
Abstract
Background:
Graft failure after meniscal allograft transplantation (MAT) may necessitate revision surgery or conversion to arthroplasty. A comprehensive understanding of the risk factors for failure after MAT of the knee may facilitate more informed shared decision-making discussions before surgery and help determine whether MAT should be performed based on patient risk.
Purpose:
To perform a systematic review and meta-analysis of risk factors associated with graft failure after MAT of the knee.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
The PubMed, OVID/Medline, and Cochrane databases were queried in October 2021. Data pertaining to study characteristics and risk factors associated with failure after MAT were recorded. DerSimonian-Laird binary random-effects models were constructed to quantitatively evaluate the association between risk factors and MAT graft failure by generating effect estimates in the form of odds ratios (ORs) with 95% CIs. Qualitative analysis was performed to describe risk factors that were variably reported.
Results:
In total, 17 studies including 2184 patients were included. The overall pooled prevalence of failure at the latest follow-up was 17.8% (range, 3.3%-81.0%). In 10 studies reporting 5-year failure rates, the pooled prevalence of failure was 10.9% (range, 4.7%-23%). In 4 studies reporting 10-year failure rates, the pooled prevalence was 22.7% (range, 8.1%-55.0%). A total of 39 risk factors were identified, although raw data presented in a manner amenable to meta-analysis only allowed for 3 to be explored quantitatively. There was strong evidence to support that an International Cartilage Regeneration & Joint Preservation Society grade >3a (OR, 5.32; 95% CI, 2.75-10.31; P < .001) was a significant risk factor for failure after MAT. There was no statistically significant evidence to incontrovertibly support that patient sex (OR, 2.16; 95% CI, 0.83-5.64; P = .12) or MAT laterality (OR, 1.11; 95% CI, 0.38-3.28; P = .85) was associated with increased risk of failure after MAT.
Conclusion:
Based on the studies reviewed, there was strong evidence to suggest that degree of cartilage damage at the time of MAT is associated with graft failure; however, the evidence was inconclusive on whether laterality or patient sex is associated with graft failure.
Meniscal allograft transplantation (MAT) of the knee is performed in young, active patients with meniscal deficiency. Initial studies report improvement in clinical and functional outcomes in appropriately selected patients, from patient satisfaction to delay in the need for conversion to arthroplasty. However, several studies have also demonstrated that there exists a failure rate after these procedures, 7,15,19,25 with rates approaching 55% at the 10-year follow-up. 24
A better understanding of the risk factors for failure after MAT is important, as it may allow for more informed patient selection. Prior factors investigated for their potential association with graft failure include graft mismatch, articular cartilage damage, patient sex, method of graft fixation, and graft laterality. 7,8,18,19,30,34 Despite a substantial increase in the volume of literature reporting on factors associated with graft failure after MAT, these associations are conflicting in many circumstances and therefore remain unclear.
The purpose of the current study was to perform a systematic review and meta-analysis of risk factors associated with graft failure after MAT of the knee. We hypothesized that cartilage status and graft compartment laterality would be associated with an increased risk of graft failure.
Methods
Article Search Process
Articles were extracted in accordance with the 2009 PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement. 21 The query was performed in October 2021 for literature pertaining to graft failure after MAT utilizing the Boolean search phrase “(meniscal allograft transplantation AND (failure) AND ((knee))).” The query was performed using the Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials, PubMed (2008-2019), and OVID/Medline (2008-2019) databases. The protocol for this systematic review and meta-analysis was registered on PROSPERO (ID: 293726).
Article Eligibility
Eligible articles included those written in the English language that reported on clinical outcomes after MAT at any postoperative follow-up period. No minimum follow-up was used to restrict the search, as the primary outcome was all-cause failure after MAT. Included were studies with evidence levels 1 to 3 that directly compared cases and controls or level 4 studies that performed a subanalysis allowing for information necessary to generate odds ratios (ORs). Articles were excluded if failure rates were not evaluated; data were not readily analyzable; populations included pediatric patients; or studies included conference abstracts, narrative or systematic reviews, case reports, technical notes, biomechanical studies, and letters to the editor. Additionally, the references of included articles were cross-referenced for additional investigations that may have been missed in the systematic search.
