
Abstract
Background:
The advantages of remnant tissue preservation in anterior cruciate ligament (ACL) reconstruction (ACLR) remain controversial.
Hypothesis:
It was hypothesized that a large amount of remnant tissue, especially if anatomically positioned, would improve patient-reported outcomes and second-look graft appearance after preserved double-bundle ACLR (DB-ACLR).
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This retrospective study included 89 consecutive patients who underwent unilateral remnant-preserving DB-ACLR using 2 hamstring tendon autografts. The authors categorized the arthroscopic findings into 3 groups according to the location and volume of the ACL remnant tissue in the femoral notch: (1) anatomical attachment (group AA; n = 34); (2) nonanatomical attachment (group NA; n = 33); and (3) no remnant (group NR; n = 22). Based on second-look arthroscopy, the reconstructed graft was graded as excellent, fair, or poor. Patient-reported outcomes were evaluated at 2 years after surgery using the Knee injury and Osteoarthritis Outcome Score (KOOS) and the Japanese Anterior Cruciate Ligament Questionnaire–25 (JACL-25).
Results:
The AA and NA groups had a significantly shorter time from injury to surgery compared with the NR group (P = .0165). Considering the second-look arthroscopic findings, the authors found a significant difference in synovial coverage of the grafts between the 3 groups (P = .0018). There were no significant differences in the overall KOOS and JACL-25 score among the 3 groups; however, the KOOS–Sport and Recreation and KOOS–Quality of Life subscale scores were significantly higher in the AA group compared with the NA and NR groups (P = .0014 and .0039, respectively). The JACL-25 score for middle- to high-speed flexion and extension was significantly better in the AA group versus the NR group (P = .0261).
Conclusion:
This study showed that preserving anatomically positioned and adequate remnant tissue during DB-ACLR improved second-look graft appearance and KOOS–Sport and Recreation and KOOS–Quality of Life scores.
Keywords
Several surgical options for achieving better outcomes after anterior cruciate ligament (ACL) reconstruction (ACLR) have been reported in the literature. Based on laboratory, animal, and biomechanical studies, a number of authors have reported that remnant-preserving ACLR may improve mechanical stability, biological healing of ACL grafts, and knee function. 19,25,36,47,49,53 Improved postoperative graft maturation at second-look arthroscopy has been reported after ACLR with a remnant tissue–preserving procedure compared with a remnant tissue–resecting procedure. 25,34 Remnant preservation during ACLR may accelerate graft healing, depending on the morphological remnant condition and the amount of preserved remnant. However, meta-analyses have reported no differences in clinical outcomes or knee stability between ACLR with versus without remnant preservation. 29,52 In addition, some authors have mentioned impingement and formation of cyclops lesions after remnant-preserved ACLR. 4,47,63
Crain et al 11 developed a classification system for remnant ACL tissue (type 1, ACL wrapped around the posterior cruciate ligament [PCL]; type 2, ACL healed to the roof of the notch; type 3, remnant healed to the lateral wall of the notch or the medial aspect of the lateral femoral condyle in a position anterior and distal to the ACL anatomic footprint; and type 4, no ligament tissue remaining). However, there are some cases in which the location and volume of the remnant tissue cannot be classified using this system, for example, when the remnant tissue is located in the femoral anatomical position of the torn ACL. Clinically, in the early phase after injury, remnant tissue occasionally exists attached to the anatomical site at the femoral side with a large amount (anatomically located and a large amount of remnant tissue) of the torn ACL. However, to our knowledge, there is no study regarding the preservation of remnant tissue at the femoral side in ACLR despite existing mechanoreceptors, including Pacinian corpuscles, Ruffini endings, and Golgi tendon organs, at the femoral attachment and tibial sites of the ACL. 15,46,63 Therefore, we speculate that the preservation of such remnant tissue might have the potential to improve the outcome of ACLR.
The purpose of the current study was to clarify the effect of remnant condition on postoperative outcomes and graft appearance after remnant-preserving double-bundle ACLR (DB-ACLR). We hypothesized that a large amount of remnant tissue, especially if anatomically positioned, would improve outcomes and graft appearance.
Methods
Study Design
The protocol for the study was approved by the institutional review board of our hospital. In this retrospective cohort study, we reviewed the records of 142 consecutive patients with an ACL-deficient unilateral knee who underwent anatomic DB-ACLR with or without remnant tissue preservation using 2 hamstring tendon autografts at NTT East Japan Sapporo Hospital between January 2014 and July 2018. The diagnosis of ACL rupture was confirmed based on magnetic resonance imaging and physical findings. One well-trained senior orthopaedic surgeon (M.I.) performed all operative procedures using the same protocol, and the same postoperative rehabilitation protocol was used for all patients. 23,59 The inclusion criterion was a time from injury to surgery within 6 months after ACL injury. Exclusion criteria included patients with an isolated anteromedial (AM) or posterolateral (PL) bundle tear, patients with a combined injury in other knee ligaments, and patients who had undergone any previous knee operations. Of the 142 initial patients, 41 patients did not meet the inclusion criteria, leaving 101 eligible patients (101 knees). All patients were informed that if they did not want to participate in this study, they could choose a non–remnant preserved ACLR procedure. The patients were also informed that a C-arm fluoroscope would be used intraoperatively.
