
Abstract
Background:
Psychological distress after orthopaedic surgery can lead to worse outcomes, including higher levels of disability and pain and lower quality of life. The 10-item Optimal Screening for Prediction for Referral and Outcome–Yellow Flag (OSPRO-YF) survey screens for multiple psychological constructs relevant to recovery from orthopaedic injury and may be useful to preoperatively identify patients who may require further psychological assessment and possible intervention after surgery.
Purpose/Hypothesis:
To determine the association between the OSPRO-YF and physiological patient-reported outcomes (PROs). It was hypothesized that higher OSPRO-YF scores (indicating worse psychological distress) would be associated with worse PRO scores at time of return to sport.
Study Design:
Case series; Level of evidence, 4.
Methods:
This study evaluated 107 patients at a single, academic health center who were assessed at a sports orthopaedics clinic and ultimately treated surgically for injuries to the knee, shoulder, foot, or ankle. Preoperatively, patients completed the OSPRO-YF survey as well as the following PRO measures: Patient-Reported Outcomes Measurement Information System (PROMIS), Single Assessment Numeric Evaluation, numeric rating scale for pain; American Shoulder and Elbow Surgeons standardized shoulder assessment form for patients with shoulder injuries, the International Knee Documentation Committee score (for patients with knee injuries), and the Foot and Ankle Ability Measure (FAAM; for patients with foot or ankle injuries). At the time of anticipated full recovery and/or return to sport, patients again completed the same PRO surveys. Multivariable regression was used to evaluate the association between total OSPRO-YF score at baseline and PRO scores at the time of functional recovery.
Results:
The baseline OSPRO-YF score predicted postoperative PROMIS Physical Function and FAAM Sports scores only. A 1-unit increase in the OSPRO-YF was associated with a 0.55-point reduction in PROMIS Physical Function (95% CI, –1.05 to –0.04; P = .033) indicating worse outcomes. Among patients who underwent ankle surgery, a 1-unit increase in OSPRO-YF was associated with a 6.45-point reduction in FAAM Sports (95% CI, –12.0 to –0.87; P = .023).
Conclusion:
The study findings demonstrated that the OSPRO-YF survey predicts certain long-term PRO scores at the time of expected return to sport, independent of baseline scores.
Psychological distress presents a significant barrier to patient recovery and return to baseline function after orthopaedic injury. Clinically significant levels of psychological distress including anxiety and depression have been noted in up to 50% of patients who have experienced a traumatic orthopaedic injury. 1,50 Psychological distress can affect rehabilitation after injury, lowering quality of life and prolonging recovery. 15,39 Certain specific baseline psychological characteristics can directly impair recovery from orthopaedic injury. Lower self-efficacy surrounding injury, higher anxiety regarding pain, pain catastrophizing, and higher levels of depression have all been linked to worse outcomes after definitive surgical repair. 1,41,44,48,49 Perseverance of pain results in lower quality of life and patient satisfaction scores, despite technically successful surgical correction of orthopaedic injuries. 7,37,38 In addition, high pain catastrophizing is associated with reduced response to physical therapy, with reported pain scores above the clinical threshold despite effective physical therapy treatment, 44 as well as increased pain medication consumption postoperatively. 46 Despite this, there is currently limited literature investigating the utility of psychological screening within the general sports orthopaedics population, outside of those undergoing anterior cruciate ligament (ACL) reconstruction. 3,9,34
The use of concise screening tools can enable surgeons to quickly and accurately identify patients who may be more likely to experience poor surgical outcomes due to psychological distress. There are a number of tools that have been utilized in orthopaedic populations, including the Brief Symptom Inventory (BSI), 6 the Distress and Risk Assessment Method Questionnaire, 30 and the Four-Dimensional Symptom Questionnaire (4DSQ). 21 However, each of these tools is >40 questions long, which may limit patient responses and impede clinic flow. Other measures such as the Pain Catastrophizing Scale (PCS), 47 Tampa Scale for Kinesiophobia (TSK-11), 22 and Patient Health Questionnaire (PHQ-9) 45 are more common to orthopaedists, but they only capture single dimensions of psychological distress. The 10-item Optimal Screening for Prediction for Referral and Outcome–Yellow Flag (OSPRO-YF) assessment tool is a multidimensional psychological screening questionnaire that identifies patients at increased risk of psychological burden after injury. OSPRO-YF evaluates multiple psychiatric domains related to negative mood, poor pain coping, and low self-efficacy/pain acceptance. 8,24 Higher OSPRO-YF counts have been shown to predict long-term patient responses to rehabilitation for musculoskeletal pain. 5,16,25,26 However, no studies have yet investigated the utility of OSPRO-YF screening within a sports orthopaedics population, which typically consists of younger and more active individuals than the general population seeking rehabilitation for musculoskeletal pain. Furthermore, no studies have examined whether OSPRO-YF predicts postoperative functional outcomes for sports-related pathologies.
