
Abstract
Background:
Recent meta-analyses have advised against distal clavicle resection (DCR) as an adjuvant procedure during rotator cuff repair (RCR), whether performed routinely or in shoulders diagnosed with symptomatic acromioclavicular joint (ACJ) arthropathy. However, the efficacy of DCR as a secondary procedure in patients with persistent pain attributed to symptomatic ACJ arthropathy remains unknown.
Purpose:
To evaluate outcomes of secondary DCR in patients with failed nonoperative treatment of symptomatic ACJ arthropathy after isolated RCR with complete tendon healing.
Study Design:
Case series; Level of evidence, 4.
Methods:
Between 2008 and 2018, the senior surgeon performed isolated RCR in 1935 patients, of which 23 (1.2%) presented with ACJ pain and discomfort at ≥12 months after the index RCR, despite complete healing of repaired tendons. Those 23 patients underwent secondary DCR, as ACJ arthropathy was confirmed clinically and radiographically. Clinical assessment before DCR included the Subjective Shoulder Value (SSV) and pain at rest. Clinical assessment at >12 months after DCR included the SSV, pain at rest, Constant-Murley score, range of motion, and satisfaction. Pre- and post-DCR SSV and pain scores were compared.
Results:
Of the initial cohort, 5 patients did not consent to the use of their data, leaving 18 patients aged 53.3 ± 7.6 years (mean ± SD; range, 39-68 years) for outcome assessment. At a mean follow-up of 7.0 ± 3.1 years after DCR, the SSV significantly improved from 58.7 ± 17.2 to 76.1 ± 20.2 (P < .001), and the pain at rest significantly decreased from 4.7 ± 1.5 to 2.8 ± 1.9 (P < .001). At final follow-up, the Constant-Murley score was 70.2 ± 21.0. Of 18 patients, 15 had none or mild residual pain (0-2; 83%), while 3 had substantial residual pain (5 or 6; 17%). Only 1 of the 3 patients with substantial residual pain had a poor SSV score (20 points) and was against opting for DCR in retrospect. No patient had infections or gross ACJ instability after DCR.
Conclusion:
Secondary DCR for cases of symptomatic ACJ arthropathy after isolated RCR with complete tendon healing reduced pain in 83% of patients, and 94% were satisfied and would undergo secondary DCR again.
Keywords
Symptomatic acromioclavicular joint (ACJ) arthropathy can be challenging to diagnose and treat, as it is often concomitant with other shoulder pathologies, including rotator cuff tears, glenohumeral degeneration, and biceps or labral tears. 14 Symptomatic ACJ arthropathy has also been reported after rotator cuff repair (RCR), where inferiorly directed osteophytes can lead to impingement and pain, 15,16 though it is not always clear whether these conditions were present before surgery or whether they developed naturally or consequently thereafter.
Nonoperative treatment of symptomatic ACJ arthropathy includes physical therapy and corticosteroid injection, 11,12 though patients with persistent symptoms may require distal clavicle resection (DCR). 8,11,12 Routine DCR is not always recommended, however, as it can lead to complications such as pain, stiffness, instability, or infection. 2,4,7,9,13,15 Moreover, up to 90% of patients with asymptomatic ACJ arthropathy may remain pain-free at 7-year follow-up. 6 Recent meta-analyses 10,18 have advised against DCR as an adjuvant procedure during RCR, whether performed routinely or in shoulders diagnosed with symptomatic ACJ arthropathy. Yet, the efficacy of DCR as a secondary procedure in patients with persistent pain attributed to symptomatic ACJ arthropathy remains unknown.
The purpose of this study was to evaluate outcomes of secondary arthroscopic DCR in patients who had failed nonoperative treatment of symptomatic ACJ arthropathy after isolated RCR with complete tendon healing. The hypothesis was that at a minimum follow-up of 1 year, secondary arthroscopic DCR would provide adequate pain relief and shoulder function in most patients.
Methods
The study protocol received ethics committee approval, and all study patients provided informed consent for the use of their data for research. Between 2008 and 2018, the senior surgeon (A.G.) performed RCR in 2393 patients, of whom 458 had adjuvant DCR because they presented with clinical symptoms and radiographic evidence of ACJ arthropathy. The remaining 1935 patients underwent isolated RCR, as they had no radiological signs of ACJ arthropathy; among these, 23 (1.2%) presented to the clinic unsolicited for ACJ pain and functional impairment at minimum 12 months after index RCR, despite complete healing of repaired tendons, full shoulder range of motion, and functional recovery as it related to the rotator cuff. Of those 23 patients, palpation of the ACJ before RCR had led to pain in only 1 patient and to tenderness in 7 patients. In all patients, pain after RCR persisted despite ≥3 months of nonoperative treatment using NSAIDs, corticosteroid injections, and physical therapy.