Before the ACLR procedure, we arthroscopically observed the morphological status of the remnant tissue in each participant. First, we carefully observed the condition of the remnant tissue via arthroscope and recorded our findings on video. Then we performed the reconstruction. At the follow-up examination, with the aid of the surgical records and videos, we categorized the condition of the ACL remnant tissue on arthroscopic findings into 3 groups according to the location and volume of the remnant. In cases of anatomical attachment (group AA; n = 34) (Figure 1A), the remnant was attached to the anatomical site in the distal femur, but anterior laxity was grossly visible and 2 distinct patterns were observed: (1) remnant tissue in which ≥50% of the injured ACL could be observed at the anatomical site, or (2) remnant tissue remained at the anatomical site of the AM or PL bundle, although the bundle was partially detached from the distal femur. In knees with nonanatomical attachment (NA group; n = 33) (Figure 1B), the remnant was attached to the outside of the AM bundle footprint in the distal femur, and 3 patterns were visible: (1) ACL fibers were retracted and matted down to the PCL (Crain type 1); (2) ACL disruption was healed and attached to the roof of the notch (Crain type 2); or (3) remnants were attached to the medial aspect of the lateral femoral condyle in a position anterior and distal to the ACL anatomical footprint (Crain type 3). In knees with no remnant (NR group; n = 22) (Figure 1C), there was no identifiable spanning of ligament tissue, even in the short gap between the tibial stump and the PCL (Crain type 4).

Characteristic patterns of the 3 categories of anterior cruciate ligament remnant condition. (A) Anatomical attachment (group AA): (1) a large amount of remnant is attached to the anatomic site of anteromedial (AM) and posterolateral (PL) bundles, but anterior laxity is obviously observed; and (2) a large amount of remnant is attached to the anatomic site of the AM or PL bundle, and a partial detachment of the AM or PL bundle is visible. (B) Nonanatomical attachment (group NA): remnant is scarring posterior cruciate ligament (Crain type 1) (1), remnant is attached to the roof of the notch (Crain type 2) (2), or remnant is attached to the nonanatomic site of the AM and PL bundle (Crain type 3) (3). (C) No remnant (group NR): the remnant is absent in the femoral wall. Arrow indicates the attachment site of ACL.
We evaluated the patients in our outpatient clinic for ≥2 years after surgery; 3, 5, and 4 patients were lost during the follow-up in the AA, NA, and NR groups, respectively. Thus, 89 patients (88%) participated in this study and underwent clinical evaluation (Figure 2). They underwent second-look arthroscopy approximately 1 to 2 years after surgery, when 2 double-spike plates that were inserted into the tibia were removed.
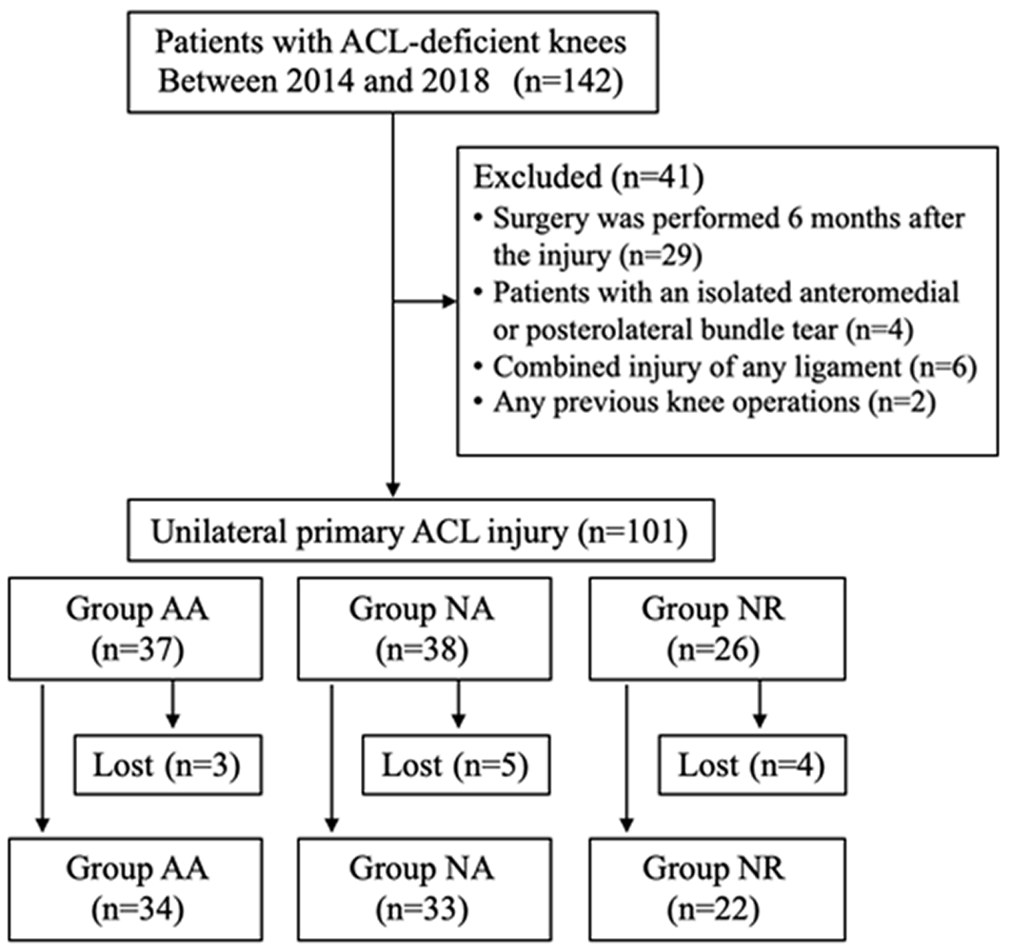
Flowchart of the study design. AA, anatomical attachment; ACL, anterior cruciate ligament; NA, nonanatomical attachment; NR, no remnant.
