
Abstract
Background:
On August 31, 2017, Ohio passed legislation that regulates how opioids can be prescribed postoperatively. Studies have shown that such legislation is successful in reducing the morphine milligram equivalents (MMEs) prescribed after certain orthopaedic procedures.
Purpose:
(1) To determine if the opioid prescription–limiting legislation in Ohio reduced the cumulative MMEs prescribed after hip arthroscopy without significantly affecting the rates of emergency department (ED) visits, hospital readmissions, and reoperations within 90 days postoperatively, and (2) to assess risk factors associated with increased postoperative opioid dosing.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This study included patients who underwent primary and revision hip arthroscopy at a single institution over a 4-year period. The prelegislation (PRE) and postlegislation (POST) groups were defined as patients who underwent surgery before August 31, 2017, and on/after this date, respectively. The Ohio Automated Rx Reporting System was queried for controlled-substance prescriptions from 30 days preoperatively to 90 days postoperatively, and patient medical records were reviewed to collect demographic, medical, surgical, and readmission data. Inverse probability weighting–adjusted mean treatment effect regression models were used to measure the difference in mean outcomes between the PRE and POST cohorts.
Results:
A total of 546 patients (228 PRE, 318 POST) were identified. There was a 25% reduction in the cumulative MMEs prescribed to the POST group as compared with the PRE group during the first 90 days postoperatively (840 vs 1125 MME, respectively; P < .01). The legislation was associated with a significant decrease in the cumulative MMEs prescribed in the first 90 postoperative days (mean treatment effect = –280.6; P < .01), and there were no significant between-group differences in the frequency of ED encounters (8.8% PRE, 11.6% POST; P = .32), hospital readmissions (1.3% PRE, 0.9% POST; P = .70), or reoperations (0.9% PRE, 0.6% POST; P ≥ .99) during this period. Preoperative opioid use was a significant independent risk factor for increased cumulative MMEs in the first 90 days postoperatively (β = 275; P < .01).
Conclusion:
Opioid prescription–limiting legislation in Ohio was associated with significant reductions in opioid MMEs dosing in the 90-day period following hip arthroscopy. This legislation had no significant effect on ED utilization, hospital readmissions, or reoperations within the same period. Preoperative opioid use was a significant risk factor for increased MME dosing after hip arthroscopy.
Approximately 25 million people used opioid pain medications for nonmedical purposes between 2002 and 2011 in the United States alone. 8 This upward trend in consumption has led to an increase in the rate of fatal opioid overdoses, opioid-related emergency department (ED) encounters, and admissions to substance abuse treatment programs. 6 Policy makers within the United States have instituted reasonable prescriber practice changes in many states to reduce the number of circulating opioids. In 2016, Massachusetts became the first state to pass such legislation, and Ohio passed its opioid prescription–limiting legislation on August 31, 2017. 13 This law went into effect immediately after its passage. In Ohio, this legislation states that opioid prescriptions for acute pain (eg, acute postoperative pain) cannot be written for >7 days for adults and that the maximum dose per day cannot exceed 30 morphine milligram equivalents (MMEs). Earlier studies from various states have shown that opioid-limiting legislation has been largely successful in reducing the amount of opioids that are prescribed after certain orthopaedic procedures. 4,14 –18
Although opioid-prescribing legislation has been successful in reducing the amount of opioids that are prescribed postoperatively, the effect of such policy on prescription practices and rates of ED utilization, reoperations, and readmissions after hip arthroscopy is currently unknown. It is important to ascertain this effect for numerous reasons. First, patients aged 20 to 39 years are the most common group to undergo hip arthroscopy, and they have the highest reported rate of illicit drug use. 7,12 Second, in the postoperative period, patients who undergo hip arthroscopy require substantial levels of opioid medications despite advances in regional and general anesthesia. 1,10,20 Third, studies have shown that increased opioid consumption postoperatively is associated with worse outcomes after hip arthroscopy. 3,21 Finally, the most common reason for ED utilization after hip arthroscopy is inadequate pain control. 19
The purpose of this study was 2-fold. The primary purpose was to determine if the opioid prescription–limiting legislation in Ohio reduces the cumulative MMEs prescribed after hip arthroscopy without significantly affecting the rates of ED utilization, hospital readmissions, and reoperations within 90 days postoperatively. The secondary purpose was to assess risk factors associated with increasing opioid dosing postoperatively.