The 23 patients were scheduled for secondary DCR, as ACJ arthropathy was confirmed by the presence of ≥3 of the following indications: severe pain upon palpation of the ACJ, positive cross-arm test result, positive ACJ shear test result, and positive resisted ACJ extension test result. For the last item, the patient’s shoulder was positioned in 90° of flexion and internal rotation, and the physical therapist placed his or her hand on the patient’s elbow and asked the patient to horizontally abduct the arm against isometric resistance; pain at the ACJ indicated a positive test result. 17 The 23 patients were also assessed using magnetic resonance imaging to rule out any retears or concomitant pathologies, such biceps or labral lesions or glenohumeral degeneration. None of the patients had undergone any surgical procedures on the ipsilateral shoulder before or after the index RCR.
Of the initial cohort of 23 patients, 5 were lost to follow-up, leaving 18 for outcome assessment (Figure 1).

Patient inclusion. ACJ, acromioclavicular joint; DCR, distal clavicle resection; RCR, rotator cuff repair.
Clinical Assessment
An orthopaedic surgery fellow (Y.B.) collected the clinical assessment immediately before DCR, which comprised the Subjective Shoulder Value (SSV) and pain at rest. At a minimum follow-up of 12 months after DCR, the SSV, pain at rest, and Constant-Murley scores were collected, as well as range of motion, including active forward elevation, external rotation with elbow at the side, and internal rotation. In addition, patients were asked to categorize their level of satisfaction with the procedure (disappointed, dissatisfied, satisfied, very satisfied) and to indicate whether they would opt for DCR in retrospect.
Surgical Technique
All patients underwent surgery in the beach-chair position under general anaesthesia with an interscalene block. A standard posterior portal was created, and the RCR and acromial decompression from the index procedure were inspected from intra-articular and subacromial views. In all shoulders, arthroscopic evaluation confirmed complete rotator cuff healing, as well as healthy humeral and glenoid cartilage, labrum, and, if present, long head of the biceps tendon. A needle was utilized to create an anterior and anterolateral portal using an outside-in technique, and through these portals a tissue ablation device (VAPR; DePuy Synthes) was used to expose the entire lateral aspect of the clavicle subperiosteally from the anterior capsule to the posterior capsule. Once the lateral clavicle was exposed and any impinging soft tissues were removed, resection of the distal clavicle was performed, removing 8 mm of bone from anterior to posterior using an oval bur (Stryker), taking care to create an even resection. The coracoclavicular and superior acromioclavicular ligaments were left intact. The arthroscope was then moved to the anterior and anterolateral portals to allow complete visualization of the posterior aspect of the distal clavicle and posterior capsule. A hooked probe was used to test the stability of the distal clavicle and confirm adequate resection. The portals were closed with nylon suture and standard dressings applied. No adjuvant procedures, such as acromioplasty or biceps tenotomy/tenodesis, were performed during DCR.
Postoperative Rehabilitation
All shoulders were immobilized, and patients used a sling for the first 10 days, while the regional block was effective, and began gentle postoperative therapy immediately after surgery, performing active assisted range of motion exercises. In the next 7 to 10 days, the goal was to recover full passive range of motion and improve to active movements to enable the patient to resume activities of daily living by the third postoperative month. No strength exercises were prescribed to the patient.
Statistical Analysis
Descriptive statistics were used to summarize the data. Normality of continuous variables was assessed through Shapiro-Wilk tests. For continuous variables, comparisons between groups were performed using Wilcoxon signed rank tests, as none of the variables were normally distributed. Univariable linear regression analyses were performed to determine associations of postoperative Constant-Murley score with 5 independent variables: sex, age, dominant side affected, time from RCR to DCR, and time from DCR to follow-up. P values <.05 were considered significant. Statistical analyses were performed using R Version 4.1 (R Foundation for Statistical Computing). Models were deemed sufficiently powered, considering the recommendations of Austin and Steyerberg 1 of 2 subjects per variable.
