half of the subscapularis muscle. Since this cutoff point is determined not by measuring the distribution of fat and muscle throughout the entire subscapularis muscle but by identifying the presence of a greater proportion of fat in the upper portion of the muscle, early diagnosis and prompt treatment are considered necessary.
Limitations
The inclusion of cases with a combined PSRC tear is a limitation of this study. However, evaluations of isolated and combined tears were performed because there is a high possibility of a type 2 error owing to the smaller number of cases with only an isolated tear, and any relation between PSRC integrity and a retear of a repaired subscapularis tendon has not been confirmed. In addition, since many isolated subscapularis tendon tears with fatty infiltration of grade ≥3 are generally treated nonoperatively because of the high possibility of a retear, enrollment of patients with combined tears and those with surgically treated isolated tears was necessary for the evaluation and analysis. Furthermore, apart from including the integrity of a PSRC and its effect, another limitation of the current study is the evaluation without considering demographic factors, such as age, tobacco use, work level, and others, that may affect the retear rate. Last, even though a large number of images were reviewed, the interrater reliability that was assessed and reported by only 2 observers does not provide sufficient evidence for generalizability; therefore, gathering and examining more results from a larger number of observers is required in the future.
Conclusion
In assessing fatty infiltration of the subscapularis muscle, the modified Goutallier classification showed higher reliability. The cutoff for a potential retear (grade 3.5) was at a point where the fatty infiltration extends to the lower portion of the subscapularis muscle.
Footnotes
Final revision submitted February 20, 2023; accepted March 2, 2023.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Severance Hospital, Yonsei University (No. 4-2022-0831).