
Abstract
Background:
Purposeful rehabilitation before surgery (prehabilitation) has been researched and implemented in the treatment of anterior cruciate ligament tears. However, it is unclear whether prehabilitation would affect outcomes for baseball pitchers with partial ulnar collateral ligament (UCL) tears.
Purpose/Hypothesis:
The purpose of this study was to determine whether baseball pitchers with partial UCL tears who completed ≥4 weeks of prehabilitation (prehab group) have different return to play (RTP) outcomes than pitchers with 0 to 3 weeks of preoperative physical therapy (no prehab group). We hypothesized that pitchers in the prehab group would have similar RTP rates compared with pitchers in the no prehab group.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Baseball pitchers of all competitive levels who underwent primary UCL reconstruction (UCLR) or UCL repair between 2010 and 2019 were included. Physician chart notes, magnetic resonance images, and operative notes were screened to confirm primary UCLR or UCL repair of a partial UCL tear and to identify whether the nonoperative treatment had been attempted. Patients were contacted via RedCap for postoperative complications, reoperations, RTP, and patient-reported outcomes (Kerlan-Jobe Orthopaedic Clinic score, Andrews-Timmerman score, Conway-Jobe score, and satisfaction).
Results:
Overall, 105 baseball pitchers (n = 55 prehab group; n = 50 no prehab group) were included and evaluated at 3.4 ± 2.5 years postoperatively. Six pitchers underwent UCL repair, and 99 pitchers underwent UCLR. All demographic characteristics were similar between groups except the prehab group received a gracilis graft more frequently (76.5% vs 51.2%; P = .038). The RTP rate (prehab [88.1%] vs no prehab [93.8%]; P = .465) was similar between groups. All other postoperative outcomes were also similar between groups, including revision rates and patient-reported outcomes.
Conclusion:
Postoperative and patient-reported outcomes did not differ significantly between pitchers with partial UCL tears who performed rehabilitation before UCL surgery and pitchers who did not attempt a significant period of rehabilitation before UCL surgery. Clinicians should feel comfortable recommending rehabilitation for patients with partial UCL tears who wish to attempt a period of nonoperative treatment, as postoperative outcomes are not affected if UCL surgery is later needed.
Ulnar collateral ligament (UCL) injuries are becoming more common in both professional and recreational throwing athletes. 5,11 UCL injuries can be classified into 4 grades as follows: low-grade partial UCL tear (type 1); high-grade partial UCL tear (type 2); complete full-thickness UCL tear (type 3); or tear/pathology in >1 location of the UCL 19 (type 4). Surgical intervention is often recommended for athletes with complete tears who wish to return to play (RTP). 3 However, RTP can range from 10 to 18 months after UCL reconstruction (UCLR). 22,24 In athletes with partial UCL tears, conservative treatment is a viable option to promote ligament healing and successful outcomes. 3,23 Nonoperative treatment includes rest, activity modification, and rehabilitation, with possible biologic augmentation—such as platelet-rich plasma (PRP). 2 –4,23
Rehabilitation is often focused on strengthening the kinetic chain and the dynamic elbow stabilizers to promote ligament healing and protect the UCL. 8,9,12,20 Previous research indicates that 6% to 29% of players who attempt conservative management of a partial UCL tear ultimately require surgery. 6 Prehabilitation has been studied extensively and commonly implemented for anterior cruciate ligament (ACL) reconstruction (ACLR) to improve preoperative range of motion and quadriceps strength. 21,21 However, it is unknown whether prehabilitation can affect RTP after UCL surgery.
The primary purpose of this study was to determine whether baseball pitchers with partial UCL tears who completed ≥4 weeks of rehabilitation before surgery (prehab group) had different RTP rates than players who attempted 0 to 3 weeks of physical therapy before UCL surgery (no prehab group). The secondary purpose of this study was to compare revision, reoperation, and patient-reported outcomes between the prehab and no prehab groups. We hypothesized that pitchers in the prehab group would have similar RTP rates compared with pitchers in the no prehab group.