METHODS
Design and Data Collection
Before any data collection, approval for the study was obtained from the institutional review board and the State of Ohio Board of Pharmacy. This retrospective cohort study included patients who underwent primary and revision hip arthroscopy for femoroacetabular impingement syndrome from January 2016 to February 2019 at a single academic tertiary referral center. Patients were identified using an institutional database. Patients were excluded from the final analysis if they carried a diagnosis of hip dysplasia preoperatively and underwent open surgery in conjunction with hip arthroscopy to correct the underlying dysplasia. The remainder of the patients were included.
Patients were categorized into 1 of 2 cohorts based on their dates of surgery. Those who underwent hip arthroscopy before August 31, 2017, (the date when the Ohio law was passed) were placed into the prelegislation (PRE) cohort while patients who underwent surgery on or after that date were placed into the postlegislation (POST) cohort. Patients were also classified as either opioid naïve if they did not have an opioid prescription written within 30 days before surgery or opioid tolerant if they had ≥1 opioid prescriptions written within 30 days before surgery. The electronic medical record of each patient was reviewed to collect demographic, medical, surgical, and readmission data. Operative duration was not collected, as it has not been significantly associated with higher postoperative opioid usage. 7
A query was performed of the Ohio Automated Rx Reporting System (OARRS), the State of Ohio Board of Pharmacy’s prescription drug monitoring program. OARRS is a 5-year rolling database, and data before the 5-year period are expunged from the system daily. Data from OARRS provided by the State of Ohio Board of Pharmacy were deidentified. Controlled-substance prescription data were obtained for all patients from 30 days before surgery to 90 days postoperatively. Information was obtained regarding the type and dose of oral opioid (eg, oxycodone, tramadol, hydrocodone), the number of prescriptions, and the number of pills per prescription. To account for the relative potency of each type of opioid, the dose (in mg) was converted into MMEs using the following multipliers 11 : oxycodone, ×1.5; tramadol, ×0.1; and hydromorphone, ×4. No multipliers were applied to morphine or hydrocodone. The new dosing value was multiplied by the number of tablets within each prescription to obtain the MME for the prescription. The cumulative MMEs were calculated as the sum of the MMEs for each prescription prescribed in the following postoperative periods: immediate (ie, first 7 days), 0 to 30 days, 31 to 60 days, and 61 to 90 days. In addition, we collected data regarding prescriptions of benzodiazepine (eg, diazepam, alprazolam) and gamma-aminobutyric acid (GABA) analog (eg, gabapentin, pregabalin) that were prescribed within 30 days before surgery. In our practice, postoperative pain prescriptions are written postoperatively and before discharge from the ambulatory surgical center.
The data within OARRS are limited to the dates that prescriptions were written/filled and the MME of the entire prescription (if the prescription is for an opioid). The database does not provide insight into the actual consumption habits of the patient. However, we believe that quantifying the number of prescriptions filled and the MME within each prescription serves as a valid proxy for opioid consumption because only 33% of patients dispose of their unused opioid medication. 5
Statistical Analysis
Demographic and comorbidity data were presented using median and interquartile range for continuous variables and frequencies for categorical variables. Some of the covariates of interest were reorganized for meaningful interpretation of regression coefficients. The MMEs in the immediate, 0- to 30-day, 31- to 60-day, and 61- to 90-day postoperative periods were compared between the PRE and POST periods. The Wilcoxon signed-rank test was used to distinguish intracohort differences for preoperative opioid tolerance status, as well as the PRE and POST cohorts. The Kruskal-Wallis equality-of-populations rank test was applied to assess the impact of preoperative opioid tolerance status and legislation.