Surgical Procedure of Remnant-Preserved Anatomic DB-ACLR
A standard arthroscopic examination was performed via the anterolateral, AM, and central portals. After observing the ruptured ACL, cartilages and menisci conditions, and any additional treatments of the intra-articular lesions, were recorded (Table 1). The remnant tissue of the injured ACL on both the femoral and the tibial sides was left intact. A 3-cm longitudinal skin incision was made on the upper pes anserinus. After the semitendinosus tendon was harvested with a tendon stripper, the former tendon was cut in half and folded. The distal half of the semitendinosus tendon was used to create the AM bundle graft, and the proximal half was used for the PL bundle graft. Before grafting, an Endobutton CL (Smith & Nephew) was attached to the looped end. The length of the loop was matched to that of the femoral tunnel measured during surgery. Fiber loop tape (Arthrex), which is a commercially available polyester tape, was mechanically connected to the other end of the doubled tendons using the SpeedWhip Rip-Stop Graft Preparation Technique.
Arthroscopic Intra-articular Treatment a

a Data are reported as n (%). AA, anatomical attachment; NA, nonanatomical attachment; NR, no remnant.
Arthroscopic anatomic DB-ACLR with preservation of the remnant tissue was performed as previously described. 58,60 We used the C-arm image intensifier system during arthroscopic surgery to confirm the anatomical aiming point considering that a large amount of remnant obstructed the view of the femoral and tibial attachments. When the remnant was attached to the anatomic site of the AM bundle and the volume of the remnant was sufficient, a behind-remnant 21 approach was performed according to previously described methods.
Briefly, for tibial tunnel placement, the centers of the tibial footprints of the AM and PL were marked using a radiofrequency device based on the lateral knee image obtained with the C-arm image intensifier system. A tibial tunnel for the AM and PL bundles was created using a hole-in-1 guide (Wire-navigator; Smith & Nephew) following the marked points. Two tibial tunnels were made with a cannulated drill of up to 1 mm under the measured diameter of the prepared substitute. For femoral tunnel placement, the anatomical position of the femoral footprints was marked using a radiofrequency device based on the lateral knee images obtained with the C-arm image intensifier system. The 2 femoral sockets were created using the transtibial approach following the marked points for the AM and PL bundle grafts with cannulated drills. The locations of the tunnels have been previously reported. 24,59 If the tunnel location in the fluoroscopic image was not appropriate, the guide pin was removed and reinserted using the ACL tibial or femoral guide. If the location of the guide pin was correct, anteroposterior and lateral views of the knee were obtained using fluoroscopy; subsequently, each tunnel location was checked.
The graft for the AM and PL bundles was introduced through the remnant from the tibial tunnel to the femoral tunnel, using a passing pin. The Endobutton was flipped onto the femoral cortical surface. Thus, the 2 bundles were covered with the remnant (Figure 3). First, an assistant surgeon simultaneously applied a tension of 40 N to each graft using a tensiometer (Meira Corp) during 0° to 120° of knee motion. A surgeon simultaneously secured the 2 tape portions onto the tibia using a double-spike plate (Meira Corp) in the knee extension position. Finally, 15 N was applied to the grafts.
All the patients underwent postoperative management using the same rehabilitation protocol. 40,57,58 The rehabilitation protocol was the same for patients who underwent meniscal repair and meniscal resection.

Arthroscopic images during anterior cruciate ligament reconstruction. (A) The remnant was attached to the anatomic site of the anteromedial (AM) bundle and partially detached from the posterolateral (PL) bundle (AA group). (B) The AM and PL grafts (arrow) were placed using the behind-remnant method.
Clinical Evaluation
Each patient underwent clinical examinations once before surgery and again 2 years after surgery. Pivot shift was evaluated with the objective International Knee Documentation Committee (IKDC) scoring system. Side-to-side differences in anterior laxity were measured with a KT-2000 arthrometer (MEDmetric) at 30° of flexion under an anterior drawer force of 133 N. Peak isokinetic torque of the quadriceps and hamstrings was measured at 60° per second of angular velocity using Biodex System 3 (Biodex Medical Systems) in both knees before and after surgery. Muscle torque measured preoperatively and postoperatively in the uninvolved knee was represented as a ratio (percentage) to the uninvolved value.
At 2 years postoperatively, patients completed the Knee injury and Osteoarthritis Outcome Score (KOOS) 44 and the Japanese Anterior Cruciate Ligament Questionnaire–25 (JACL-25). 33 The JACL-25 was developed to assess fear of motion during daily activity and sports participation in patients with ACL injuries. It contains 25 items with scores ranging from 0 to 100, with subscale scores for each motion type: middle- to high-speed flexion and extension (up to 56 points), low-speed flexion and extension (up to 20 points), and abduction and adduction (up to 28 points); 1 question for middle- to high-speed flexion and extension overlaps with the abduction and adduction section. Higher scores indicate worse psychological readiness.