Quality Assessment
The methodological index for non-randomized studies (MINORS) checklist 13 was used to evaluate the quality of all included studies. The checklist involves 12 items to assess quality, of which 4 are applicable only to comparative studies. The 4 additional criteria specific to comparative groups were used to assess the bias present in articles when selecting cohorts. Each item is scored on a scale of 0 to 2; thus, the maximum MINORS score is 16 for noncomparative studies and 24 for comparative studies. Two reviewers (K.N.K. and R.A.D.) scored each study, and any discrepancies were mitigated by consensus agreement or excluded altogether.
Statistical Analysis
All statistical analyses and related figures were produced via OpenMetaAnalyst, using metafor R console code. 32 A 2-tailed P value <.05 was considered to indicate statistical significance. Risk factors were recorded from each included study, and ORs were calculated from 2-by-2 tables for each study. If risk factors were used to match cohorts 1:1 by exact values, they were not included in the quantitative meta-analysis. Risk factors not amenable to calculation of ORs because of the method of reporting were quantified using mean differences when appropriate. Furthermore, risk factors without sufficient data to perform a meta-analysis were described narratively and excluded from being analyzed quantitatively. DerSimonian-Laird random-effects models were used to determine pooled effect sizes 4 –6 because study heterogeneity was expected given that patient populations were not identical, study designs differed, surgical indications may vary, and surgeon experience has inherent variability.
In accordance with previous recommendations and guidelines for performing meta-analyses from statistical methods literature, a minimum of 2 studies were incorporated into each meta-analysis, as this number is efficient in drawing conclusions from resultant data. 9,11 The pooled effect size was calculated as a weighted average of the effects estimated in the individual studies, with weights representing the amount of information from each study. The 95% CI was used to report all pooled statistics. Heterogeneity was assessed by the P value of chi-square statistics and the I 2 statistic using random-effects models. We regarded heterogeneity as possibly unimportant at an I 2 value <40% and considerable at an I 2 >75%. 14 Risk factors were classified as having strong evidence, moderate evidence, minimal evidence, or marginal to no evidence, according to previously established criteria (Table 1). 28
Risk Factor Strength of Evidence Classifications a

a MAT, meniscal allograft transplantation; OR, odds ratio.
Results
Study Characteristics
After consensus was reached between the 2 reviewers, 17 studies # investigating the outcomes of 2184 patients were included in the final quantitative and qualitative analysis (Figure 1). Eleven (64.7%) studies 1,2,7,8,15 –18,26,29,30 were retrospective cohort studies, while the remaining 6 (35.3%) articles 19,20,24,25,31,34 were case series. The overall pooled prevalence of failure at latest follow-up was 17.8% (range, 3.3%-81.0%). In 10 studies ** reporting 5-year failure rates, the pooled prevalence of failure was 10.9% (range, 4.7%-23%). In 4 studies 17,24,30,34 reporting 10-year failure rates, the pooled prevalence was 22.7% (range, 8.1%-55.0%).