Methods
Inclusion and Exclusion Criteria
This retrospective cohort study was determined to be exempt from institutional review board approval. The medical records of patients aged 14 to 40 years who underwent UCL surgery at our institution between January 1, 2010, and December 31, 2019, were obtained using Current Procedural Terminology codes 24345 (“repair, revision, and/or reconstruction procedures with local tissue on the humerus [upper arm] and elbow”) and 24346 (“repair, revision, and/or reconstruction procedures with graft on the humerus [upper arm] and elbow”). Physician chart notes and operative notes were screened to confirm primary UCLR or UCL repair and to identify whether conservative treatment—and rehabilitation in particular—was attempted before UCL surgery. Physician notes in medical records, operative reports, and medical history were then screened further for included patients to collect postoperative outcomes. Patients were excluded if they were not baseball pitchers, had no available physician notes in their medical record, or if the index procedure was a revision UCLR or UCL repair. Patients were also excluded if they had a complete UCL tear identified from preoperative magnetic resonance imaging, as pitchers with a complete UCL tear who aspire to RTP are generally recommended for surgery at our institution.
Included pitchers underwent UCL surgery from 10 different orthopaedic surgeons (including B.J.E. and M.G.C.) at our institution, with a single surgeon (M.G.C.) performing the UCL surgery for 80% of the included pitchers. Patients underwent UCL repair only if they had an isolated proximal or distal tear with good-quality tissue. The decision for a patient to participate in preoperative rehabilitation was made based on the patient’s and orthopaedic surgeon’s discussions after a thorough review of the patient’s history, physical examination, the severity and location of the injury on imaging studies, and the patient’s goals.
Data Collection
A retrospective medical-record review was conducted to collect the demographic data for all eligible baseball pitchers who underwent UCL surgery. Data collected from the clinic notes included age, level of play (recreational, high school, collegiate, or professional), position played, UCL tear location (distal vs middle vs proximal), UCLR technique (Jobe, modified Jobe, docking, modified docking, or David Altcheck, Neal ElAttrache, Tommy John), duration of rehabilitation before surgery, and biologic treatments attempted (ie, PRP). The effect of bracing could not be assessed because of a lack of available information in the patient medical records. Postoperative outcomes of interest included reoperation and revision, postoperative neuropathy, RTP, return to the same level of play (RTSP), and durations of RTP/RTSP.
In addition, patients were contacted via RedCap—a secure online survey database—to complete a comprehensive set of patient-reported outcome measures. Surveys included an RTP questionnaire, a satisfaction score, the Andrews-Timmerman score (range, 20-200; higher scores indicate better postoperative outcomes), the Kerlan-Jobe Orthopaedic Clinic (KJOC) score (range, 0-100; higher scores indicate greater sport-specific shoulder and elbow function), a Single Assessment Numeric Evaluation score (range, 0-100; higher scores indicate less elbow pain), and the Conway-Jobe score (range, poor to excellent). For the Conway-Jobe score, an excellent result indicates that the patient was able to compete at the same level or higher before the injury for >12 months, a good result indicates that the patient was able to compete at a lower level for >12 months, a fair result indicates that the patient was able to return to a recreational level, and a poor result indicates that the patient was unable to return to participation.
Statistical Analysis
Demographic data, perioperative data, and postoperative outcomes were compared between the prehab and no prehab groups. The Mann-Whitney test was used to compare nonparametric data and the Student t test was used to compare parametric data. The chi-square test or the Fisher exact test was used to compare categorical data. P < .05 was deemed significant. All statistical analyses were performed using R Studio Version 3.6.3.