Second-Look Arthroscopic Examination
On second-look arthroscopy, the AM and PL bundle grafts were observed at various angles of knee flexion by using the standard technique with the lateral parapatellar portal. Specifically, the PL bundle graft was observed in the figure-4 position. Graft quality was evaluated based on the thickness and apparent tension of the graft, as well as the synovial coverage of the graft, according to a previous method. 22 The graft thickness and apparent tension of the reconstructed graft were graded as A (no elongation of a sufficiently thick graft), B (elongation of a relatively thin graft), or C (obvious elongation of the graft). In addition, synovial coverage of the reconstructed graft was graded as A (completely covered), B (partially covered), or C (almost uncovered). For the overall evaluation of each bundle, we assigned 2 points for grade A, 1 point for grade B, and 0 points for grade C and summed the 2 scores. A total score of 4 points was deemed “excellent,” 2 or 3 points was deemed “fair,” and 0 or 1 point was deemed “poor.”
Statistical Analysis
All data were presented as the mean ± SD. The Kolmogorov-Smirnov test was used to check the data for normality. Comparisons within the AA, NA, and NR groups were performed using 1-way analysis of variance with the Fisher protected least significant difference test for post hoc multiple comparisons and the Kruskal-Wallis test followed by the Mann-Whitney U test for ordinal categorical and nonnormally distributed data. The Pearson chi-square test was used for categorical data. A commercially available software program (GraphPad Software) was used for the statistical calculations. The significance level was set at P < .05. In addition, we evaluated the association between age and time from injury to surgery using the Pearson correlation coefficient.
Results
Patient Characteristics
The 89 study patients included 42 men and 47 women with a mean age of 30.4 years (range, 13-68 years). The mean ages of the AA, NA, and NR groups were 36.5, 30.0, and 22.1 years, respectively. Patients in the AA and NA groups were significantly older compared with patients in the NR group (AA vs NR, P = .0001; NA vs NR, P = .0405). Patients underwent reconstruction at a mean of 51.2, 55.9, and 75.1 days after injury in groups AA, NA, and NR, respectively, with significant differences between groups AA and NR (P = .0229) and groups NA and NR (P = .0423). The other background factors for each group are listed in Table 2. The medial and lateral menisci were injured in 52 patients.
Patient Characteristics a

a Data are reported as mean ± SD unless otherwise indicated. The 3 groups were compared using 1-way analysis of variance, with post hoc pairwise comparisons for significant differences using the Fisher protected least significant difference test. Bolded P values indicate statistical significance (P < .05). AA, anatomical attachment; NA, nonanatomical attachment; NR, no remnant.
Objective Clinical Outcomes
None of the groups experienced any intra- or postoperative complications, such as iatrogenic cartilage injuries, tunnel malposition, graft fixation failure, delayed wound healing, deep vein thrombosis, infection, cyclops syndrome, joint contracture, or fracture. There were no significant differences in clinical outcomes among the 3 groups (Table 3).
Comparisons of Clinical Outcomes Among Groups a
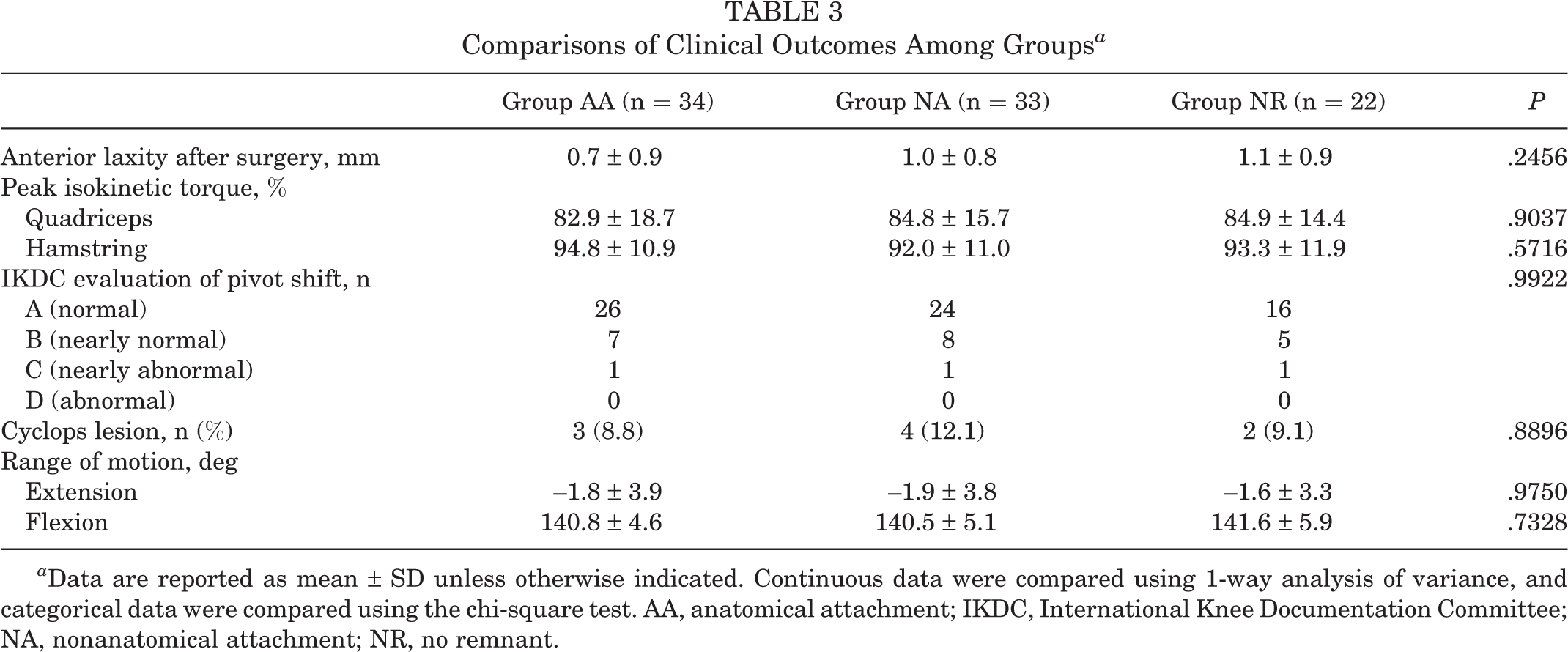
a Data are reported as mean ± SD unless otherwise indicated. Continuous data were compared using 1-way analysis of variance, and categorical data were compared using the chi-square test. AA, anatomical attachment; IKDC, International Knee Documentation Committee; NA, nonanatomical attachment; NR, no remnant.