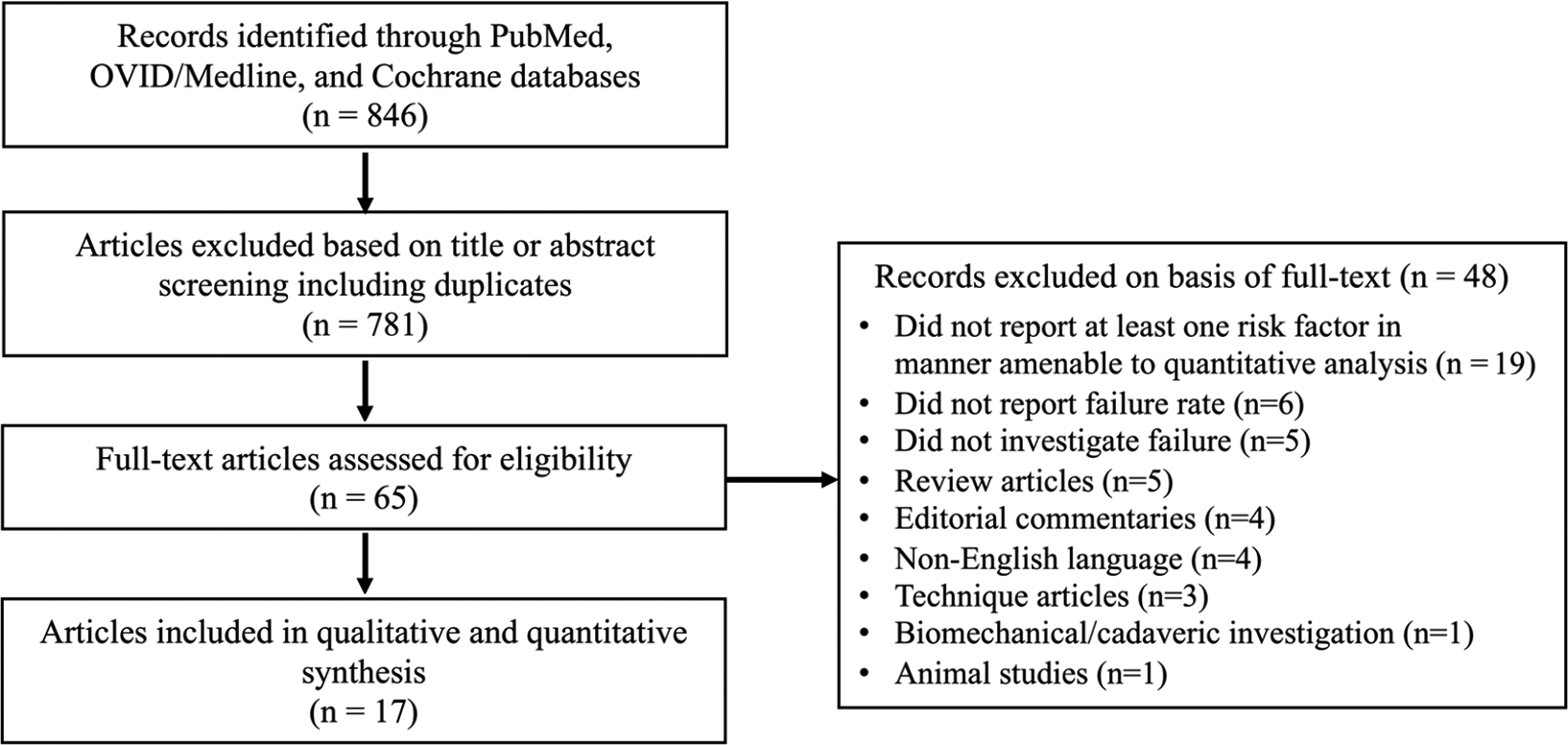
Study selection flowchart.
The overall pooled age and body mass index (BMI) of included patients were 35.1 ± 5.2 years and 25.1 ± 3.9, respectively. The definitions of failure were largely consistent across studies (Table 2) but were generally defined as need for revision MAT or graft removal, meniscectomy, conversion to arthroplasty, or gross appearance of graft failure at second-look arthroscopy.
Characteristics of the Included Studies a

a In all studies, the study population consisted of patients who underwent primary meniscal allograft transplantation (MAT). BMI, body mass index; ICRS, International Cartilage Regeneraton & Joint Preservation Society; IKDC, International Knee Documentation Committee; JSW, joint-space width; LFC, lateral femoral condyle; LOE, level of evidence; LTP, lateral tibial plateau; MRI, magnetic resonance imaging; N, number of patients; OAT, osteochondral autograft transplantation; OCS, Outerbridge cartilage score; TKA, total knee arthroplasty; UKA, unicompartmental knee arthroplasty.