Results
Overall, 105 baseball pitchers were evaluated in this study (n = 55 prehab pitchers; and 50 no prehab pitchers) and were assessed at a mean of 3.4 ± 2.5 years postoperatively. Pitchers in the prehab group performed a mean of 9.5 ± 9.4 weeks of preoperative rehabilitation, while pitchers in the no prehab group performed a mean of 0.2 ± 0.8 weeks (P < .001). Prehab pitchers were more likely to attempt biologic treatment (14.5% vs 0%; P = .006); however, all other demographic characteristics were similar between groups (Tables 1 and 2). The biologic treatment consisted of PRP injections for 4 prehab pitchers and cortisone injections for the other 4 prehab pitchers.
Comparison of Characteristics Between Prehab and No Prehab Pitchers a

a Data are presented as mean ± SD or n (%). BMI, body mass index; DOS, date of surgery; prehab, prehabilitation.
Comparison of Clinical Assessment and Management Variables Between Prehab and No Prehab Pitchers a
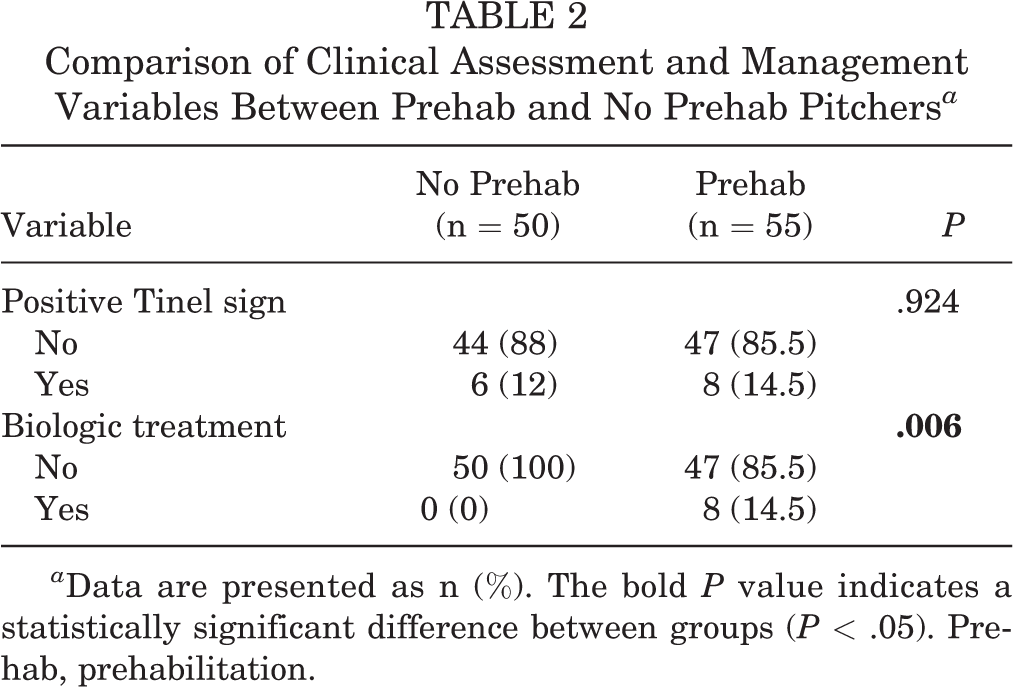
a Data are presented as n (%). The bold P value indicates a statistically significant difference between groups (P < .05). Prehab, prehabilitation.
Intraoperatively, prehab pitchers were more likely to receive a gracilis autograft (76.5% vs 51.2%) and less likely to receive a palmaris longus autograft (17.6% vs 34.9%) (P = .038) than no prehab pitchers. However, no other intraoperative variables differed between groups (Table 3).
Comparison of Intraoperative Variables Between Prehab and No Prehab Pitchers a

a Data are presented as n (%). The bold P value indicates a statistically significant difference between groups (P < .05). Prehab, prehabilitation; UCL, ulnar collateral ligament; UCLR, ulnar collateral ligament reconstruction; UNT, ulnar nerve transposition.
