
Abstract
Background:
Medial opening-wedge high tibial osteotomy (MOWHTO) reduces contact stress by altering the weightbearing axis from the medial to the lateral compartment, relieves knee pain, and slows the progression of osteoarthritis.
Purpose/Hypothesis:
To evaluate whether the volume of the medial meniscus affects outcomes after MOWHTO. It was hypothesized that reduced medial meniscal volume would be associated with worse midterm clinical and radiographic outcomes.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Included were 59 patients who underwent MOWHTO and had ≥4 years of follow-up data. The mean follow-up period was 66.5 ± 15.1 months (range, 48-110 months). The cohort was classified into 3 groups according to the status of the medial meniscus on arthroscopic examination before osteotomy: no meniscal tear, degenerative tear leading to partial meniscectomy, and degenerative tear leading to subtotal meniscectomy. The Hospital for Special Surgery score and Knee Society objective and functional scores were compared among the groups at 2 time points (preoperative and latest follow-up), and the medial joint space width (JSW) was compared among the groups at 3 time points (preoperative, 1 year postoperative, and latest follow-up).
Results:
Overall, 9 patients had no meniscal tear, 20 patients underwent partial meniscectomy, and 30 patients underwent subtotal meniscectomy. The clinical scores improved significantly from preoperatively to the latest follow-up (P ≤ .001 for all), with no significant difference among the groups. Post hoc analysis indicated that at the latest follow-up, JSW was significantly lower in the subtotal meniscectomy group compared with the no-tear group on both 45° of flexion posterior-anterior (2.5 ± 1.3 vs 3.9 ± 1.8 mm; P = .004) and anterior-posterior (3.4 ± 1.1 vs 4.5 ± 0.9 mm; P = .011) radiographs.
Conclusion:
Subtotal meniscectomy of the medial meniscus performed during arthroscopic examination with MOWHTO was associated with decreased JSW at midterm follow-up. Efforts should be made to preserve the medial meniscus as much as possible during MOWHTO.
The medial meniscus plays a crucial role in shock absorption, load distribution to minimize excessive contact pressure, and knee joint stabilization to protect articular cartilage. 4,28 The association between meniscal resection and progression of osteoarthritis (OA), first noted by Fairbank 7 in 1948, has become widely known. 20 In 2004, Englund and Lohmander 5 reported that meniscal loss was a risk factor for degenerative changes in the knee joint and indicated that patients undergoing partial meniscectomy have a lower risk of OA than those undergoing subtotal or total meniscectomy.
Medial opening-wedge high tibial osteotomy (MOWHTO) is a viable surgical option for the treatment of medial compartment OA with varus deformity. 9,11,21 It reduces contact stress by altering the weightbearing axis from the medial to the lateral compartment, relieves knee pain, promotes healing of the injured medial femoral or tibial condylar cartilage, and slows the progression of OA. 19,23,24 Although studies have analyzed the relationship between medial meniscal extrusion or posterior root tear and MOWHTO outcomes, 12,17 it is not clear which is greater, the effect of meniscal resection on exacerbating OA or the effect of MOWHTO on preventing OA.
In this study, we evaluated whether the role of MOWHTO in reducing pain and preventing OA progression is affected by the volume of the medial meniscus. We hypothesized that reduced medial meniscal volume would be associated with worse midterm clinical and radiographic results after MOWHTO.
Methods
This retrospective study was conducted after obtaining of institutional review board approval from our institution. Between December 2009 and May 2016, 119 patients underwent MOWHTO performed by a single surgeon (S.-I.B.). The indications for MOWHTO were an active lifestyle with symptomatic medial compartment OA with varus alignment of the affected lower limb on standing hip-knee-ankle (HKA) radiographs and an intact lateral compartment despite nonoperative treatment for >3 months. In all patients, the severity of varus deformity was evaluated on standing hip-to-ankle radiographs. All patients had Ahlbäck grade <3 medial OA that had not advanced to the lateral compartment, as confirmed by radiography and magnetic resonance imaging (MRI). 1 The contraindications for MOWHTO were Ahlbäck grade ≥3 medial compartment arthritis, active inflammatory arthritis, lateral compartment arthritis, severe patellofemoral arthritis, or a flexion contracture >10°.
