
Abstract
Background:
To evaluate the burden of overuse injuries, the Oslo Sports Trauma Research Centre (OSTRC) questionnaire on health problems (OSTRC-H2) was developed in English in 2013.
Purpose:
To translate and culturally adapt the OSTRC-H2 into French and investigate the reliability and validity of this new version.
Study Design:
Cohort study (diagnosis); Level of evidence, 3.
Methods:
The OSTRC-H2 was translated from English to French according to international guidelines. A total of 80 elite athletes were then invited to complete the OSTRC-H2 weekly for 3 months. Potential ceiling effects, construct validity, and reliability were investigated. Convergent validity was measured using Pearson correlations for continuous items and kappa coefficients for binary items; internal consistency was measured using the Cronbach alpha coefficient; and test-retest reliability was measured using the intraclass correlation coefficient (ICC). Separate analyses were performed on the entire cohort of athletes (population 1 [P1]) and on athletes who reported a health problem during the follow-up (P2).
Results:
A total of 80 elite athletes took part in this study. The response rate was very high, with 909 of 960 questionnaires returned (95%). The mean weekly prevalence of health problems was 19.6% during the follow-up period. Nineteen participants reported a health problem during the follow-up (P2). The OSTRC-H2 showed very good test-retest reliability for both populations (ICC, 0.85 [95% CI, 0.77-0.90] for P1; ICC, 0.90 [95% CI, 0.68-0.98] for P2). Internal consistency was very good for P2 (Cronbach α = .94). The OSTRC-H2 demonstrated high concordance with the visual analog scale of symptom intensity (r = 0.52; P < .05), and low concordance with the overtraining questions from the Questionnaire de la Société Française de Médecine du Sport (κ from –0.01 to 0.12; P > .05).
Conclusion:
The French version of the OSTRC-H2 was found to be valid and reliable when applied to French-speaking elite athletes.
Keywords
Prevention of injury and illness is an essential aspect of sports medicine, as it can significantly impact the physical fitness, performance, and success of athletes. The first step in developing comprehensive injury prevention programs is to understand the extent of the problem. Injury surveillance systems are therefore essential for monitoring and tracking physical symptoms and injuries. However, many challenges have been highlighted in recording the magnitude of overuse injuries using established injury surveillance methods. 1 For example, athletes often continue to practice and participate in competitions despite overuse injuries, which makes the exact point of injury occurrence difficult to define. To evaluate the burden of overuse injuries more adequately, the Oslo Sports Trauma Research Center questionnaires on overuse injury (OSTRC-O) and health problems (OSTRC-H) were developed in 2013 by Clarsen et al. 5,6 Both questionnaires consist of 4 key questions on the presence of physical and health complaints during the past 7 days, their effect on sports activity, and the intensity of symptoms. Athletes are requested to complete the questionnaires regularly throughout the course of a surveillance period. The OSTRC-O is focused on injury complaints in predetermined areas (eg, the shoulder, lower back, or knee), whereas the OSTRC-H includes a broader definition of health complaints, including illnesses and injuries in any anatomic region. In 2020, Clarsen et al 4 provided a revised version of the OSTRC-H: the OSTRC-H2. The total score of the questionnaire varies from a score of 0, indicating no problems, to a score of 100, indicating complete inability to participate in sports. For athletes reporting any health problems, the OSTRC-H2 delves into the type of complaint (injury or illness), the area (in cases of injury), or symptoms (in cases of illness).
The Swedish, 8 Danish, 5 Japanese, 14 Thai, 10 and Spanish 2 versions of the OSTRC-O have been validated. Only the Japanese 14 and Spanish2 versions of the OSTRC-H have been translated and validated.
No tools in the French language are currently available to register the occurrence and consequences of health problems among athletes. Therefore, the purpose of this study was to translate the OSTRC-H2 questionnaire into French. Furthermore, we aimed to evaluate the measurement properties of the translated version of the OSTRC-H2 among French-speaking elite athletes to confirm its validity and reliability in this population. We hypothesized that the French version of the OSTRC-H2 would be valid and reliable.
Methods
The Strengthening the Reporting of Observational Studies in Epidemiology checklist for cross-sectional studies was used as a guideline in this study. The study protocol received ethics committee approval, and all study participants provided written informed consent.