In this study, we evaluated the ability of the OSPRO-YF screening tool to predict postoperative patient-reported outcomes (PROs) within an orthopaedic sports population. We hypothesized that patients with higher baseline OSPRO-YF counts would report lower overall function and higher pain scores at the time of return to sport.
Methods
Patient Selection
After receiving institutional review board approval for the study protocol, we conducted a retrospective review of patients who received surgical intervention for a sports-related injury between February 2021 and March 2022. Informed consent was not required as this was a retrospective records review of previously treated patients. The study population consisted of consecutive patients with sports-related pathologies of the knee, shoulder, ankle, or foot, who were treated within a single academic health system and underwent surgical treatment. Retrospective review of the electronic medical record was conducted. Patients were included if they had completed an OSPRO-YF questionnaire at initial evaluation, had undergone surgery, and had attended postoperative follow-up through the time of their expected full return to sport based on their pathology and surgery. Patients were excluded if they (1) received bilateral surgeries, (2) experienced any postoperative complications including superficial or deep surgical site infection and failure of the index surgery, (3) required a second surgery, or (4) had not yet completed the requisite pre- and postoperative PRO measures at the time of expected return to play.
All related surgeries were performed by a single fellowship-trained orthopaedic sports surgeon (B.C.L.). Physical therapy and rehabilitation followed standard evidence-based protocols at our institution and varied by pathology.
Primary Outcome Measure
We elected to evaluate outcomes at the time of expected return to play instead of a uniform time postoperatively across all pathologies. This was done in order to assess whether OSPRO-YF scores could predict function at a time point that is relevant for making clinical decisions regarding return to play.
We defined expected return to play as the time at which a patient could be expected to return to most sporting activity after sports-related knee, shoulder, ankle, or foot injury. The timing of expected return to play per surgery type (ie, the window for measuring and analyzing function) was as follows: for ACL reconstruction and ACL reconstruction + meniscal debridement, 9 ± 2 months; for meniscal debridement/meniscal surgery, 4 ± 1 months; for Achilles tendon repair, 6 ± 2 months; for metatarsal open reduction and internal fixation (ORIF), 5 ± 1 months; for labral or capsular repair, 6 ± 2 months; and for rotator cuff repair, 6 ± 2 months.
Data Collection
All data were collected retrospectively from our institution’s electronic health record database via MaestroCare (May 2022 Version; Epic Systems Corp). Patient descriptive variables including age at the time of surgery, sex, race and ethnicity, body mass index (BMI), and smoking status were collected in addition to injury information including surgery received and laterality. Patients completed the OSPRO-YF survey before their surgery as part of routine clinical care, either in the clinic on a tablet or online via the MaestroCare platform. In accordance with standard protocol, PRO scores were collected at the initial visit before surgery (baseline) and at each postoperative follow-up appointment.