The study inclusion criteria were as follows: (1) primary MOWHTO using locking plate fixation (Tomofix, DePuy Synthes, or Synthes), (2) postoperative follow-up >4 years, and (3) medial meniscal status according to arthroscopic examination. The exclusion criteria were as follows: (1) revision surgery (n = 3), (2) combined cruciate ligament reconstruction (n = 9), (3) combined medial meniscal allograft transplantation (n = 2), insufficient follow-up duration (n = 35), and without arthroscopic examination before osteotomy (n = 11). Thus, 59 of the 119 patients were enrolled in the study.
Surgical Technique and Rehabilitation
All surgical procedures were performed by a single senior surgeon (S.I.B.). The target correction angle was assessed on a standing hip-to-ankle radiograph with the patella facing forward, according to the method described by Miniaci et al. 22 The target weightbearing line (WBL) that crossed the knee joint from the center of the hip to the center of the ankle was determined at approximately 62.5% from the medial border, along the width of the tibia plateau, and modified according to the intra-articular compartment status. 14,27 In all patients, the intra-articular compartment status was evaluated during preoperative physical examination and MRI and was confirmed during a concomitant arthroscopic examination before osteotomy. If a degenerative tear was present in the meniscus and causing symptoms, the patient underwent partial or subtotal meniscectomy. Repair was not attempted because the tear in the medial meniscus was attributed to degenerative changes. After the arthroscopic procedure was completed, the medial meniscal status was reevaluated and the femoral and tibial articular cartilage was assessed using the International Cartilage Regeneration & Joint Preservation Society scale. 13
For the MOHWTO, an anterior-medial longitudinal skin incision was created from the superior-medial aspect of the inferior patellar pole to 4 to 5 cm below the tibial tubercle. Before biplanar osteotomy, the semitendinosus and gracilis tendons were partially detached, and the superficial medial collateral ligament was released distally below the osteotomy level. The osteotomy proceeded until an intact lateral hinge located approximately 9 mm from the lateral cortex. The posterior neurovascular structures were protected using a blunt retractor. The proximal tibial osteotomy site was opened using a lamina spreader, and fixation was achieved using TomoFix (DePuy Synthes or Synthes). On the day after surgery, the patients began continuous passive motion exercises. Weightbearing was gradually introduced, from toe touching during the first 2 weeks to full weightbearing at 6 to 8 weeks postoperatively. Postoperative rehabilitation was continued for 3 months, focusing on attaining full range of motion and strengthening the quadriceps.
Medial Meniscal Volume Evaluation and Study Design
The findings of the arthroscopic examination before MOWHTO were recorded in a preformatted electronic database. 16 Medial meniscal volume was based on the width of the most reduced portion of the meniscus. For data analysis, the patients were divided into 3 groups according to the medial meniscal status: (1) no meniscal tear group, for which no procedure was implemented during arthroscopic examination; (2) partial meniscectomy group, in whom the medial meniscal width was ≥3 mm owing to partial maceration before surgery or partial meniscectomy during arthroscopic examination; and (3) subtotal meniscectomy group, in whom the medial meniscal width was <3 mm owing to subtotal or total maceration before surgery or subtotal or total meniscectomy during arthroscopic examination.
MOWHTO Outcome Evaluation
Patient characteristics (age, sex, body mass index), HKA angle before and after surgery, and cartilage status at arthroscopic examination were assessed for each group. The clinical outcomes were evaluated with the Hospital for Special Surgery (HSS) score, the Knee Society (KS) objective and functional scores, and medial joint space width (JSW). The HSS and KS were administered preoperatively and at every annual follow-up after surgery. 27
The medial JSW was measured on standing 45° of flexion posterior-anterior (PA) and anterior-posterior (AP) radiographs. The width between the femoral condyle and tibial plateau was measured at the center of the medial compartment. To minimize measurement error, images were acquired according to a standardized protocol. 8,18 The digital caliper in the picture archiving and communication system (PetaVision3D) was used. The WBL ratio was calculated as the ratio between the tibial plateau width and the medial tibial intersection of the line, with the medial tibial edge at 0% and the lateral tibial edge at 100%; it was assessed at 3 time points.
To verify data reliability, the JSW and WBL ratio was measured independently by 2 experienced orthopaedic surgeons (J.-H.S. and H.-K.C.) twice within a period of 2 weeks, and intraobserver and interobserver agreement was calculated.