This study had 2 continuous phases. First, the OSTRC-H2 questionnaire was translated from English to French, culturally adapted, and pretested among a restricted sample of 9 elite athletes. The translation was based on a standardized method, adhering to Beaton international cross-cultural adaptation recommendations for questionnaires measuring health status. 3 Second, to evaluate the validity and reliability of the questionnaire, elite athletes were invited to complete the French version of the OSTRC-H2 questionnaire twice: once at inclusion and once again after 24 to 72 hours. Additionally, to estimate the prevalence of health problems reported during the follow-up, all athletes included in the study were asked to complete the OSTRC-H2 questionnaire every week for 3 months. The measurement properties of the questionnaire were assessed according to the Consensus-based Standards for the Selection of Health Status Measurement Instruments recommendations. 13
OSTRC-H2 Questionnaire
The OSTRC-H2 consists of 4 key items covering 2 objectives: (1) to detect the presence of physical or health complaints and (2) to evaluate the severity of the problem using a score between 0 and 100, with 0 representing no impact and 100 representing the maximum impact on sports activity. Item 1, which consists of 4 response options, is scored as 0, 8, 17, and 100. Items 2, 3, and 4, with 4 response options, are scored as 0, 8, 17, and 25. Athletes with a score of 100 in item 1 (“Could not participate due to a health problem”) did not answer items 2, 3, and 4. Those who selected the third or fourth response option in either item 2 or 3 or the fourth option in item 1 were considered to have substantial problems.
Study Participants
French-speaking elite athletes aged ≥18 years who were competing at national or international levels were recruited for this study. Athletes were recruited via 3 sources: (1) coaches and managers of different clubs belonging to the Ligue Francophone (“League of French-Speaking Athletes”) from different athletic disciplines; (2) high-level athletes enrolled at the Liège University, Belgium, and invited via an email invitation; and (3) through social networks. Excluded were athletes with an injury that fully prevented them from participating in sports.
Once contacted, athletes willing to participate were sent an email invitation to sign up to an online platform (AthleteMonitoring; FitStats Inc; http://www.athletemonitoring.com), where all questionnaires were available to be completed.
Procedures
Phase 1. French Translation, Cultural Adaptation, and Pretest of the OSTRC-H2
After obtaining permission to translate from the authors of the original version of the OSTRC-H2 questionnaire, 6 the OSTRC-H2 questionnaire was first translated from English to French by 2 French native translators(including S.B.), both fluent in English. The 2 translators then met to obtain a consensual first version of the French OSTRC-H2. This French version was then back-translated by 2 native English-speaking translators, fluent in French. Third, an expert panel, including the translators and the research team members, agreed on a prefinal version of the French OSTRC-H2. Finally, the prefinal version was submitted as a pretest to a sample of 9 elite athletes to assess its comprehensibility and clarity. The athletes were asked to comment on each of the questions and explain in their own words what they understood from those questions. The degree to which their understanding and each question’s intended meaning were consistent was assessed.
Phase 2. Investigation of the Measurement Properties of the OSTRC-H2
In addition to the OSTRC-H2, participants received 2 other questionnaires as convergent instruments to assess construct validity: (1) the overtraining questionnaire from the Société Française de Médecine du Sport (SFMS; “French Society of Sports Medicine”) 11 and (2) a visual analog scale (VAS) to estimate the intensity of health problems/injury/symptoms. Initially, all athletes completed the French version of the OSTRC-H2, SFMS, and VAS via the online platform. To test the reliability of the questionnaire, athletes were invited to complete the OSTRC-H2 once more the next day. A maximum interval of 72 hours was accepted for test-retest reliability. Then, participants were invited to directly complete the OSTRC-H2 on the same platform each week. All athletes received an automatic email reminder weekly. Four dichotomous questions were submitted to participants at the end of the study period to assess their opinion and acceptability of the questionnaire.
Measurement Properties
All measurement properties were investigated on 2 distinct populations: (1) the full cohort (population 1 [P1]) and (2) the restricted population of athletes who reported any health problem during the follow-up (P2). The clinometric properties of acceptability, convergent validity, internal consistency, test-retest reliability, and ceiling effects were investigated for each population.