Assessment of Psychological Distress
The predictor of interest in this analysis, the OSPRO-YF survey, assesses 11 psychological constructs within 3 broad psychological domains of self-efficacy and acceptance (pain self-efficacy, rehabilitation self-efficacy, and chronic pain acceptance), negative pain coping (fear avoidance beliefs surrounding work and physical activity, pain catastrophizing, kinesiophobia, and pain anxiety), and negative mood (depression, anxiety, and anger). Based on patient responses, OSPRO-YF generates a score estimate for each of the 11 constructs. Scores above the 75th percentile in negative pain coping or negative mood constructs or below the 25th percentile in self-efficacy/acceptance constructs are marked with a “yellow flag” for that construct, 8,16,24 and the summary OSPRO-YF score for a patient is a simple count of the number of constructs with yellow flags. The OSPRO-YF has been validated for predicting PROs, including pain intensity, disability, and quality of life for patients with musculoskeletal pain 12 months after injury. 16
PRO Measures
The following PRO measures were used in this study: Patient-Reported Outcomes Measurement Information System (PROMIS), Single Assessment Numeric Evaluation (SANE), numeric rating scale (NRS) for pain; American Shoulder and Elbow Surgeons (ASES) standardized shoulder assessment form for patients with shoulder injuries; International Knee Documentation Committee (IKDC) score for patients with knee injuries, and Foot and Ankle Ability Measure (FAAM) for those with foot or ankle injuries.
The PROMIS measures how patients conceptualize symptoms and function in their activities of daily living (ADLs). 43 PROMIS measures were developed using item-response theory, with computer-adaptive testing options that allow for accurate and reliable assessment using a minimal number of questions, reducing the questionnaire burden on patients. PROMIS scores generate T scores with a median of 50 and standard deviation of 10, in which a higher score indicates worse performance. Four PROMIS scores corresponding to 4 domains were collected: Physical Function, Pain Interference with ADLs, Sleep Disturbance, and Depression. For the SANE (range, 0-100), patients rated the functional level of the injured area in relation to its preinjury level, with higher scores indicating higher function. SANE accurately measures clinically significant improvements after surgical intervention of musculoskeletal pain. 18,51 For the NRS, the patient expressed one’s subjective pain experience as a value from 0 (no pain) to 10 (worst pain of my life). 14
The ASES (range, 0-100; lower scores indicate worse outcomes) consists of a self-reported series of ADLs that standardize physical function as it relates to the shoulder joint. 35 The IKDC (range, 0-100; lower scores indicate worse outcomes) evaluates domains of knee disability including symptoms, sports and ADL ability, and knee function compared with preinjury level. 10 The FAAM (range, 0-100; lower scores indicate worse outcomes) evaluates foot and ankle function as it relates to ADLs and ability to participate in sporting activities. Similar to the PROMIS, it utilizes item-response theory to characterize how ankle function contributes to a patient’s ability to perform various hypothetical scenarios. 31
Statistical Analysis
Data were recorded as means ± SDs for continuous variables and counts with percentages for nonmissing categorical variables. Pre- and postoperative PRO scores were compared using paired t tests, and mean differences with 95% CIs were calculated. Multivariable regression models were used to assess the relationship between baseline OSPRO-YF score and postoperative PRO scores. Models included baseline OSPRO-YF score as the primary predictor and were adjusted for injury, age, sex, race, BMI, and respective PRO baseline scores. To control for unique injury- or surgery-related characteristics, we included a categorical variable for surgery type in the model, with the following options: ACL reconstruction, ACL reconstruction + meniscal repair, meniscal repair/meniscectomy, Achilles tendon repair, metatarsal ORIF, labral or capsular repair, and rotator cuff repair. Patients who sustained a combined ACL and meniscal injury were included in the ACL group.