Statistical Analysis
Patient characteristics, HKA angle, and cartilage status were compared among the no meniscal tear, partial meniscectomy, and subtotal meniscectomy groups. The HSS and KS scores were compared among the groups at 2 time points (preoperative and latest follow-up) and the medial JSW was compared at 3 time points (preoperative, 1 year postoperative, and latest follow-up). All statistical analyses were performed using SPSS Version 21.0 (IBM). The Kruskal-Wallis test was used for continuous variables and the Fisher exact test for categorical variables. Post hoc Mann Whitney tests were used for pairwise comparisons when the Kruskal-Wallis test was significant. Statistical significance was defined as P < .05, and post hoc pairwise comparisons were adjusted using Bonferroni correction (significance level, P < .016). Intraobserver and interobserver agreement was evaluated using the intraclass correlation coefficient (ICC), with ICC values categorized as good (>0.75), fair (0.4-0.75), or poor (<0.4).
Results
The mean follow-up period among the 59 study patients was 66.5 ± 15.1 months (range, 48-110 months). There were 9 patients in the no meniscal tear group, 20 patients in the partial meniscectomy group, and 30 patients in the subtotal meniscectomy group. Table 1 summarizes the characteristics of each group. There was a significant difference in age between the no tear group and the subtotal meniscectomy group on pairwise comparison post hoc analysis using Bonferroni correction (P < .016).
Patient Characteristics According to Medial Meniscal Status During MOWHTO a
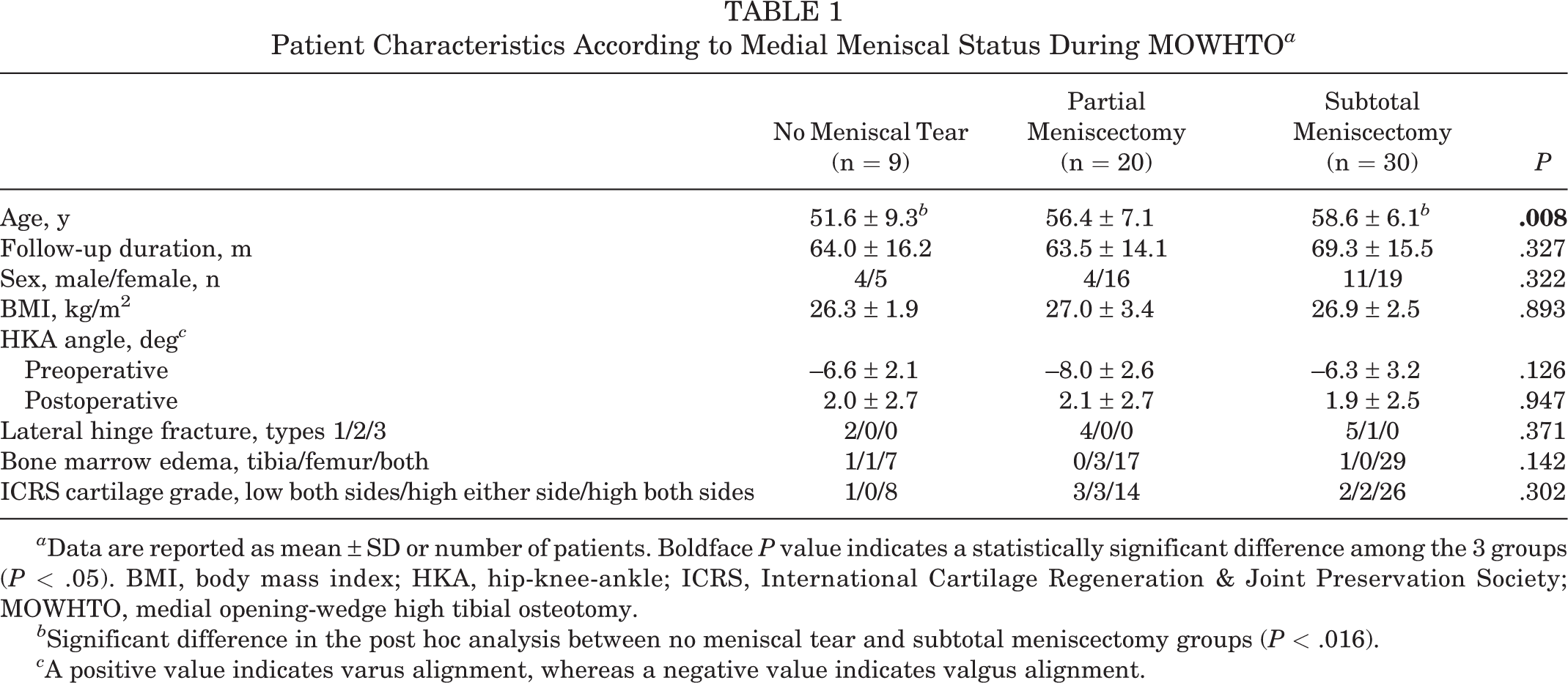
a Data are reported as mean ± SD or number of patients. Boldface P value indicates a statistically significant difference among the 3 groups (P < .05). BMI, body mass index; HKA, hip-knee-ankle; ICRS, International Cartilage Regeneration & Joint Preservation Society; MOWHTO, medial opening-wedge high tibial osteotomy.
b Significant difference in the post hoc analysis between no meniscal tear and subtotal meniscectomy groups (P < .016).
c A positive value indicates varus alignment, whereas a negative value indicates valgus alignment.