Results
The final cohort of 18 patients comprised 11 men (61%) and 7 women (39%) aged 53.3 ± 7.6 years (mean ± SD; range, 39-68 years) at secondary arthroscopic DCR, which was performed at 1.9 ± 1.1 years (range, 1.0-4.7 years) after the index RCR. No patient had infections or gross ACJ instability after DCR. The mean follow-up period was 7.0 ± 3.1 years (range, 1.3-11.2 years) after DCR (Table 1).
Clinical and Functional Data Before DCR and at Follow-up (N = 18) a

a Data are presented as mean ± SD (range) or No. (%). Dashes indicate areas not applicable. Bold P values indicate statistically significant difference from pre- to post-DCR. DCR, distal clavicle resection; GT, greater trochanter; RCR, rotator cuff repair; SSV, Subjective Shoulder Value.
At follow-up, 14 patients (77.8%) were very satisfied with DCR, 3 (16.7%) were satisfied, and 1 (5.6%) was dissatisfied; no patients were disappointed with the procedure (Table 2). Pain at rest significantly decreased from 4.7 ± 1.5 (range, 2-8) to 2.8 ± 1.9 (range, 1-7), and SSV significantly improved from 58.7 ± 17.2 (range, 30-90) to 76.1 ± 20.2 (range, 20-100) (P < .001 for both). At final follow-up, the Constant-Murley score was 70.2 ± 21.0; the range of active forward elevation was 160° ± 35.8°; the range of external rotation was 36.1° ± 16.4°; and internal rotation was functional in 14 patients (77.8%). Of 18 patients, 15 had none or mild residual pain (0-2; 83%), while 3 had substantial residual pain (5 or 6; 17%). Only 1 of the 3 patients with substantial residual pain had a poor SSV score (20 points) and was against opting for DCR in retrospect; this was a workers’ compensation case, and the patient never returned to work despite a statement of full recovery from the public health inspector.
Demographics and Clinical Assessment per Patient a

a AFE, active forward elevation; CM, Constant-Murley; DCR, distal clavicle resection; ER, external rotation with elbow at side; F, female; IR, internal rotation; L, left; M, male; NS, not satisfied; R, right; RCR, rotator cuff repair; ROM, range of motion; S, satisfied; SSV, Subjective Shoulder Value; VS, very satisfied;
b IR was classified as functional (L3, T12, T7/T8) or nonfunctional (sacrum, greater trochanter, buttock).
Univariable analysis revealed no significant associations between the independent variables and the postoperative Constant-Murley score (Table 3).
Results of Univariable Regression Analysis of Factors Associated With Postoperative Constant-Murley Score a
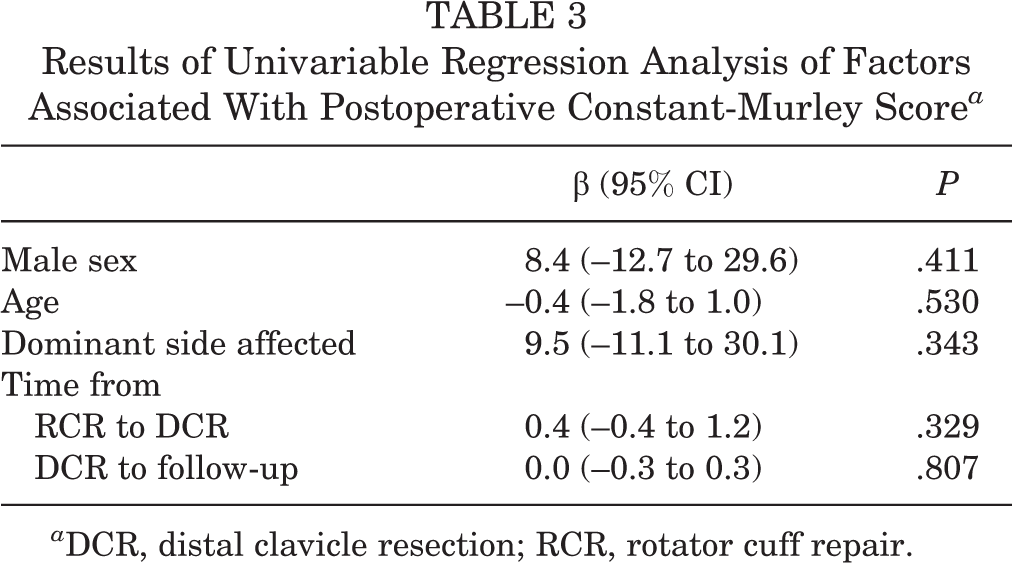
a DCR, distal clavicle resection; RCR, rotator cuff repair.