To evaluate the effect of the opioid legislation itself, inverse probability weighting–adjusted mean treatment effect (ATE) regression models were fitted to correct the imbalance in the distributions of the demographic characteristics and surgical procedures on the potential outcomes in the PRE and POST periods. The ATE measured the difference in mean outcomes between the PRE and POST cohorts. To obtain the ATE estimates, a logistic regression model was first fitted for the PRE group versus the POST group. Demographic characteristics and surgical procedures were included in the logistic model to generate propensity scores. Then the inverse of the propensity scores was used to estimate an inverse probability weighting estimator. Inverse probability weighting–adjusted regression allowed the creation of 2 pseudo-populations with similar baseline clinical characteristics, which can be used to compare the outcomes of 2 groups. We conducted an imbalance check of the propensity score models and evaluated the distribution of the propensity scores to ensure that no outliers were presented.
Multivariate regression analyses were used to identify independent risk factors for increased opioid prescribing postoperatively. These multivariate regression analyses included preoperative opioid exposure and the number of GABA analog and benzodiazepine prescriptions. We could not include demographic factors in the multivariate analyses, as the opioid data from the State of Ohio Board of Pharmacy are completely deidentified. Because of the skewness in the MME data distribution, a quantile regression analysis was applied to MME consumption up to the first 30-day postoperative period and MME dosing in the 0- to 90-day postoperative period. As the result of the zero-inflated nature of prolonged opioid use in the 30- to 90-day postoperative period, we dichotomized this outcome variable. A binary logistic regression analysis was applied to assess factors related to chronic opioid use. In all regression models, the effects of covariates on the outcome variables were adjusted for age, sex, body mass index, and legislation. All tests were 2-sided, and statistical significance was defined as P < .05. Statistical analyses were performed using Stata software (Version 15.0; StataCorp) and R software (Version 3.4.1; R Foundation for Statistical Computing).
RESULTS