Acceptability
Following the methodology employed in similar translation studies, 8,14 we requested athletes to complete 4 qualitative questions (yes/no responses) about their opinion and acceptability of the questionnaire: (1) Do you consider the questionnaire to contain relevant questions regarding the sport you are participating in? (2) Was the questionnaire difficult to complete? (3) Would you like to change or add any questions to the questionnaire? If so, please specify; and (4) Do you think that the web-based method works well? After each question, a space was provided for the athletes to add their comments.
Convergent Validity
The correlation between the OSTRC-H2 and the SFMS was used to measure convergent validity. Nine different hypotheses of correlations were consensually developed with the research team (Table 1). The Pearson correlation coefficient (r) was reported for continuous items, and the kappa coefficient (κ) was reported for binary items. The κ values were interpreted as follows: no agreement (≤0); none to slight agreement (0.01-0.20); fair agreement (0.21-0.40); moderate agreement (0.41-0.60); substantial agreement (0.61-0.80); and almost perfect agreement (0.81-1.00). 12 We considered moderate agreement and higher as a confirmation of our convergent validity hypotheses.
Hypotheses Developed to Measure Convergent Validity a

a OSTRC-H2, Oslo Sports Trauma Research Centre Questionnaire on Health Problems; SFMS, Société Française de Médecine du Sport; VAS, visual analog scale.
Internal Consistency
The Cronbach alpha (α) was used to measure internal consistency, which reflects the homogeneity of the scale, with values between 0.7 and 0.95 reflecting good internal consistency. 15 We also assessed the impact of each item on the overall internal consistency by removing 1 item at a time.
Test-Retest Reliability
Participants completed the OSTRC-H2 twice, with a 1-day interval period. Only participants who did not report any health changes between the 2 assessments were considered. Test-retest reliability was evaluated using the intraclass correlation coefficient (ICC) (2-way mixed, absolute agreement). Test-retest reliability improves as the ICC approaches 1, and an ICC >0.7 is indicative of an acceptable reliability. 7
Ceiling Effects
We defined the presence of a ceiling effect as >15% of the population obtaining the maximum score. Floor effects were not measured, as a score of 0 on the OSTRC-H2 simply reflects the nonoccurrence of health problems during the follow-up period.
Statistical Analysis
All statistical analyses were computed using SPSS Version 25 (IBM). Descriptive statistics were used to characterize the included population, for which the Gaussian distribution of all quantitative variables was tested using the Shapiro-Wilk test, histograms, quantile-quantile plots, and the difference between mean and median. Variables with normal distribution were presented using means and standard deviations, and variables with nonnormal distribution were presented using medians and interquartile ranges. Qualitative and binary variables were presented using relative and absolute frequencies. Statistical significance was set at P < .05.
Results
Phase 1. French Translation, Cultural Adaptation, and Pretest of the OSTRC-H2
The OSTRC-H2 was translated into French without any major difficulties. The prefinal version was pretested on a sample of 9 French-speaking elite athletes from Belgium, France, and Libya. As none of the athletes reported any problems understanding the questionnaire, and it was validated by the expert committee, the prefinal version became the definitive final version (available separately as supplemental material).
Phase 2. Measurement Properties of the OSTRC-H2
A sample of 80 elite athletes (63 men and 17 women; median age, 21.5 years) were included in the validation phase of the OSTRC-H2. Participants mainly performed track and field (n = 15), handball (n = 12), hockey (n = 10), football (n = 8), and basketball (n = 6), reporting a median training duration of 9.4 hours per week. Participant characteristics are reported in Table 2.
Characteristics of the Included Population (N = 80) a

a Data are reported as n (%) or median [interquartile range].
b Other sports practiced included biathlon, boxing, and dancing.
All 80 athletes were evaluated over 12 consecutive weeks. The response rate was very high, with 909 of 960 questionnaires returned (95%). Among the 80 participants, 19 (23.7%) reported a health problem (illness or injury) during the follow-up period. The mean weekly prevalence of health problems was 19.6% (95% CI, 18.1-21.1). No significant difference was observed between participants who did not report any health problem (n = 61) and participants who reported a health problem (n = 19) in age, sex, mean hours of sports activity per week, or category of sports. The mean prevalence of substantial health problems was 10.2% (95% CI, 9.48-10.9). The highest mean prevalence belonged to overuse injuries (9.6% per week), followed by traumatic injuries (8.9%) and illness (1.94%)

Prevalence of all health issues and substantial health issues during the follow-up.