Discussion
The main finding of this study is that, at a mean follow-up of 7.0 years, secondary DCR for cases of symptomatic ACJ arthropathy after isolated RCR with complete tendon healing reduced pain in 83% of patients, though 94% were satisfied and would undergo secondary DCR again. The findings therefore support the hypothesis that secondary DCR can relieve pain in most patients with symptomatic ACJ arthropathy after isolated RCR with complete tendon healing whose nonoperative management failed. The findings are not surprising, however, as residual pain is common after RCR, which does not always restore normal shoulder function. As none of the patients had painful ACJ before RCR, we cannot ascertain whether the ACJ pain was related to prior cuff repair or postoperative rehabilitation thereafter or if it was a new pathology.
During DCR, the surgeon must ensure sufficient resection of the distal clavicle, as insufficient resection may result in persistent pain in symptomatic cases or trigger pain in asymptomatic cases. Some surgeons are concerned about ACJ instability attributed to excessive resection, 18 as there is little margin for error to resect the distal clavicle completely without sacrificing some ligamentous or capsular structures. Branch et al 3 suggested that a minimum of 5 mm of the distal clavicle must be resected to prevent bone-on-bone contact. In the present series, none of the patients reported any ACJ instability at a follow-up of 7.0 ± 3.1 years, likely because the target resection was 7 mm, with preservation of the extrinsic coracoclavicular ligament and superior acromioclavicular ligament.
Recent meta-analyses have advised against DCR as an adjuvant procedure during RCR, 10,18 as it does not improve clinical scores or decrease pain when compared with isolated RCR. It is worth noting that the meta-analyses reported pain ranging from 0.6 to 1.7 at mean follow-ups of 2.2 to 3.6 years, which is slightly lower than pain at rest in the present study, which remained at 2.8 ± 1.9 but at considerably longer follow-up of 7.0 ± 3.1 years. The clinical relevance of these findings is that patients should be informed about the potential for residual pain and/or functional impairment, which could be associated with other intrinsic or extrinsic factors that may be unrelated to the ACJ.
In the present series, DCR was performed in only 1.2% of patients who had undergone isolated RCR and who presented with persistent pain despite complete healing and ≥3 months of nonoperative treatment using NSAIDs, corticosteroid injections, and physical therapy. This treatment strategy is in consensus with a recent systematic review by Farrell et al 5 on nonpharmacologic treatments and criteria for surgical management of ACJ arthropathy. Farrell et al suggested that patients should undergo 4 to 6 months of nonpharmacologic and pharmacologic treatments before nonoperative management is deemed to have failed and surgical intervention is indicated.
Limitations
The results of this study should be interpreted with the following limitations. First, this is a rare procedure; therefore, only 23 patients who presented to the clinic unsolicited over a period of 9 years underwent secondary DCR for symptomatic ACJ arthropathy after isolated RCR. We did not evaluate ACJ pain in patients who did not return to the clinic or determine how many had corticosteroid injections. Second, there is considerable heterogeneity in the period between index RCR and secondary DCR, as well as between DCR and final follow-up, rendering comparison of patients inappropriate, as it is difficult to ascertain whether outcomes at final follow-up are affected by natural degeneration of the glenohumeral joint with aging. Third, the retrospective data did not include Constant-Murley score or range of motion before DCR, which prevented assessment of how DCR could have compromised or improved specific parameters, such as shoulder strength and mobility. Nevertheless, the present study is the first to report on a series of secondary DCR to treat symptomatic ACJ arthropathy after isolated RCR, and it indicates that the procedure is feasible and effective in a small subset of patients who develop this condition, hence supporting the recommendations of recent meta-analyses that DCR should not be performed during primary RCR, neither systematically nor in selected patients.
Conclusion
Secondary DCR for cases of symptomatic ACJ arthropathy after isolated RCR with complete tendon healing reduced pain in 83% of patients, though 94% were satisfied and would undergo secondary DCR again. Secondary DCR can be considered a safe treatment option for patients with residual ACJ symptoms after isolated RCR surgery.
Footnotes
Acknowledgment
The authors thank Luca Nover for assisting with the statistical analysis.
Final revision submitted December 15, 2022; accepted January 25, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: The statistical analysis and manuscript preparation for this study were funded by GCS Ramsay SanteÌ pour l’Enseignement et la Recherche. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from GCS Ramsay Santé pour l’Enseignement et la Recherche (No. COS-RGDS-2021-10-006-GODENECHE-A).