Overall, 546 patients were identified, with 228 and 318 patients in the PRE and POST cohorts, respectively (Table 1). The median age of the entire patient population was 27.5 years with the majority being female (71.1%). Most cases were primary hip arthroscopies (92.7%). There were no significant differences between the cohorts with respect to age, sex, body mass index, or medical comorbidities. There were also no significant differences in the frequency of surgical procedures performed during arthroscopy, with the exception of rim recession, which was performed at a significantly higher rate in the PRE cohort relative to the POST cohort (P = .03). Seven patients in the PRE cohort and 97 in the POST cohort were not captured in the OARRS database and were therefore excluded from subsequent analyses.
Preoperative Patient Characteristics and Surgical Procedures a
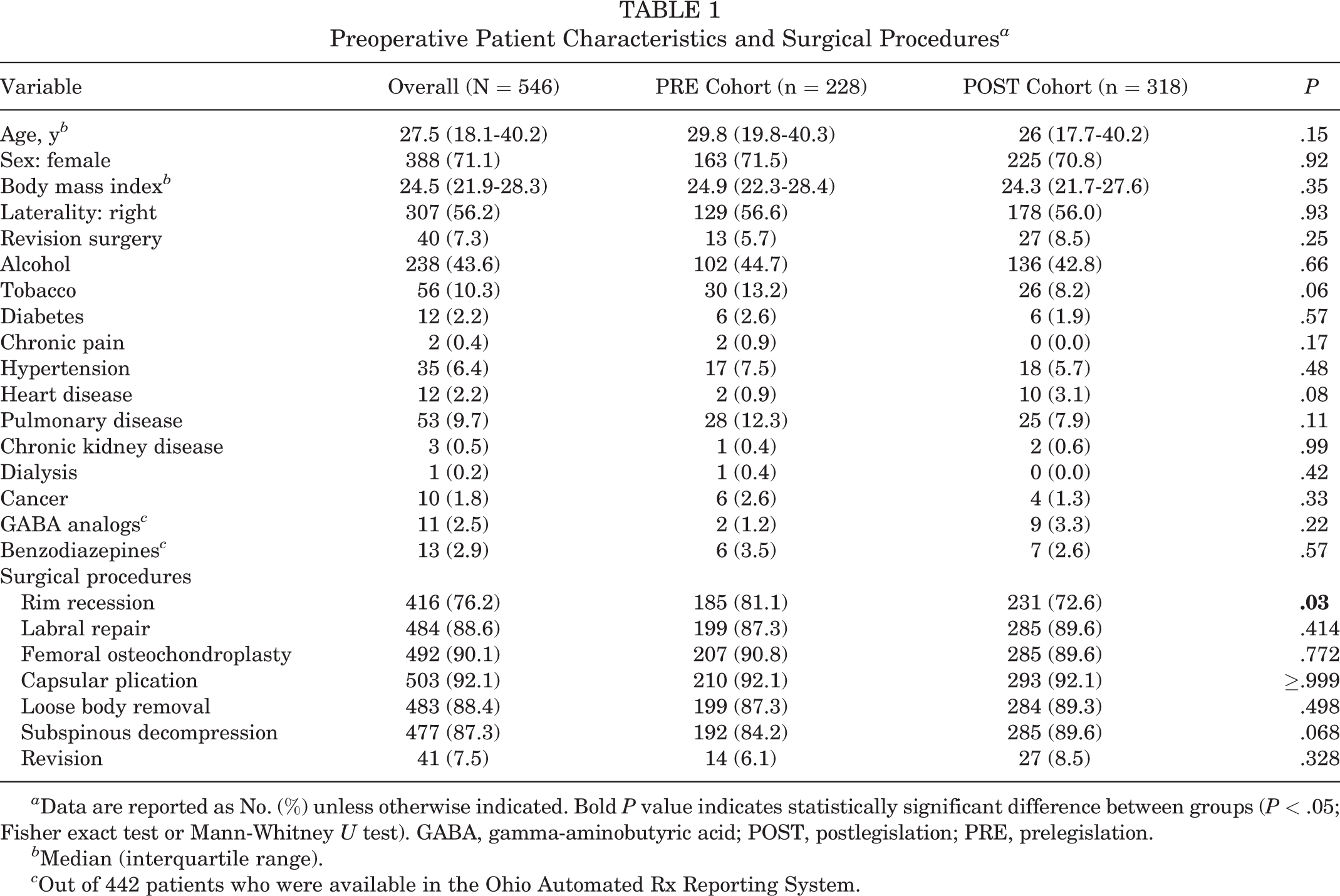
a Data are reported as No. (%) unless otherwise indicated. Bold P value indicates statistically significant difference between groups (P < .05; Fisher exact test or Mann-Whitney U test). GABA, gamma-aminobutyric acid; POST, postlegislation; PRE, prelegislation.
b Median (interquartile range).
c Out of 442 patients who were available in the Ohio Automated Rx Reporting System.
Effects of Legislation on Postoperative Opioid Prescriptions
There was a significant reduction in cumulative MMEs prescribed in the immediate postoperative period (450 PRE vs 337.5 POST; P < .01) and first 30 days (525 PRE vs 375 POST; P < .01) (Figure 1).

Cumulative opioid prescription data per postoperative period stratified by legislation. Data are reported as median [interquartile range]. The Mann-Whitney U test was used to test for significance. MME, morphine milligram equivalent.
Although no significant differences were observed in the MMEs prescribed in the postoperative periods of 31 to 60 days (450 PRE, 315 POST; P = .35) and 61 to 90 days (450 PRE, 337.5 POST; P = .60), there was a significant decrease in cumulative MMEs prescribed throughout the first 90 days postoperatively between the cohorts (1125 PRE, 840 POST; P < .01).
An ATE model was used to determine the effects of the opioid prescription–limiting legislation on the prescribed MMEs postoperatively (Table 2). The legislation was associated with a significant reduction in cumulative MMEs prescribed in 3 postoperative periods: immediate (ATE = –137; P < .01), first 30 days (ATE = –120.6; P < .01), and 0 to 90 days (ATE = –280.6; P < .01).
Mean Treatment Effects of Legislation on Postoperative Opioid Use a

a Inverse probability weighting–adjusted mean treatment effect (ATE) models were performed to evaluate the difference between pre- and postlegislation morphine milligram equivalents. Bold P values indicate statistically significant difference (P < .05).