The presence of postoperative ulnar nerve symptoms was similar between groups (4% vs 0%; P = .496) (Table 4). Revision was required in 2% of the no prehab group and 1.8% of the prehab group, which did not differ significantly between groups (≥.999). Also, 88.1% of pitchers in the no prehab group returned to sport in 12.8 ± 5.2 months and 93.8% of pitchers in the prehab group returned to sport in 14 ± 4.1 months (RTP rate and time, P = .465 and P = .307, respectively).
Comparison of Postoperative Outcomes Between Prehab and No Prehab Pitchers a
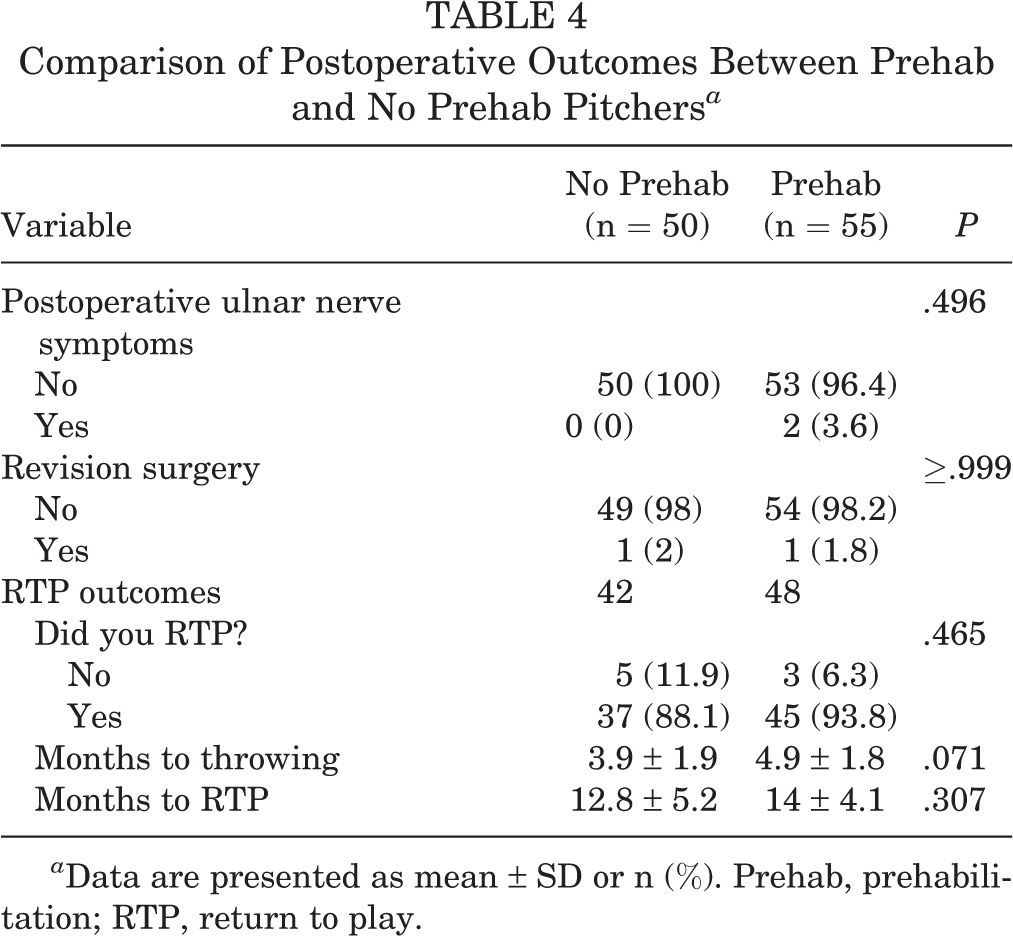
a Data are presented as mean ± SD or n (%). Prehab, prehabilitation; RTP, return to play.
Overall, 29 pitchers in the no prehab group and 27 pitchers in the prehab group completed the patient-reported outcome survey (55%). Sport-specific subjective outcomes did not differ between the groups according to the KJOC score (82.4 vs 79.1, respectively; P = .426) (Table 5). There were no significant between-group differences in any of the other patient-reported outcomes.