Acceptability
To measure the acceptability of the questionnaire, 66 athletes (82.5%) were asked to complete the 4 additional questions. Almost all athletes (92.5%) agreed that the questions were relevant to their sport, no athletes reported any difficulty in completing the questionnaire, and 12 athletes made recommendations on how to improve the questionnaires (eg, add more symptoms to the list such as burns). Almost all athletes (98.5%) reported that data collection via the internet was simple and relevant.
Convergent Validity
As 9 participants did not complete the SFMS or VAS, construct validity was measured on 71 participants in P1 and 16 participants in P2. Only hypothesis 9 was confirmed. No significant association was found between the OSTRC-H2 and any hypotheses related to the SFMS (Table 3).
Construct Validity of the OSTRC-H2 (Association With the SFMS and VAS) a
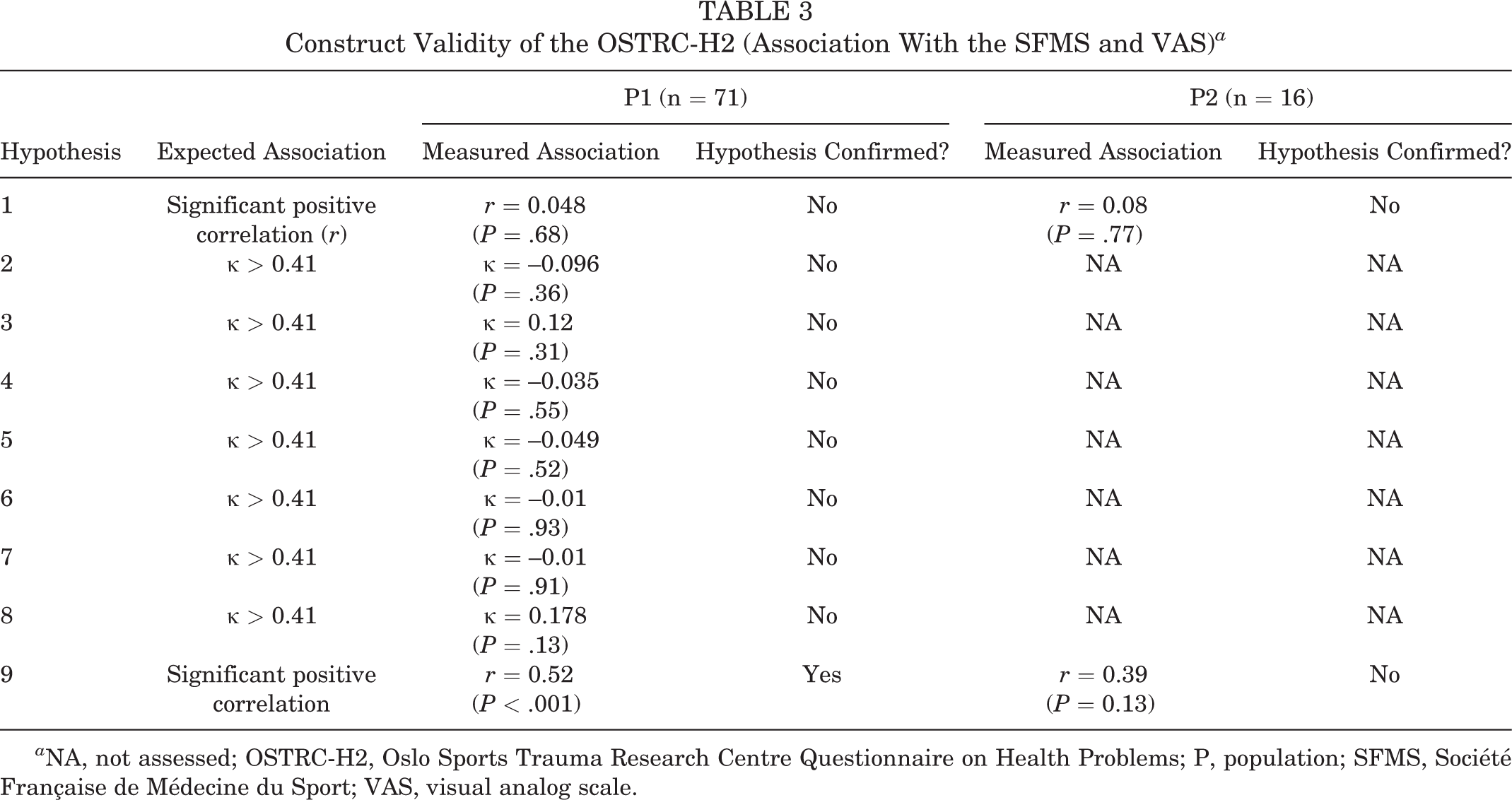
a NA, not assessed; OSTRC-H2, Oslo Sports Trauma Research Centre Questionnaire on Health Problems; P, population; SFMS, Société Française de Médecine du Sport; VAS, visual analog scale.