Patient-Reported Outcomes
The patient-reported subjective clinical outcomes after surgery are shown in Table 4. Scores on the KOOS–Sports and Recreation and KOOS–Quality of Life subscales were significantly higher in group AA versus groups NA (P = .0301 and .0354, respectively) and NR (P = .0050 and .0309, respectively). The middle- to high-speed flexion and extension score of the JACL-25 was significantly lower (ie, better) in group AA versus group NR (P = .0490).
Patient-Reported Outcome Scores After Surgery a

a Data are reported as the mean ± SD unless otherwise indicated. The 3 groups were compared using 1-way analysis of variance, with post hoc pairwise comparisons for significant differences using the Fisher protected least significant difference test. Bolded P values indicate statistical significance (P < .05). AA, anatomical attachment; JACL-25, Japanese Anterior Cruciate Ligament Questionnaire–25; KOOS, Knee injury and Osteoarthritis Outcome Score; NA, nonanatomical attachment; NR, no remnant.
Results of Second-Look Arthroscopy
The mean period from ACLR to second-look arthroscopic examination was 14 months (range, 11-24 months). The results of the second-look arthroscopic examination are shown in Table 5 and Figure 4. There were significant differences between the 3 groups regarding synovial coverage and overall evaluation of the AM bundle graft (P = .0018 and .0279, respectively). Residual analysis revealed that the synovial coverage and overall evaluation in group AA were significantly better than those in group NR (P = .0029 and .0030, respectively). Regarding the graft appearance of the PL bundle on second-look arthroscopy, there were significant differences between the 3 