Effects of Preoperative Opioid Tolerance Status on Postoperative Opioid Prescriptions
Figure 2 illustrates the effects of preoperative opioid use status (ie, opioid naïve vs opioid tolerant) on postoperative opioid prescription. An overall 410 patients were classified as opioid naïve while 32 were classified as opioid tolerant. There was a significant difference in cumulative MMEs prescribed in the first 30 days (450 opioid naïve, 562.5 opioid tolerant; P < .01) and 0 to 90 days (900 opioid naïve, 1181.3 opioid tolerant; P < .01) postoperatively between the opioid-naïve and opioid-tolerant cohorts.
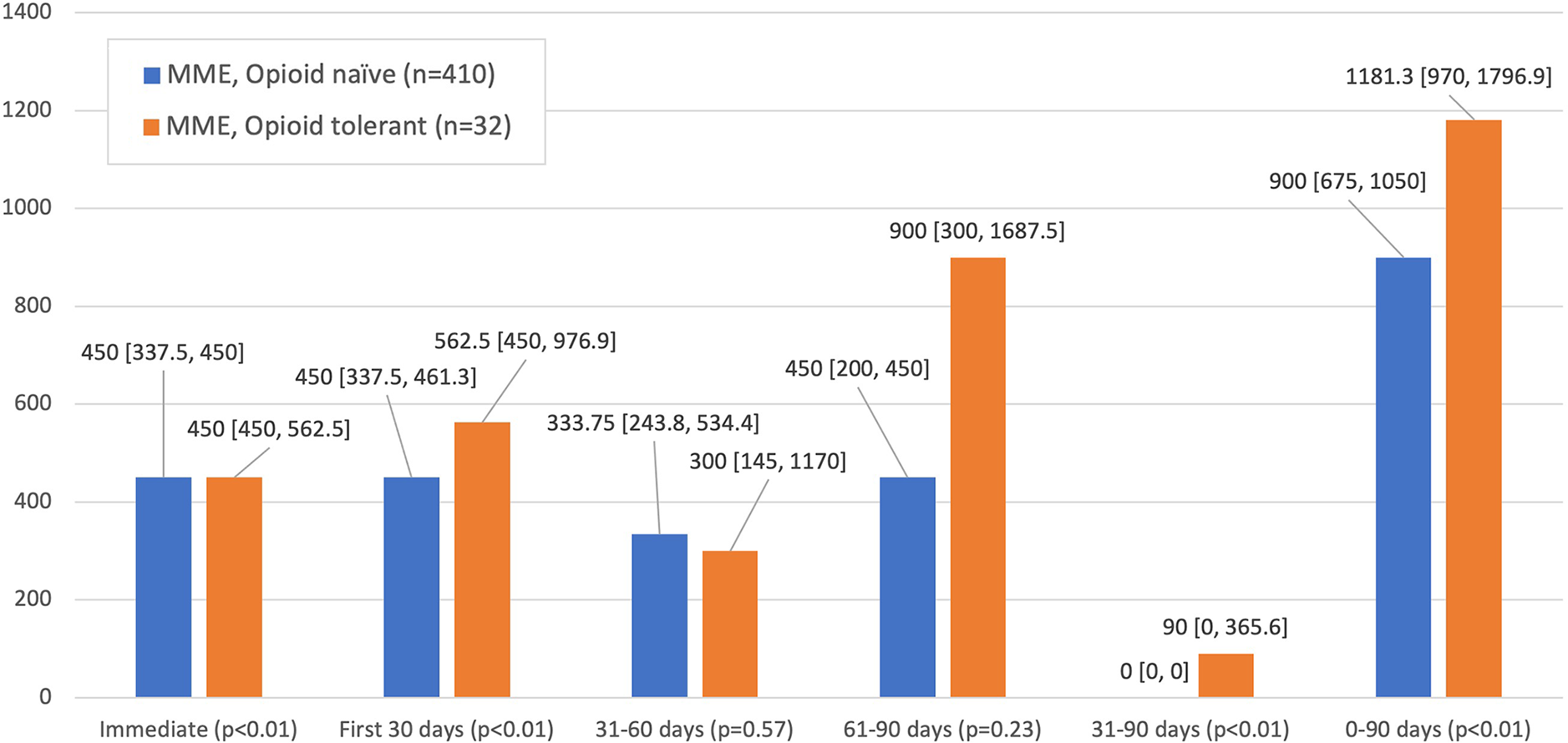
Cumulative opioid prescription data per postoperative period stratified by opioid tolerance. Data are reported as median [interquartile range]. The Mann-Whitney U test was used to test for significance. MME, morphine milligram equivalent.