Internal Consistency
Internal consistency was excellent in the population of athletes who reported a health issue (n = 19; Cronbach α = .94). Removing 1 item at a time did not impact the reliability of the questionnaire. The internal consistency of the OSTRC-H2 was equal to .97 for the entire cohort of participants (N = 80) (Table 4). All individual items demonstrated a strong, positive, and significant correlation with the total score of the OSTRC-H2 (all correlation coefficients, r ≥ 0.7; data not shown).
Test-Retest Reliability and Internal Consistency of the OSTRC-H2 a

a ICC, intraclass coefficient correlation; OSTRC-H2, Oslo Sports Trauma Research Centre Questionnaire on Health Problems; P, population.
Test-Retest Reliability
A strong test-retest reliability was observed for both populations, with an ICC value of 0.85 (95% CI, 0.77-0.90) for P1 (n = 80) and 0.90 (95% CI, 0.68-0.98) for P2 (n = 19), respectively (Table 4).
Ceiling Effects
Only 3 participants (3.75%) obtained a maximum score of 100, and thus no ceiling effects were found.
Discussion
The primary aim of this study was to translate the OSTRC-H2 questionnaire designed to register health problems for athletes from English into French. In this study, translations and back-translations were conducted without any major problems. The OSTRC-H2 showed very good test-retest reliability when including the entire population (ICC, 0.85 [95% CI, 0.77-0.90]) and when restricting the population to athletes reporting a health issue during the follow-up period (ICC, 0.90 [95% CI, 0.68-0.98]). Internal consistency was very good (Cronbach α = .94). The OSTRC-H2 demonstrated high concordance with the VAS of symptom intensity (r = 0.52; P < .05) and low concordance with the SFMS overtraining questions (κ from –0.01 to 0.12 according to hypotheses, all P > .05).
The psychometric performances of the French OSTRC-H2 were tested on a sample of 80 elite athletes. According to Terwee et al, 16 a minimum number of 50 participants should be included in any validation analysis of questionnaires. By including 80 elite athletes in our study, we believed to have enough power to evaluate psychometric properties. The mean number of participants included in other studies that have validated the OSTRC questionnaire (either OSTRC-O or OSTRC-H version 1 or 2) 2,5,8,10,11,14 was approximately 95 (range, 24-313) and the mean follow-up time across other studies that validated the OSTRC questionnaire was 12 weeks, which is concordant with our study.
The response rate throughout the study period was higher than in previous questionnaire adaptation and validation studies. This may be explained by the daily reminders that were sent to participants via the platform. Indeed, in German, 9 Danish, 8 and Japanese 14 studies, only 1 single reminder was sent. Regarding the acceptability of the questionnaire, the athletes perceived the questionnaire as relevant, quick, and easy to complete.