groups regarding thickness and apparent tension, synovial coverage, and overall evaluation (P = .0126, .0017, and .0115, respectively). Residual analysis revealed that thickness and apparent tension in groups AA and NA were significantly better than those in group NR (P = .0013 and .016, respectively), and synovial coverage and overall evaluation in group AA were significantly better than those in group NR (P = .0057 and .032, respectively).
The results of the correlation analysis showed a moderate but significant negative association between patient age and time from injury to surgery (r = –0.3056; P = .0036) (Figure 5).
Evaluation of AM Bundle Graft and PL Bundle Graft on Second-Look Arthroscopy a
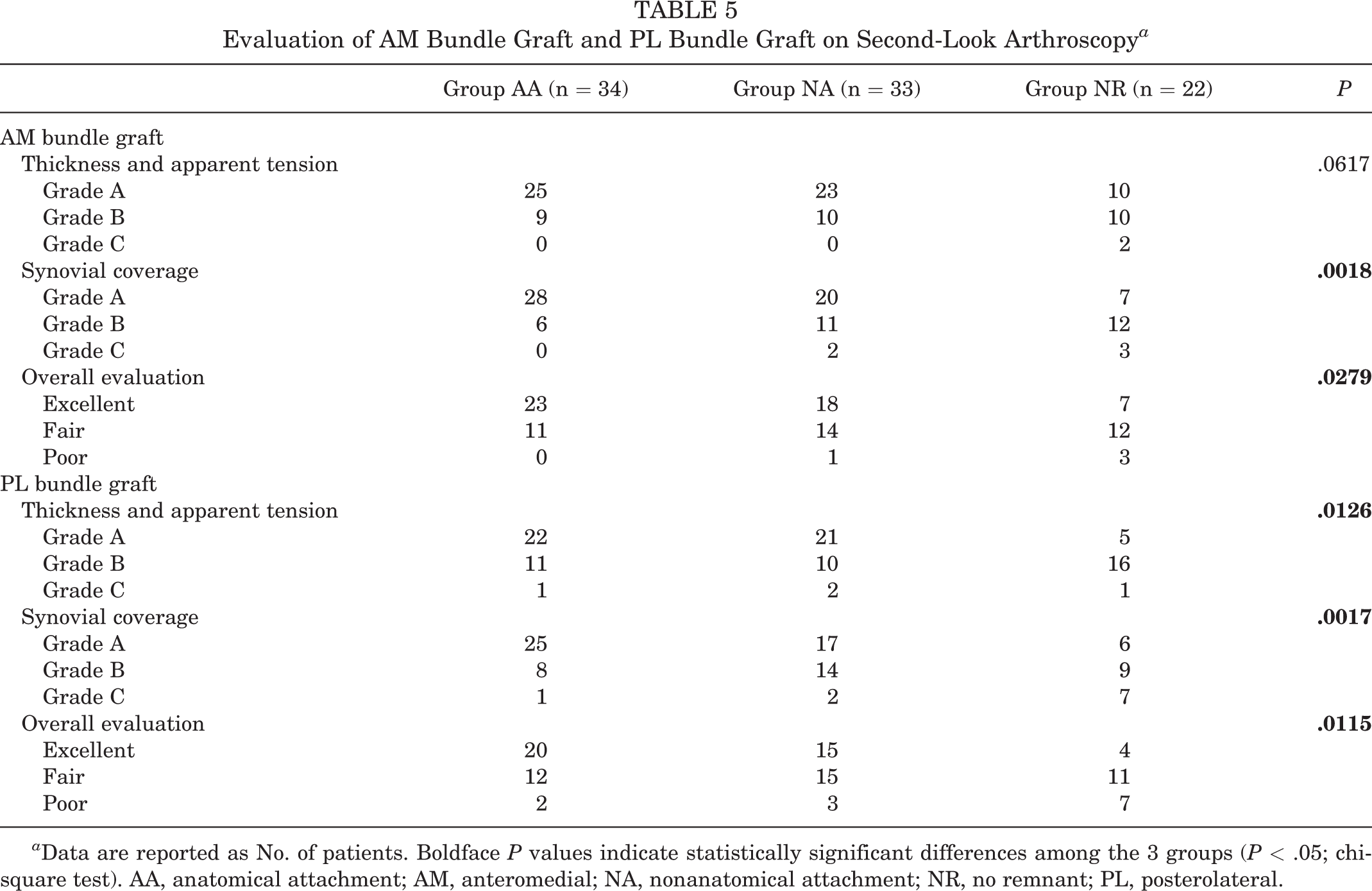
a Data are reported as No. of patients. Boldface P values indicate statistically significant differences among the 3 groups (P < .05; chi-square test). AA, anatomical attachment; AM, anteromedial; NA, nonanatomical attachment; NR, no remnant; PL, posterolateral.

Intraoperative second-look arthroscopic images showing (A) the synovium completely covered and (B) no laceration or elongation of a sufficiently thick graft in the anatomical attachment group; (C) the synovium partially covered and (D) partial laceration of a sufficiently thick graft or no laceration or elongation of a relatively thin graft in the nonanatomical attachment group; and (E) the synovium of the anteromedial bundle almost not covered and (F) partial laceration of a sufficiently thick graft or no laceration or elongation of a relatively thin graft in the no remnant group.
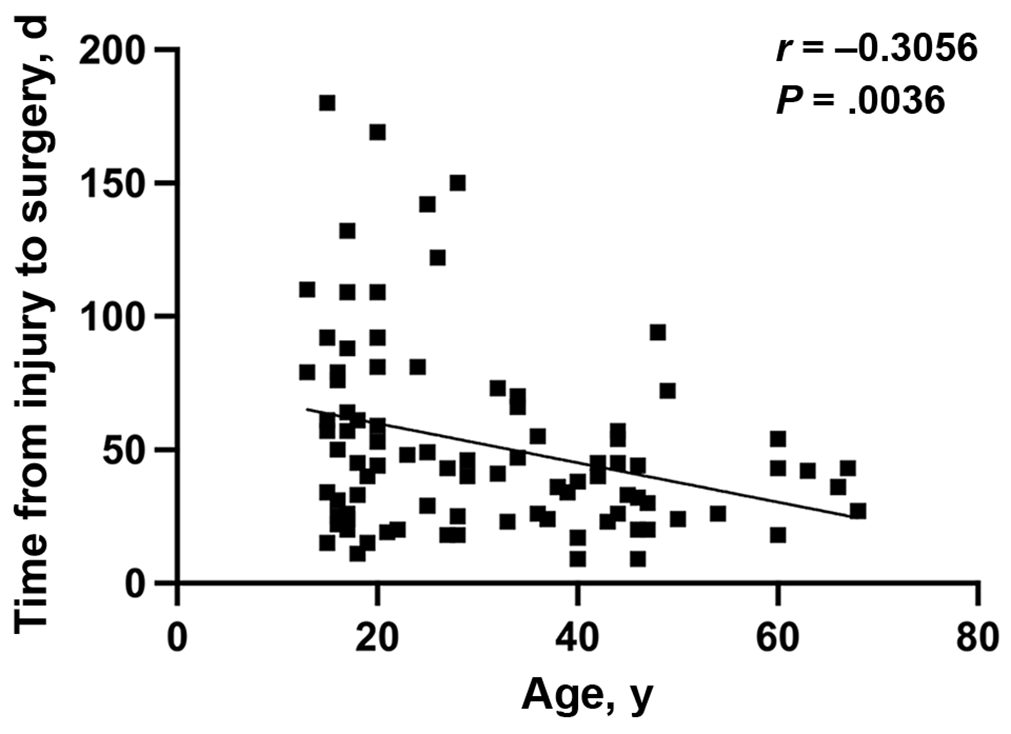
Results of correlation analysis between age and time from injury to surgery.