Methodological Quality
The mean (± SD) MINORS score was 16.7 ± 3.9 among all studies (Table 3). For the comparative studies, the mean MINORS score was 20.6 ± 0.7 out of 24. For the noncomparative studies, the mean MINORS score was 12.7 ± 0.7 out of 16.
Methodological Quality of Included Studies as Determined by the MINORS Checklist 13 a
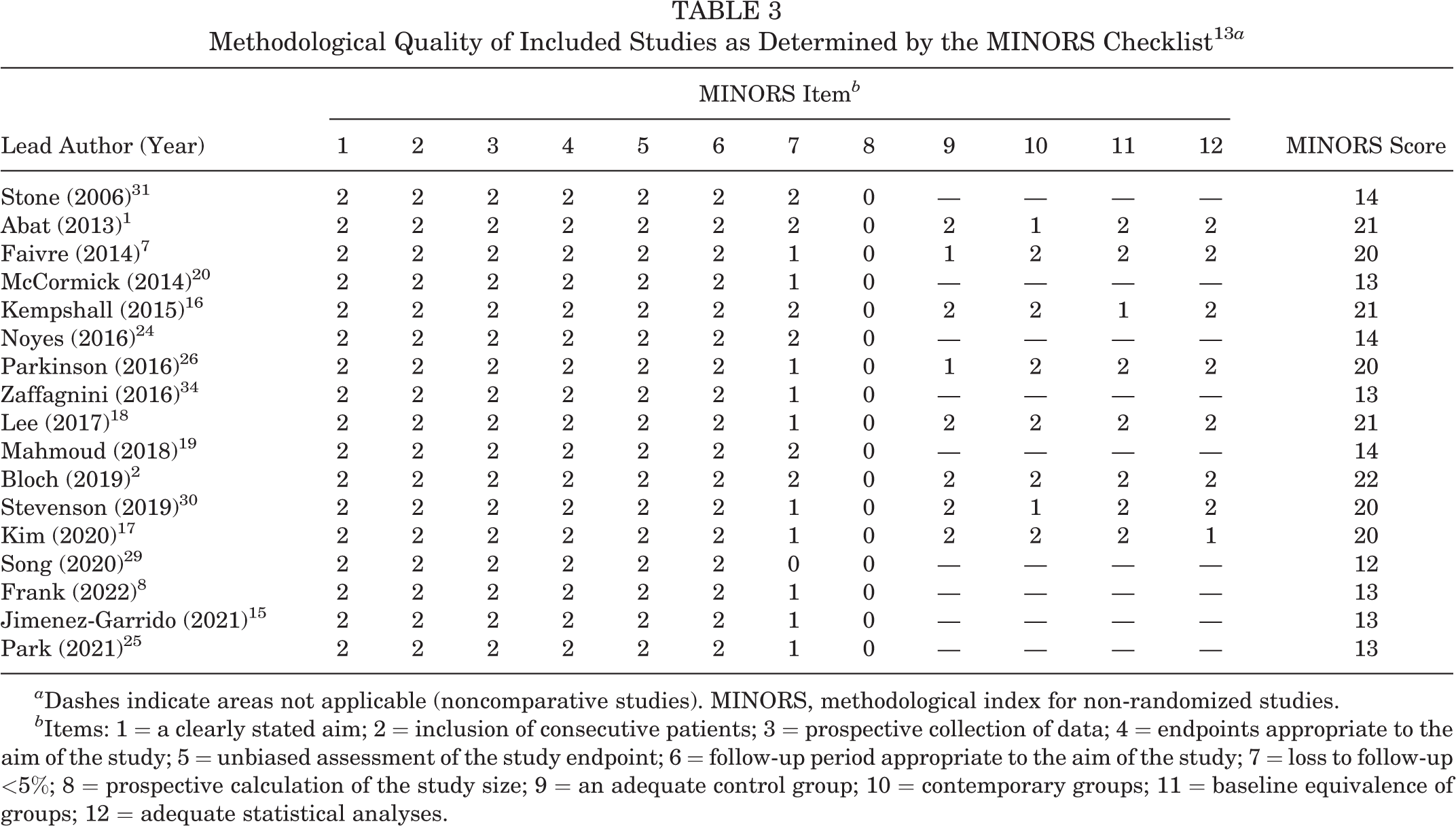
a Dashes indicate areas not applicable (noncomparative studies). MINORS, methodological index for non-randomized studies.