Combined Effects of Legislation and Preoperative Opioid Status on Postoperative Opioid Prescriptions
The opioid-naïve and opioid-tolerant cohorts were further stratified by the timing of their surgery relative to the passing of opioid prescription–limiting legislation (Table 3). Within the opioid-naïve cohort, 149 and 261 patients were placed into the PRE and POST cohorts, respectively. In the opioid-tolerant cohort, 21 patients were categorized as PRE while 11 were classified as POST. Between the PRE and POST opioid-naïve cohorts, there was a significant reduction in cumulative MMEs prescribed in 3 postoperative periods: immediate (450 PRE, 337.5 POST; P < .01), first 30 days (450 PRE, 337.5 POST; P < .01), and 0 to 90 days (1050 PRE, 810 POST; P < .01). Similarly, the PRE and POST opioid-tolerant cohorts demonstrated a significant decrease in cumulative MMEs prescribed in the immediate postoperative period (562.5 PRE, 450 POST; P < .01). However, no significant decrease was observed in cumulative MMEs prescribed between the PRE and POST opioid-tolerant cohorts in 2 postoperative periods: 0 to 30 days (562.5 PRE, 477.5 POST; P = .07) and 0 to 90 days (1325 PRE, 1080 POST; P = .11).
Cumulative Opioid Prescription Data Stratified by Legislation and Opioid Tolerance a

a Data are reported as median (interquartile range). Bold P values indicate statistically significant differences between PRE and POST (P < .05; Kruskal-Wallis rank test). MME, morphine milligram equivalent; POST, postlegislation; PRE, prelegislation.
Complications
The number of ED encounters, readmissions, and reoperations within the first 30 days postoperatively were compared between the PRE and POST cohorts (Table 4). There were no significant differences in the frequency of ED encounters (8.8% PRE, 11.6% POST; P = .32), hospital readmissions (1.3% PRE, 0.9% POST; P = .70), and reoperations (0.9% PRE, 0.6% POST; P ≥ .99) within 90 days postoperatively between the PRE and POST cohorts.
ED Encounters, Hospital Readmissions, and Reoperations Stratified by Legislation a

a Data are reported as No. (%). ED, emergency department; POST, postlegislation; PRE, prelegislation.
b Fisher exact test.
Risk Factors for Increased Postoperative Opioid Use
Results of the multivariate regression analysis are shown in Table 5. Preoperative opioid tolerance and benzodiazepine tolerance were identified as independent risk factors for opioid use after hip arthroscopy. Preoperative opioid tolerance was a significant independent risk factor for increased cumulative MMEs in 3 postoperative periods: immediate (β = 112.5; P < .01), 0 to 30 days (β = 140; P < .01), and 0 to 90 days (β = 275; P < .01). In addition, preoperative benzodiazepine use was likewise a significant independent risk factor for increased cumulative MMEs at 0 to 30 days (β = 112.5; P = .04). Preoperative GABA analog use was not a significant independent risk factor for increased cumulative MMEs in 3 postoperative periods: immediate (β = 0; P = .99), 0 to 30 days (β = –30; P = .58), and 0 to 90 days (β = –105; P = .33).
Results of Multivariate Regression Evaluating Independent Risk Factors for Postoperative Opioid Use a

a Bold P values indicate statistical significance (P < .05). GAMA, gamma-aminobutyric acid; MME, morphine milligram equivalent.