Comparison of Patient-Reported Outcomes Between Prehab and No Prehab Pitchers a
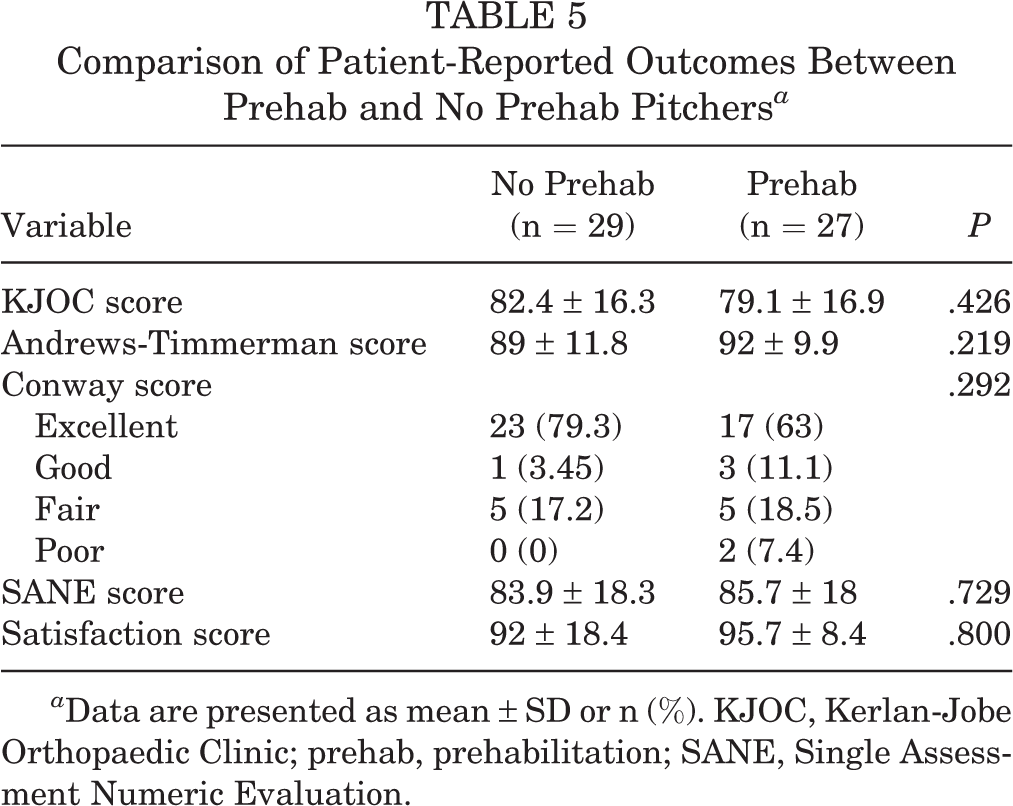
a Data are presented as mean ± SD or n (%). KJOC, Kerlan-Jobe Orthopaedic Clinic; prehab, prehabilitation; SANE, Single Assessment Numeric Evaluation.
Discussion
This study primarily aimed to determine whether rehabilitation before UCL surgery affects RTP rates in baseball pitchers with partial UCL tears and secondarily evaluated whether revision, reoperation, and patient-reported outcomes were affected by prehabilitation. The results of the present study supported our primary hypothesis, as the RTP rate did not differ significantly between pitchers who performed rehabilitation before UCL surgery (prehab group) and pitchers who did not attempt a significant period of rehabilitation before UCL surgery (no prehab group). The secondary study hypotheses were also supported because revision and reoperation rates, as well as patient-reported outcomes, did not differ between groups. However, the rehabilitation program utilized for each player is unclear and no validated prehabilitation programs were available for pitchers during the study period. Thus, further research is necessary before a strong clinical recommendation should be made.