Discussion
The most important findings of this study were that group AA had significantly better results in some parameters of patient-reported clinical outcomes (KOOS–Sports and Recreation, KOOS–Quality of Life, and JACL-25 middle- to high-speed flexion and extension) and morphological healing of the reconstructed graft than groups NA and NR. These results indicate that a large number of remnants attached to the anatomical site of the femoral notch had enhanced advantages in patient-reported outcomes, as well as in second-look arthroscopic findings in anatomic DB-ACLR with remnant tissue preservation. This supports our hypothesis that preservation of anatomically attached remnant tissue in large amounts may enhance graft morphology and improve some parameters of patient-reported clinical outcomes.
Although some studies on the use of preserved remnants during ACLR have been conducted, none have classified the condition of the remnant in terms of volume and attachment position at the femur in detail. Moreover, to date, no studies have compared the effect of specific remnant type on graft appearance and clinical outcomes after anatomic DB-ACLR. Furthermore, in the study by Crain et al, 11 ACLR was performed within a mean of 78 weeks after injury, whereas the time from injury to surgery was 8 weeks in the current study, and the time frame was significantly shorter in the AA and NA groups than in the NR group. The preservation of such anatomically located and large amounts of remnant tissue might have the potential to improve the outcome of ACLR.
The timing of reconstruction after an ACL injury has been debated as a significant factor that affects clinical outcomes after ACLR. 48 Concerning the influence of the timing of ACLR on postoperative knee stability, there have been controversies in previous studies. 2,3,7 Ahn and Lee 3 reported that the time from injury to surgery over 12 weeks was found to be a significant risk factor for postoperative instability after single-bundle reconstruction. Recently, Baba et al 6 reported that early DB-ACLR was significantly better than delayed DB-ACLR in terms of postoperative anterior and rotatory knee stability. Regarding the preservation of ACL remnant tissue, some authors have reported that early surgical intervention may achieve better clinical results since healing potential could be maintained in the early phase after injury. 27,35,38,39,62 In the Inokuchi et al 17 study, compared with human ACL–derived cells obtained during the chronic phase, cells obtained during the early phase after injury had a greater tendon-bone healing potential when used in an immunodeficient rat model of ACLR. In addition, Gao et al 12 reported that the number of mechanoreceptors in the ACL stump and the volume of the stump decreased with time from injury to surgery. A recent study 8 noted that the number of Golgi-Mazzoni corpuscles decreased significantly with time. In the present study, there were significant differences in the time from injury to surgery between the remnant groups (groups AA and NA) and group NR. This study showed that preservation of anatomically located and adequate remnant tissue improved graft appearance in second-look arthroscopy. The clinical relevance of the results from this study is that in acute ACLRs, preservation of the ACL remnant should be considered because, at this time after injury, the remnant may present the greatest healing potential.
There were significant differences in patient age between the 3 study groups. We speculate that timing between injury and ACLR might have affected them. Our study showed that the time from injury to surgery in the NR group was significantly longer than that in the AA and NA groups and there was a moderately negative correlation between age and time from injury to surgery. This implies that younger patients had a longer time from injury to surgery. In addition, a previous study reported that the regression model confirmed a negative relationship between the volume of the ACL stump and the time from injury to surgery. 12 Taken together, younger patients were distributed into the NR group, which was the nonremnant group, so that there were differences in age between the groups. We also have concerns about the effect of age on clinical outcomes. Recent studies have reported comparable clinical outcomes between older and younger patients. 10,18 Nishio et al 37 reported that equivalent clinical outcomes (Lysholm and IKDC scores) were observed between 2 age groups (patients ≥40 and <40 years of age) after DB-ACLR. Mall et al 31 reported a systematic review of the results of single-bundle ACLR in patients aged >40 years. They reported that the outcomes were similar to those in younger patients. On the other hand, Magnitskaya et al 30 reported that patients aged ≥30 years had lower IKDC scores than those aged <30 years. Saito et al 45 reported that patients aged >40 years exhibited lower IKDC scores than younger patients. Therefore, a consensus has not been reached as to whether differences in patient age influence clinical outcomes. However, attention should be paid to some problems that involve less muscle strength and bone tunnel enlargement with older age.