b Items: 1 = a clearly stated aim; 2 = inclusion of consecutive patients; 3 = prospective collection of data; 4 = endpoints appropriate to the aim of the study; 5 = unbiased assessment of the study endpoint; 6 = follow-up period appropriate to the aim of the study; 7 = loss to follow-up <5%; 8 = prospective calculation of the study size; 9 = an adequate control group; 10 = contemporary groups; 11 = baseline equivalence of groups; 12 = adequate statistical analyses.
Risk Factors
A total of 39 risk factors were studied among the 17 included articles. Qualitative analysis was performed when heterogeneity was present or when the risk factor was investigated in <3 studies. A quantitative random-effects meta-analysis was performed in the absence of these conditions. The following associated potential risk factors for graft failure after MAT of the knee were pooled in a meta-analysis as follows: International Cartilage Regeneration & Joint Preservation Society (ICRS) grade, MAT laterality, and sex (Table 4). The remaining risk factors were described narratively (Appendix Table A1). Notably, of the 8 studies 8,17 –19,24,25,29,34 that analyzed age as an independent risk factor, 5 studies 8,17,24,25,34 identified it as noncontributory to graft failure after MAT, whereas 3 studies 18,19,29 implicated age as a risk factor for failure. Of the 3 studies 15,25,34 that analyzed BMI as an independent risk factor, 2 studies 25,34 identified BMI as noncontributory to graft failure after MAT, whereas 1 study 15 implicated it as a risk factor for failure.
Summary Table for Odds Ratios for Failure in Decreasing Order of Strength of Association Derived From Meta-analyses a

a ICRS, International Cartilage Regeneraton & Joint Preservation Society; MAT, meniscal allograft transplant; OR, odds ratio.
ICRS Grade as a Risk Factor for Failure After MAT
Four studies 2,16,18,26 investigated the association between ICRS grade and failure after MAT (Figure 2). The pooled analysis revealed that ICRS grade >3a conferred a significantly higher odds of failure after MAT than ICRS grade ≤3a (OR, 5.32; 95% CI, 2.75-10.31; P < .001). Heterogeneity was considered unimportant (I 2 = 14.3%; P = .32). Based on the results, there was strong evidence to suggest that ICRS grade >3a is an important risk factor for failure after MAT.
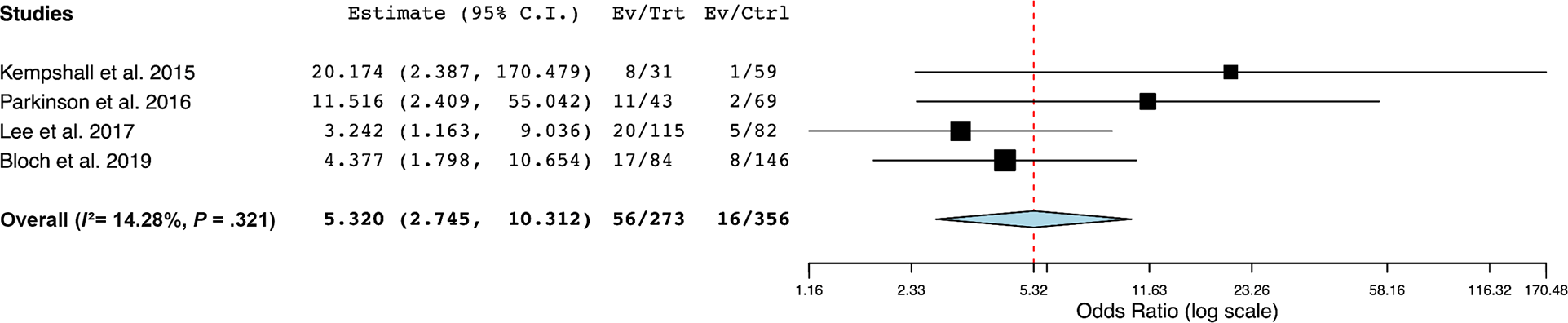
Forest plot demonstrating random-effects meta-analysis for risk factor of International Cartilage Regeneraton & Joint Preservation Society grade. Ctrl, control; Ev, event; Trt, treatment.