Prehabilitation aims to enhance general health and well-being before major surgery. It prepares patients to “weather the storm” of their operation and minimizes postoperative complications such as weakness, stiffness, and reinjury. Prehabilitation is well-established in the treatment of patients undergoing ACLR and is generally recommended for 2 to 6 weeks before surgery. 4 During this time before ACLR, prehabilitation allows the patient to gain quadriceps and hamstring muscular strength, improve knee flexion/extension and range of motion, increase neuromuscular coordination, and increase confidence. 1,15 As presented by Giesche et al 15 and Adriani et al, 1 preoperative neuromuscular coordination has been identified as a predictive factor for postoperative knee function and RTP after ACLR, and RTP occurs less frequently in patients undergoing ACLR patients with poor neuromuscular coordination than in those with better neuromuscular coordination
Similarly, performing prehabilitation for pitchers with partial UCL tears may help improve neuromuscular coordination through the kinetic chain, as many pitchers with UCL tearing present with kinetic chain deficits. Strengthening of the hips, core, scapular, and shoulder muscles, and regaining optimal shoulder range of motion may help decrease the force imposed upon the UCL. However, the present study found that pitchers who attempted rehabilitation before UCL surgery had similar outcomes to pitchers who underwent UCL surgery with no/minimal preoperative rehabilitation. This may be due to the length of postoperative rehabilitation, where there is much more time compared with ACLR postoperative rehabilitation to develop strength and improve neuromuscular coordination in the affected and surrounding joints. Also, unlike ACLR, the injured joint itself (elbow) does not suffer directly from joint stiffness (effusion) or weakness that can be directly rehabilitated—the focus is instead on optimizing the kinetic chain.
While prehabilitation has well-established benefits for patients undergoing ACLR as well as emerging benefits for acetabular labral repair and rotator cuff repair (RCR), 1,2,11,15 the present study found no benefit in performing prehabilitation before UCL surgery for baseball pitchers with partial UCL tears. This may be due to the lower extremity having to bear weight soon after surgery compared with the throwing elbow not needing to withstand significant valgus stress in daily life and throwing postponed until 4 to 6 months after UCL surgery. Furthermore, when an ACL injury occurs, the hemarthrosis often causes quadriceps shutdown, whereas a UCL injury is often less traumatic and causes less damage to surrounding tissues. Also, since the length of rehabilitation after UCL surgery is often longer than that of ACLR, there is more time to address potential neuromuscular control and biomechanical deficits. Last, the mechanism of ACL injury is generally acute, while UCL injury is often due to overuse and/or repetitive submaximal trauma. Therefore, the necessity for prehabilitation to work on any neuromuscular deficits may be less relevant for UCL injuries.
Ford et al 13 found that of 28 players with incomplete UCL injuries who completed nonoperative rehabilitation, 26 (93%) had a successful RTSP. Thus, players who are indicated for nonoperative treatment may have successful outcomes concerning RTP and RTSP without surgery. However, identifying baseball players who should succeed with nonoperative treatment is challenging, with many important factors to consider, such as partial- versus full-thickness UCL tears, proximal versus distal injury, amount of UCL laxity, timing of the competitive season, and much more. Players who are candidates for nonoperative treatment often attempt nonoperative treatment to RTP faster and avoid surgery. However, those who fail nonoperative treatment and later require surgery ultimately wind up returning to play even later because of the failed nonoperative treatment duration. Thus, further improvements in the indications and contraindications for nonoperative treatment are still necessary to help minimize lost playing time.