DISCUSSION
Our results demonstrate that opioid prescription–limiting legislation in Ohio was associated with significant reductions in cumulative MMEs prescribed after hip arthroscopy without significantly affecting the rates of ED utilization, hospital readmissions, and reoperations. In this study, we found significant reductions of 25% and 29% in cumulative MMEs prescribed in the immediate (ie, 0-7 days) and 0- to 30-day postoperative periods, respectively, when comparing the PRE and POST cohorts. A significant decrease was also observed in cumulative MMEs prescribed in the 0- to 90-day postoperative period between the PRE and POST cohorts. However, this reduction was largely attributed to that observed at postoperative 0 to 30 days, as there were no significant differences between the cohorts in cumulative MMEs prescribed at 31 to 60 days and 61 to 90 days. When we accounted for preoperative opioid tolerance, it was apparent that the opioid-tolerant cohort was prescribed more opioids than its opioid-naïve counterparts throughout the postoperative period.
Our finding that opioid-limiting legislation significantly reduces the cumulative MMEs prescribed after hip arthroscopy is congruent with previously published studies. In a series of retrospective studies, Reid et al 15 –17 and Shah et al 18 demonstrated that similar opioid-limiting legislation in Rhode Island was associated with a significant reduction in cumulative MMEs prescribed after an array of orthopaedic procedures, including shoulder and knee arthroscopy, lumbar spine surgery, total joint arthroplasty, and open reduction and internal fixation of distal radius and ankle fractures.
Furthermore, our findings reinforce the well-established relationship between preoperative opioid tolerance and increased prescribing and/or usage of opioids postoperatively. In a retrospective review of a private insurance database, Anciano Granadillo et al 2 demonstrated that the most significant predictor for prolonged opioid use after hip arthroscopy was preoperative opioid use. Likewise, Cunningham et al 7 revealed that any opioid use 2 weeks before surgery was the strongest predictor of opioid use after hip arthroscopy. Finally, Degen et al 9 showed that the risk of persistent opioid use (ie, ≥2 prescriptions filled between 9 and 15 months postoperatively) was greatest in patients who used opioids within 1 year before hip arthroscopy. The relationship between preoperative and increased postoperative opioid consumption is generalizable beyond hip arthroscopy as well. In a retrospective review of 1384 patients undergoing primary total hip or total knee arthroplasty, Benfield et al 4 illustrated that patients with a history of “opioid abuse” received 24.88 MMEs per day more postoperatively when compared with patients without such a history.
Limitations
The outcomes of this study must be interpreted within its limitations. First, this study examined findings from a single academic institution and tertiary referral center, which potentially limits the generalizability of the results. However, surgical residents, physician assistants, and nurse practitioners practicing under the attending surgeons frequently prescribe opioids for acute postoperative pain. Thus, this study highlights the effect of opioid-limiting legislation on the opioid-prescribing practices of many providers. In addition, the findings of this study are consistent with previously published studies. A second limitation is that the OARRS is a 5-year rolling database in which data before the 5-year period are automatically deleted. This ultimately limited the size of our patient population, specifically the PRE cohort.
Third, we did not control for the type of anesthesia that was used during surgery, whether postoperative nerve blocks were utilized, and the use of nonopioid pain medications (eg, nonsteroidal anti-inflammatory drugs) on postoperative opioid-prescribing practices. Fourth, it is possible that the reduction in opioid prescriptions seen in this study and similar studies is not completely attributed to the opioid-limiting legislation, because provider awareness of the opioid epidemic had greatly increased during the same period.
Conclusion
Opioid prescription–limiting legislation in Ohio was associated with significant reductions in opioid MME dosing in the 90-day postoperative period after hip arthroscopy. These reductions were most pronounced in the first 7 days and first 30 days after surgery. This legislation had no significant effect on ED utilization, hospital readmissions, or reoperations within 90 days postoperatively. Preoperative opioid use was a significant risk factor for increased MME dosing after hip arthroscopy.
Footnotes
Final revision submitted December 19, 2022; accepted January 20, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: Y.R. and J.G.I. have received education payments from Rock Medical. R.C.M. has received consulting fees from RTI Surgical, Stryker, and Wright Medical; nonconsulting fees from Smith & Nephew; and royalties from Stryker. S.J.N. has received educational support from Elite Orthopaedics and Stryker and consulting fees and royalties from Stryker. M.J.S. has received education payments from Elite Orthopaedics, consulting fees from Smith & Nephew and Stryker, nonconsulting fees from Smith & Nephew, and honoraria from Fidia Pharma. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Case Western Reserve University (No. STUDY20200623).