Clinical and Radiographic Results
Clinical and radiographic results are presented in Table 2. Overall, the clinical scores improved significantly from preoperatively to latest follow-up (HSS score: from 73.5 ± 9.7 to 89.1 ± 8.8 [P < .001]; KS objective score: from 79.0 ± 8.2 to 90.7 ± 10.4 [P = .001]; KS functional score: from 68.3 ± 11.2 to 83.8 ± 13.2 [P < .001]). There were no significant differences in clinical findings among the 3 groups at latest follow-up.
Midterm Clinical and Radiographic Results of the Groups According to the Medial Meniscal Status in Arthroscopic Examination During MOWHTO a

a Data are reported as mean ± SD. Boldface P values indicate a statistically significant difference among the 3 groups (P < .05). HSS, Hospital for Special Surgery score; JSW, joint space width; KS; Knee Society score; MOWHTO, medial opening-wedge high tibial osteotomy; WBL, weightbearing line.
b Significant difference in the post hoc analysis (P < .016) between the no meniscal tear and subtotal meniscectomy groups.
The interobserver agreement was 0.897 for JSW on 45° of flexion PA radiograph, 0.876 for JSW on AP radiograph, and 0.882 for WBL ratio, and the intraobserver agreement was 0.916 for JSW of 45° of flexion PA radiograph, 0.920 for JSW of AP radiograph, and 0.895 for WBL ratio. Agreement was found to be good.
There was a significant difference among groups in medial JSW on 45° of flexion PA radiograph at both the 1-year (P = .042) and latest (P = .010) follow-ups (Table 2 and Figure 1A). In post hoc analysis using Bonferroni correction, significant differences were observed between the no tear and subtotal meniscectomy groups only at the latest follow-up (3.9 ± 1.8 vs 2.5 ± 1.3 mm, respectively; P = .004). There was a significant difference among groups in the medial JSW on AP radiograph at the latest follow-up (Table 2 and Figure 1B); post hoc analysis found the difference between the no tear and subtotal meniscectomy groups to be significant (4.5 ± 0.9 vs 3.4 ± 1.1 mm, respectively; P = .011).
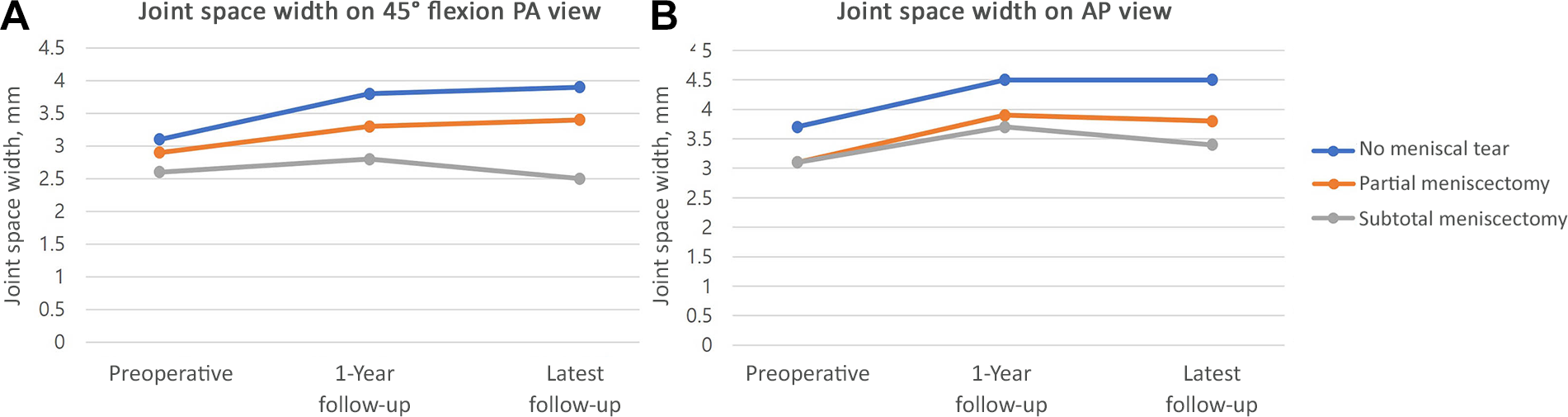
Changes over time according to the medial meniscal group in medial joint space width: (A) 45° of flexion posterior-anterior (PA) view and (B) anterior-posterior (AP) view.