The normality of each outcome was assessed via graphical methods, including residual plots. PROMIS (Physical Function, Pain Interference, Sleep Disturbance, Depression), SANE, ASES, IKDC, and FAAM (ADL, Sports) were modeled with linear models, and least-squares mean differences with associated 95% CIs were calculated. NRS pain was modeled using a generalized linear model (negative binomial distribution), and the resulting geometric mean ratio and 95% CI was calculated. SAS Version 9.4 (SAS Institute) was used for all analyses, and P < .05 was considered statistically significant.
Results
Patient Characteristics and Surgery Data
Overall, 497 patients underwent surgery during the observation window, with 210 patients who achieved the requisite postoperative follow-up time (ie, typical return-to-sport clearance time frame) required to be included in the analysis. Of these patients, 107 patients had both preoperative OSPRO-YF and PRO scores and follow-up PRO scores and were included in the analysis. The analyzed cohort had a mean age of 44 ± 17.4 years, and slightly more than half were male (n = 52; 48.6%). A majority of patients were White (n = 71; 66.3%) and 92.5% were non-Hispanic. The mean BMI was 29.7 ± 6.8. Only 8 patients were smokers (Table 1).
Patient Characteristics and Surgery Data (N = 107 patients) a
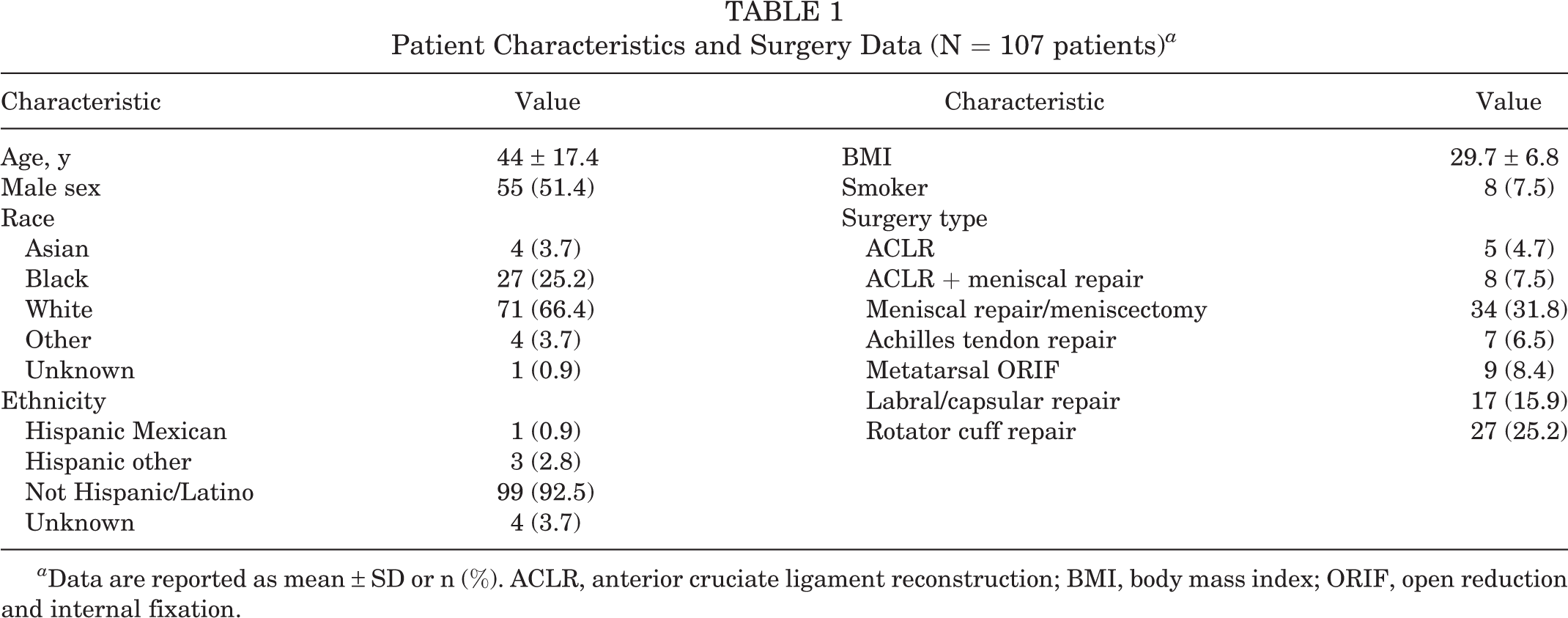
a Data are reported as mean ± SD or n (%). ACLR, anterior cruciate ligament reconstruction; BMI, body mass index; ORIF, open reduction and internal fixation.