Preserved ACL remnants have been reported to accelerate revascularization and promote graft incorporation. 1,41 However, it is not easy to evaluate the effects of remnant preservation on clinical outcomes and synovial coverage of the graft by physical and radiological examinations. In this study, patient-reported outcomes were used to verify the advantages of remnant-preserved ACLR. To examine the effect of preservation of remnant tissue on patient satisfaction more precisely, both the KOOS and JACL-25 were used. Previously, the JACL-25 was reported to be reliable, responsive, and appropriate for the assessment of patient outcomes after ACLR. 33 Regarding the effect of preservation of remnant tissue on synovial coverage of the graft, the graft maturation was observed when a large amount of remnant tissue located anatomically was preserved during ACLR. In other words, we showed that the ACL remnant was a better feature in patient-reported outcomes and graft synovialization because ACL remnants may create accelerated revascularization, greater preservation of proprioception, and enhanced graft tendon incorporation. 12
Two studies were performed in which remnant preservation in ACLR showed significantly better synovial coverage and knee stability, although these studies did not find any difference in clinical outcomes between the groups. 25,34 Nakamae et al 34 reported that patients in the ACL augmentation group showed better synovial coverage of the graft on second-look arthroscopy than those in the single- and double-bundle reconstruction groups. Improvement in proprioceptive function was observed in patients with good synovial coverage of the graft. 26 Kondo et al 23 reported that the KT-2000 arthrometer anterior laxity values and results of the pivot-shift test were significantly better in the remnant-tissue preservation procedure than in the remnant-tissue resection procedure. The arthroscopic evaluation showed that the remnant-preserving procedure was significantly better than the remnant-resecting procedure concerning postoperative thickness and apparent tension of the grafts, as well as synovial and fibrous tissue coverage of the grafts. Concerning the clinical outcome, some authors have reported that the advantages of remnant preservation were good functional outcomes and reduced percentage of graft rupture. 20,26,50 However, some meta-analyses have indicated that there is no difference in clinical outcomes between the 2 techniques. 29,52,54 Therefore, controversy remains regarding whether to preserve the remnant during ACLR. 16,20,26,29,43,50,52,54 No consensus has been reached as to whether the remnant-preserved procedure has advantages in bone-graft healing and clinical outcomes in clinical studies. However, to date, most clinical research has focused on the preservation of the tibial attachment sites of the ACL remnant in ACLR without paying much attention to the femoral attachment site of the ACL remnant. In this study, it was noted that preservation of the remnants not only originating from the anatomic attachment of the distal femur but also having a large volume in ACLR had advantages in some patient-reported outcomes as well as in follow-up arthroscopic findings.
This procedure may result in better outcomes for several reasons. First, we preserved remnant tissues at the femoral side as well as the tibial using the remnant preservation technique 21 in ACLR. In previous studies, the preservation of the remnant tissue on the tibial side was important to promote graft healing and improve synovial coverage. However, we believe that preservation of the remnant tissue at the femoral side is also important because mechanoreceptors, including Pacinian corpuscles, Ruffini endings, and Golgi tendon organs, are located at both the femoral and the tibial attachment sites of the ACL. 15,46,63 Second, we speculated that the ruptured ACL remnants connecting the femur to the tibia would improve patient-reported outcomes. When the remnants connect the femur to the tibia, they could play a role in maintaining knee function and stability and accelerating the cellular proliferation and revascularization of the grafted tendon. 12 The tension of the ruptured ACL remnants could maintain mechanoreceptors in the ruptured ACL remnants. 28 Third, it was essential to determine whether the volume of ACL remnants was sufficient for ACLR. Some authors have reported a statistically significant improvement in proprioceptive and functional outcomes in the group with more preserved remnants. 25,26,32 Therefore, it may be expected that the more the femoral remnant is kept intact, continuous, and kept plenty, the better the preservation of proprioceptive outcomes will be.
There has been some apprehension that remnant tissue preservation may increase the occurrence rate of cyclops syndrome or lesions after ACL surgery. 13 The incidence of cyclops syndrome, which shows serious loss of knee extension caused by a hard nodule around the ACL graft, has been reported to range from 2% to 11%. 5,48,55 Webster et al 56 reported that preservation of the tibial stump remnant was not associated with increased rates of surgery for symptomatic cyclops lesions. In the present study, cyclops syndrome was not observed in any of the double-bundle procedures. The incidence of a cyclops lesion, which is a soft fibrous nodule without any clinical symptoms around the graft, has been reported to range from 2% to 47%. 4,9,14,48 Only a few studies have shown that in single-bundle ACLR, there is no significant association between remnant preservation and the presence of a cyclops lesion. 3,9,42,55 In contrast, several investigators 32,34 reported increased symptomatic cyclops lesions with DB-ACLR with remnant tissue preservation. However, Tanabe et al 51 and Kondo et al 25 reported that there is no difference in the incidence of cyclops lesions between remnant-preserving and remnant-resecting ACLR. The present study supports these results. We believe that preservation of ACL remnant tissue does not increase the frequency of cyclops lesions after DB-ACLR.
Limitations
This study has some limitations. First, it had a retrospective design with a relatively small number of patients. Second, evaluations of the remnant and graft were performed retrospectively from the recorded videos. Although we had records of complete surgical procedures, the accuracy of grading based on a video can be limited. Third, we did not measure proprioceptive function in ACLR. Fourth, the mean time from injury to surgery was longer in group NR than the times in groups AA and NA. Some authors have suggested that one of the advantages of early ACLR is that further meniscal or chondral injuries may be avoided, resulting in a faster return to full activities. 6,7 Even though there was no significant difference in the incidence of meniscal and chondral injuries in this study, we consider that delayed ACLR may influence the results of patient-reported outcomes and second-look arthroscopic findings. Fifth, we did not perform radiological and histological assessments of the ACL graft. A previous study reported the usefulness of T1rho and T2 maps in evaluating graft maturation. 61 In addition, a previous study showed that diffusion tensor imaging can be used to image and visualize the structure of ACL grafts. 43 These could be more helpful in assessing the quality of the ACL graft in our surgical procedure. Sixth, we did not have detailed data regarding the return to sports or the difference between preoperative and postoperative activity levels. Therefore, further research and longer follow-up are needed to evaluate the value of preserving ACL remnants.
Conclusion
This study showed that preservation of anatomically positioned and adequate remnant tissue improved graft appearance and the corresponding patient-reported outcomes in DB-ACLR.
Footnotes
Final revision submitted December 30, 2022; accepted January 24, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by JSPS KAKENHI (grant JP 21K16698). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from NTT East Japan Hospital (reference No.19-00469).