To examine the reliability, we calculated the internal consistency as measured by the Cronbach alpha. The Cronbach alpha was .94 for the sample of participants who reported a health problem (n = 19). Looking at the whole population, we found a Cronbach alpha of .97, which is considered too high and may indicate redundancies between items. This later result is unsurprising because most of the population (ie, 76%) did not report any health problems during the study. If the athlete chooses response “a” for question 1 (ie, “complete participation without any health problems”), a total score of 0 was attributed, automatically ending the questionnaire. It is therefore logical that the internal consistency is impacted by this. In the Spanish translation 2 of the OSTRC-H2, authors also demonstrated a higher internal consistency among the entire population than among subgroups, including participants who reported health issues. 2 Globally, the internal consistency results found in our study are comparable with the original version 6 (ie, Cronbach alpha = .96) and other translations (ie, Cronbach alpha of .92, .90, and .96 for the German, 9 Danish, 8 and Japanese 14 translations, respectively). Another measure of reliability is the test-retest reliability. We chose a very short time between the test and the retest (ie, 24 hours, with a range of 24-72 hours accepted) to avoid any health changes between the first and second administration. Moreover, because this questionnaire refers to health issues occurring the week before the completion of the questionnaire, it is assumed that a longer time frame could negatively influence the results of the second administration, presenting lower reliability. The same methodology has also been selected by most of the translators of the OSTRC questionnaires for similar reasons. However, since the OSTRC-H2 questionnaire is composed of 4 questions, we could not exclude a recall bias. This is the reason the translators of the Japanese version of the OSTRC-H2 questionnaire 14 deliberately chose not to assess the test-retest reliability of the questionnaire. Nevertheless, in our study, very good values of test-retest reliability were found (ie, ICC, 0.85 [95% CI, 0.77-0.90]), as reported in the Spanish 2 version (ICC, 0.87 [95% CI, 0.79-0.92]).
Validity was investigated through construct validity. It could have been possible to evaluate the criterion-related validity of the questionnaire by performing a medical diagnosis of injuries for each participant. However, the process of data collection did not allow us to perform such evaluations. Only 1 of our 9 pre-hypotheses was confirmed. However, we believe that this is mainly because of a methodological choice made regarding the questionnaire used for measuring the construct validity. Questionnaires other than the SFMS could have been more appropriate, but to the best of our knowledge, no questionnaire measuring a similar construct to the OSTRC-H2 was available and validated in French. We were therefore confronted with an issue regarding the availability of questionnaires in other languages. Because the construct validity of the OSTRC-H questionnaire has already been validated in other cohorts, we nevertheless believe that the OSTRC-H2 is a valid tool to properly measure the occurrence of health problems in athletes.
Limitations
Some limitations of this work should be considered. First, as already mentioned, the validity results should be considered with caution because of the lack of other similar and recognized instruments to evaluate the construct of interest. Second, a reporting bias may be possible in such a study. Athletes might not have reported a health issue due to forgetfulness or voluntarily for a number of reasons, such as depression, anxiety, et cetera, or because they were used to a condition and failed to recognize it as a health issue. Also, we observed a decrease in the prevalence of health issues reported during the follow-up, the reason for which has not been studied. It could be hypothesized that students who participated in this study decreased their training frequency and, as a result, the incidence of related health issues decreased during the months leading to their examinations. Third, only elite athletes were included in this study, and the validity of the questionnaire in other groups, including amateur athletes and children, is still unknown. Finally, we did not focus on a specific sport but did not study all possible sports either. Therefore, we cannot ensure that the French version of the OSTRC-H2 can be used to record all health problems in high-performance athletes in different sports. Future studies could focus on measuring the prevalence of health problems in a targeted population to analyze sport-specific risk factors.
Conclusion
Study findings indicated that the translated version of the OSTRC-H2 was valid and reliable when applied to French-speaking elite athletes.
Supplemental material for this article is available at https://journals.sagepub.com/doi/full/10.1177/23259671231173374#supplementary-materials.
Supplemental Material
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671231173374 - French Translation and Validation of the OSTRC-H2 Questionnaire on Overuse Injuries and Health Problems in Elite Athletes
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671231173374 for French Translation and Validation of the OSTRC-H2 Questionnaire on Overuse Injuries and Health Problems in Elite Athletes by Charlotte Beaudart, Margaux Galvanin, Rosalie Hauspy, Benjamin Matthew Clarsen, Christophe Demoulin, Stephen Bornheim, Julien Van Beveren and Jean-François Kaux in Orthopaedic Journal of Sports Medicine
Footnotes
Acknowledgment
The authors thank all the athletes for their participation and AthleteMonitoring for providing free access to their platform for this study.
Final revision submitted January 24, 2023; accepted February 22, 2023.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
The present study was approved by the Ethics Committee of the University of Liège (ref 2020/390).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.