Preoperative OSPRO-YF Score
A mean of 6.1 ± 3.7 yellow flags per patient were observed (Table 2). Constructs that most commonly had a yellow flag were chronic pain acceptance (n = 73; 68.2%), rehabilitation self-efficacy (n = 68; 63.6%), and pain anxiety (n = 66; 61.7%). Only 8 of the 107 patients (7.5%) had zero yellow flags at baseline.
OSPRO-YF Score and Distribution of Yellow Flags Across Constructs a
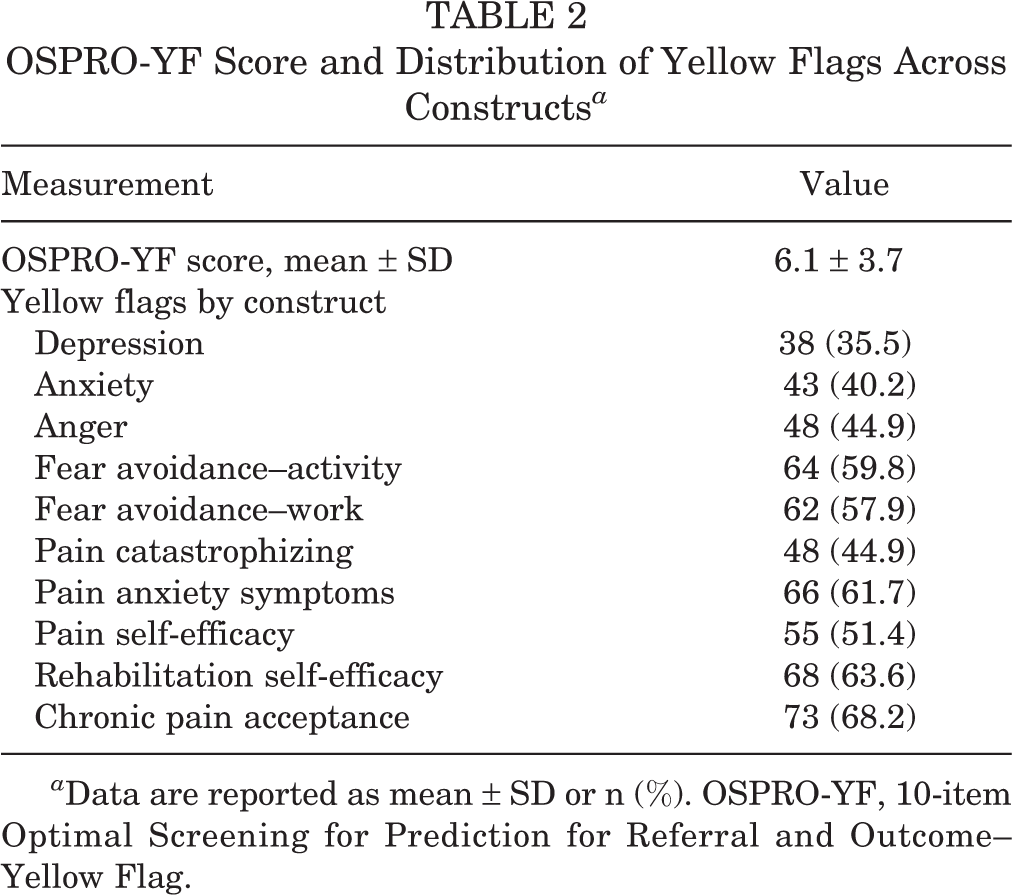
a Data are reported as mean ± SD or n (%). OSPRO-YF, 10-item Optimal Screening for Prediction for Referral and Outcome–Yellow Flag.