Discussion
An important finding of this study is that clinical scores at midterm follow-up after MOWHTO were improved regardless of medial meniscal status; however, the JSW was significantly lower in patients who underwent subtotal meniscectomy with MOWHTO versus patients with no meniscal tear, on both 45° of flexion PA radiograph (P = .004) and AP radiograph (P = .011). This finding implies that the progression of OA in MOWHTO can be associated with reduced medial meniscal volume. Thus, effort should be made to preserve the medial meniscus as much as possible during MOWHTO.
MOWHTO is performed on symptomatic knee medial compartment OA patients and showed significant improvement in postoperative clinical outcome. This was also observed in studies with a long follow-up period. Lee et al 15 reported that midterm clinical scores showed improvement regardless of the degree of OA. In a study by Song et al, 26 improvement of clinical score was observed in patients who underwent MOWHTO regardless of the lateral hinge fracture. As such, the effect of improving the symptoms of MOWHTO has been proven. On the other hand, whether meniscal tears in patients with OA affect the clinical results is still controversial. 2,12,17 Englund et al 6 found no relationship between meniscal injuries demonstrated on MRI and subjective symptoms reported by patients with OA. Kamimura et al 10 demonstrated a relationship between the type of medial meniscal tear and characteristic clinical symptoms reported by patients with medial knee OA.
MOWHTO shifts the weight load axis into the lateral compartment to improve load distribution, thus slowing the progression of medial compartment OA. 9,11 Birmingham et al 3 evaluated the effect of MOWHTO on radiographic outcomes over a 2-year postoperative period in patients with varus alignment and medial compartment OA. The mechanical axis angle was well-maintained for 2 years after surgical correction, and the medial JSW slightly increased after 2 years compared with that before surgery. Sawaguchi et al 25 evaluated the outcomes between individuals undergoing MOWHTO and nonoperative care or no treatment. Radiographic evaluation revealed that unlike the significant decrease in the JSW in the nonoperative care group, in the HTO group the JSW was relatively stable, with a mean decrease of 0.11 mm from baseline to the 2-year postoperative period.
On the other hand, when the medial meniscal volume was reduced, knee OA was further progressed. Fairbank 7 announced that joint destruction proceeded owing to loss of weightbearing function of the meniscus after meniscectomy. Englund and Lohmander 5 reported that at mid- to long-term follow-up after meniscectomy, 27% of patients who had prior meniscal surgery developed symptomatic radiographic tibiofemoral OA. In the current study, we found that subtotal meniscectomy of the medial meniscus was associated with decreased joint space at midterm follow-up after MOWHTO. It was confirmed that saving the meniscus can be equally applied when HTO is performed.
Limitations
Some limitations to this study should be noted. First, the statistical power of this study is reduced because the number of patients enrolled in the no meniscal tear group was small, and the number of patients in each group was not uniform. However, this was because of the characteristics of patients who underwent HTO, and it was difficult to arbitrarily increase the number of patients because it was a retrospective study. We attempted to supplement this through nonparametric analysis, but our attempt was insufficient. It is believed that further study on large-scale patients is needed. Second, among the preoperative patient factors, age showed a statistically significant difference in the comparison among the groups. The reason for this is not clear. However, other factors such as body mass index and cartilage status, which can affect research results other than age, do not show statistical significance. Also, there have been no previous studies showing that age is associated with OA progression, a JSW reduction. Therefore, it is not judged that this would have had a significant impact on the results of the study. Third, although the comparison of medial JSW between the 3 groups before surgery was not statistically significant, it was observed that the smaller the meniscal volume, the smaller the JSW. This indicates that caution is needed to interpret the results of this study.
Conclusion
Subtotal meniscectomy of the medial meniscus performed during arthroscopic examination with MOWHTO was associated with decreased joint space at midterm follow-up. Efforts should be made to preserve the medial meniscus as much as possible during MOWHTO.
Footnotes
Final revision submitted December 12, 2022; accepted January 24, 2023.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Asan Medical Center (reference No. 2021-0314).