Delay in surgery has been shown to negatively affect the outcomes of various orthopaedic surgeries. For example, RCRs that are delayed >1 year after an injury have a higher risk of retear compared with surgeries performed earlier. 14,17 A recent meta-analysis by van der List et al 17 found that among 3494 patients, patients undergoing RCR >1 year from injury were at an increased risk (odds ratio, 2.9) of retear compared with patients who underwent surgery within 1 year from injury. However, this effect was not observed with shorter time points, with comparisons of undergoing RCR at 3 months and 6 months after injury showing statistically similar retear rates. 17 While a drastic delay in undergoing UCL surgery may affect postoperative outcomes, the delay due to attempting rehabilitation is likely much shorter than 1 year, which may explain why no differences in outcomes were observed in the present study. Further research is needed to clarify the role of surgery timing on UCL surgery, as the findings between RCR and UCL surgery may not be generalizable.
Although we found no difference in the primary hypothesis, there were several interesting findings. First, pitchers in the prehab group were found to be the only pitchers who attempted biologic treatment in this study. Several studies have evaluated the use of biologic augmentation, including several case series and 1 study that utilized the Major League Baseball (MLB) Health and Injury Tracking System database. 4,7 While the case series reported good results after PRP injections, the MLB database study did not see any added benefit of PRP. Mills et al 19 performed a retrospective study to evaluate the success of biologic augmentation in the nonoperative treatment of UCL tears and concluded that the success of biologic treatment in treating these UCL tears is dependent on the severity of the injury. Overall, 23 athletes had low-grade partial UCL tears, 16 had high-grade partial UCL tears, and 11 had complete UCL tears. Also, 26 of 50 (52%) athletes were able to return to their baseline level of function and performance with solely biologic treatment and rehabilitation. However, the athletes with partial UCL tears were found to be 3.8 times more likely to succeed without surgical intervention compared with athletes with complete tears. 19 In the present study, it makes sense that only pitchers in the prehab group received biologic treatment, as most clinicians will give the biologic treatment at least 6 to 8 weeks to see how the patient responds before progressing to surgery.
Pitchers in the prehab group were also more likely to receive a gracilis graft and less likely to receive a palmaris longus graft relative to pitchers in the no prehab group. Several studies have evaluated the effects of graft type on professional baseball RTP and pitching performance after UCLR. 10,16,18 One study found that pitchers who received a palmaris longus graft RTP more frequently than those who received gracilis grafts, while the other 2 studies found no difference in RTP rates based on the graft utilized. 10,16,18 Therefore, it is possible that none of the pitchers in the prehab group had an increased RTP rate because of an increased usage of palmaris longus grafts in this cohort. RTP did not differ between groups in the present study.
Limitations
There are several limitations to this study. First, this study was performed retrospectively. Thus, rehabilitation protocols were not randomized or standardized, and decision-making about which pitchers would attempt rehabilitation was also not standardized. A future prospective study comparing pitchers with UCL tears who do and do not perform a validated prehabilitation program will help clarify the effect of prehabilitation for baseball pitchers. Second, the timing of surgery throughout the competitive season was not evaluated. Therefore, the timing of surgery could have differed between groups and affected RTP duration. Third, low- and high-grade partial UCL tears were not able to be differentiated because of inconsistent reporting of low- versus high-grade tearing in the medical-record review. Fourth, pitchers who did not require surgery were not evaluated; thus, the success rate of rehabilitation alone was not determined. Finally, this study was limited by a low rate of patient-reported outcome survey completion (55%).
Conclusion
Postoperative and patient-reported outcomes did not differ significantly between pitchers with partial UCL tears who performed rehabilitation before UCL surgery and pitchers who did not attempt a significant period of rehabilitation before UCL surgery. Clinicians should feel comfortable recommending rehabilitation for patients with partial UCL tears who wish to attempt a period of nonoperative treatment, as postoperative outcomes are not affected if UCL surgery is later needed.
Footnotes
Final revision submitted December 22, 2022; accepted January 19, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.J.E. has received research support from Arthrex, DePuy, Linvatec, Smith & Nephew, and Stryker; education payments from Arthrex and Smith & Nephew; and consulting fees from Arthrex, DePuy, and Smith & Nephew. M.G.C. has received grant payments from Arthrex and DJO and education support from Liberty Surgical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by Thomas Jefferson University (ref No. 21E.528).