PRO Scores
Pre- and postoperative outcome scores are reported in Table 3. On average, patients improved on all PRO measurements from preoperatively to the time of expected return to sport. After controlling for baseline scores, age was associated with lower postoperative scores on PROMIS Physical Function (P = .017) as well as higher scores on PROMIS Pain Interference (P = .007). BMI was similarly associated with lower postoperative scores on PROMIS Physical Function (P = .001) as well as higher scores on PROMIS Pain Interference (P = .009). Of note, 63 (58.9%) patients reported no pain at the time of final follow-up.
Preoperative and Postoperative PRO Scores a

a ADL, Activities of Daily Living; ASES, American Shoulder and Elbow Surgeons standardized shoulder assessment score; FAAM, Foot and Ankle Ability Measure; IKDC, International Knee Documentation Committee score; NRS, numeric rating scale; PRO, patient-reported outcome; PROMIS, Patient-Reported Outcomes Measurement Information System; SANE, Single Assessment Numeric Evaluation score.
An increased OSPRO-YF score was found to be associated with worse PROMIS Physical Function score at time of expected return to play (least-squares mean difference, –0.55 [95% CI, –1.05 to –0.04]; P = .033). Among patients with ankle injuries, an increased OSPRO-YF score was associated with a lower FAAM Sports score at the time of expected return to play (least-squares mean difference, –6.45 [95% CI, –12.0 to –0.87]; P = .023) (Table 4).
Association of Increased OSPRO-YF Score With PRO Scores a

a Values are the association between a 1-unit increase in OSPRO-YF score and the resulting change in PRO score. Boldface P values indicate statistical significance (P < .05). ADL, Activities of Daily Living; ASES, American Shoulder and Elbow Surgeons standardized shoulder assessment form; FAAM, Foot and Ankle Ability Measure; IKDC, International Knee Documentation Committee score; NRS, numeric rating scale; OSPRO-YF, 10-item Optimal Screening for Prediction for Referral and Outcome–Yellow Flag; PROMIS, Patient-Reported Outcomes Measurement Information System; SANE, Single Assessment Numeric Evaluation score.
b Reported as least-squares mean difference (95% CI).
c Higher scores indicate worse outcomes.
d Reported as geometric mean ratio (95% CI).
Discussion
The study findings demonstrated that the OSPRO-YF survey predicts certain long-term PROs at the time of expected return to sport. This study is the first to both characterize baseline OSPRO-YF scores of this population and find markedly elevated psychological distress, with a mean of 6.1 flagged psychological domains per patient. This is also the first study to demonstrate an association between baseline OSPRO-YF scores and PRO scores at the time of expected functional recovery after surgery while accounting for other relevant covariates. A 1-unit increase in the OSPRO-YF was associated with a 0.55-point reduction in PROMIS Physical Function (95% CI, –1.05 to –0.04; P = .033) indicating worse physical function. Among patients who underwent ankle surgery, a 1-unit increase in OSPRO-YF was associated with a 6.45-point reduction in FAAM Sports (95% CI, –12.0 to –0.87; P = .023).
Accurately assessing patients at greater risk for psychological distress after orthopaedic injury is essential in order to better manage their expectations after surgical repair and potentially offer interventions to address pain-related psychological distress such as pain catastrophizing, fear avoidance, and anxiety. There are currently few studies exploring the utility of the OSPRO-YF screening tool in orthopaedics and none yet within a population of exclusively sports-related injuries requiring surgery. While there are a number of tools to measure psychological distress that have been validated within orthopaedics, they are generally lengthy and time-consuming to complete. For example, the BSI has 53 questions, the 4DSQ has 50 questions, and the Distress and Risk Assessment Methods Questionnaire has 45 questions. Measures such as the PCS, TSK-11, and PHQ-9 are shorter but measure only single psychological constructs, requiring multiple questionnaires to appropriately capture the full breadth of psychological needs. Routine use of these in the clinical setting has been limited, likely because of their high response burden; it is unreasonable to expect all new patients to complete these in the clinical setting without significantly slowing clinic flow. The OSPRO-YF is multidimensional and comparably quite brief (it can be completed in 2-3 minutes), reducing questionnaire fatigue from patients and making it easier to administer in a fast-paced sports clinic. 8
The study population had a markedly high incidence of yellow flags overall. Specifically, >60% of patients in the current cohort had a yellow flag for poor pain acceptance or low self-efficacy. Unfortunately, these constructs are well known to be associated with worse surgical outcomes. For example, scores of self-efficacy surrounding knee function are independently predictive of perceived knee function a year after surgery, with lower scores associated with lower Lysholm and Knee injury and Osteoarthritis Outcome Score–Sport and Recreation subscale scores. 49 In addition, lower self-efficacy was associated with higher pain and disability scores 2 years after total knee arthroplasty. 52 Pain acceptance is similarly related to postoperative outcomes. After posterior lumbar spinal fusion, patients with higher baseline pain acceptance had lower rates of disability and better physical and mental health. 12 A pilot study demonstrated that patients exposed to a trial of acceptance and commitment therapy showed higher levels of pain acceptance that correlated with lower disability rates and opioid use. 13 Taken together with the current paper, these results indicate that patients undergoing surgery for a sports-related injury may be predisposed toward subtypes of psychological distress known to impair recovery and rehabilitation.
In addition to characterizing the baseline psychological profile of this patient population, we found that within patients receiving ankle surgery, higher OSPRO-YF scores at baseline were associated with lower perceived function of that joint, although we were limited by the sample size of patients for the specific joint. A systemic review by Rosenberger et al 41 across a range of surgical procedures demonstrated that higher baseline scores of depression, anxiety, and preoperative stress were associated with worse patient perception of surgical outcomes including physical function. In patients who underwent ACL reconstruction, self-perceived lower physical function in the absence of difference in mechanical stability 1 year after surgery negatively predicted return to preinjury function. 3,4,19 The causal pathway between high psychological distress and poor postsurgical outcomes is not fully understood, but mediating factors may include lower participation in rehabilitation among those with high distress. 20 Norte et al 36 found that patients with a greater fear of pain after ACL reconstruction engaged in less physical activity, resulting in weaker hamstrings and subsequently lower KOOS-ADL scores. It is important to identify factors that may prevent a patient from engaging in the necessary rehabilitation after orthopaedic sports-related surgeries. Psychological distress is modifiable, and our study contributes important new information to better characterize which specific psychological characteristics are most prevalent in this population.
Identifying high psychological distress preoperatively is essential in order to offer effective intervention. Negative responses to pain can be improved with psychological and psychiatric interventions. 15,42 A scoping review by Gibson and Sabo 17 identified multiple interventions that can reduce psychological distress after surgery, including patient education, physical therapy, and cognitive-behavioral therapy. A similar review by Szeverenyi et al 48 further characterized the role of patient education preoperatively; simple patient education reduced psychological distress preoperatively along with postoperative pain and anxiety. Other interventions have targeted both the pre- and the postoperative period. An intervention that increased psychosocial support during rehabilitation from orthopaedic injury led to reduced incidence of a new psychiatric diagnosis and overall improved quality of life. 40 In a study of patients scheduled to undergo ACL surgery, Maddison et al 29 showed that watching a brief (9-minute) informational video preoperatively and again during the 2- to 6-week postoperative period led to increased function on IKDC subjective and objective scores and reduced overall crutch usage. This was partially explained by increased self-efficacy scores. In a similar cohort comprising patients who underwent ACL reconstruction, Cupal and Brewer 11 assigned a subset of patients to undergo 10 brief sessions of relaxation and guided imagery. These patients demonstrated greater knee strength and reported less pain and less reinjury anxiety than controls.
These studies demonstrate the utility of offering therapies in conjunction with surgery to better care for orthopaedic sports patients. However, orthopaedic providers cannot offer these therapies without first identifying patients who need them. A brief multidimensional screening tool such as the OSPRO-YF or the newly developed Screening for Pain vulnerability And Resilience measure for assessing fear avoidance and negative pain coping 27,28 can be administered in the clinic preoperatively to identify which patients may require psychological support.
We did not find a significant relationship between OSPRO-YF count and PROMIS Depression scores. This further validates OSPRO-YF as a tool that measures multiple psychological constructs and highlights that depression is not synonymous with overall pain-related distress. A higher total OSPRO-YF score indicates increased levels of distress across multiple psychological constructs, of which some may contribute to patient outcomes while others have less effect. We similarly found no relationship between OSPRO-YF score and the NRS pain score. This finding was surprising, as prior research has demonstrated that the constructs measured in the OSPRO-YF are associated with postoperative pain intensity 23,32,33,48 as well as perceived physical function. 2,20,23,41,48 Postoperative pain is a complex phenomenon with myriad contributing factors. The mean postoperative NRS pain score was low (1.4 of 10), and 58.9% of patients reported no pain. It is likely that we encountered floor effects that contributed to this finding.
Limitations
This study has several limitations. First, our cohort comprised multiple sports-related injuries and was relatively small because our selection of patients was treated by a single surgeon in order to reduce variability. As a result, this study was underpowered to investigate which specific yellow-flag constructs were associated with outcomes. Future studies of larger cohorts can investigate if some yellow-flag domains are more predictive than others. We were similarly underpowered to perform separate analyses by joint and pathology. A potential relationship between OSPRO-YF and joint-specific PRO scores such as the IKDC score for the knee or ASES standardized shoulder assessment form for the shoulder should be investigated. In addition, we did not collect information regarding level of sporting activity (recreational vs professional), type of sport, or mechanism of injury. Professional athletes may experience higher levels of psychological distress after an injury because it may directly affect their livelihood.
We excluded patients with bilateral surgeries as well, which may have biased our results. Similarly, we did not evaluate patients who received surgeries including bony work separately from those who underwent only soft tissue surgeries. Patients who underwent bony work, such as ACL repair graft harvesting for bone-to-bone grafts and tunneling, may experience more postoperative pain than patients who underwent exclusively soft tissue surgeries. Future research may evaluate differences in these groups. Finally, patients who received surgeries with a longer recovery time such as ACL repair were underrepresented in this cohort as they were not yet cleared for full return to sport. Given these limitations, our work should be considered exploratory in nature and hypothesis generating for larger studies, including those that would test interventions to reduce different types of psychological distress in this population.
Conclusion
The OSPRO-YF survey was an effective tool to preoperatively screen for patients at risk for lower PRO scores at the time of expected functional recovery, independent of baseline scores. Patients undergoing surgery for orthopaedic sports-related injury may experience higher levels of psychological distress than previously believed. Evaluation and treatment of psychological distress preoperatively and during rehabilitation are important considerations in the management of sports-related injury and surgery.
Footnotes
Final revision submitted December 14, 2022; accepted January 27, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.C.L. has received grant support from DJO and Zimmer Biomet, education payments from Smith & Nephew and Southtech Orthopedics, honoraria from Wright Medical, and hospitality payments from Crossroads Extremity Systems and Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Duke University Health System (reference No. Pro00110198).