Patient Sex as a Risk Factor for Failure After MAT
Three studies 8,19,31 investigated the association between sex and failure after MAT (Figure 3). The pooled analysis revealed that female sex was not significantly associated with failure after MAT compared with male sex (OR, 2.16; 95% CI, 0.83-5.64; P = .12). Heterogeneity was considered unimportant (I 2 = 0.52%; P = .37). Based on the results, there was marginal to no evidence to suggest that female sex is an important risk factor for failure after MAT.

Forest plot demonstrating random-effects meta-analysis for risk factor of sex. Ctrl, control; Ev, event; Trt, treatment.
Graft Laterality as a Risk Factor for Failure After MAT
Six studies 17,19,24,26,31,34 investigated the association between medial versus lateral MAT and failure after MAT (Figure 4). The pooled analysis revealed that medial MAT was not significantly associated with failure after MAT compared with lateral MAT (OR, 1.11; 95% CI, 0.38-3.28; P = .85). Heterogeneity was considered moderate (I 2 = 65.8%; P = .012). Based on the results, there was marginal to no evidence to suggest that graft laterality is an important risk factor for failure after MAT.

Forest plot demonstrating random-effects meta-analysis for risk factor of meniscal allograft transplant laterality. Ctrl, control; Ev, event; Trt, treatment.
Discussion
The main findings of the current systematic review and meta-analysis are as follows: (1) strong evidence was found to support that ICRS cartilage grade >3a at the time of primary MAT is an important risk factor for graft failure after MAT; (2) little to no evidence was found to support that MAT laterality and patient sex were important risk factors for failure after MAT; and (3) numerous risk factors have been investigated in isolation as they pertain to graft failure after MAT for which association and importance remain unknown. Importantly, this is the largest combined cohort studied for patients undergoing MAT, representing increased statistical power derived from more than 2000 primary patients who underwent MAT.
The current study quantitatively analyzed 3 reported risk factors investigated in the literature, ultimately concluding that the presence of ICRS grade >3a increases the risk for graft failure by 532% in certain patients. However, it should be noted that the presence of chondral damage does not necessarily imply impending failure but only that there exists a higher likelihood that the MAT will fail. The ICRS scale defines a grade 3a cartilage defect as when the lesion extends beyond 50% of the cartilage depth, whereas a grade 3b defect is a more abnormal lesion that extends into the calcified layer. 3 This suggests that proposed chondroprotective effects associated with MAT cannot compensate for high-grade cartilage lesions identified at the time of surgery. Furthermore, this suggests that the transition to full-thickness cartilage loss may be associated with MAT failure. Interestingly, we did not identify any studies that compared lower ICRS cartilage grades with ICRS grades ≥3, precluding the analysis of a wider spectrum of cartilage pathology on MAT failure. Parkinson et al 26 reported the outcomes of 125 consecutive patients treated with MAT, reporting that patients with ICRS articular cartilage grades ≤3a had an 85% reduction in the probability of failure compared with patients with severe cartilage damage. Although purely speculation given the current data, it is plausible that since cartilage status is a time-dependent prognostic factor where damage may accumulate over time in the presence of meniscal deficiency, 29 the influence of time from meniscectomy or irreparable meniscal injury to MAT should be considered since expeditious surgery may positively influence graft survivorship. Based on the rates of MAT failure identified in this review, additional procedures may eventually be necessary in select patients, especially in those with high-grade cartilage damage at the time of MAT, as evidenced by ICRS grades >3a.
No significant association was found between patients receiving either a medial or lateral MAT with respect to the risk of graft failure, suggesting that MAT may successfully provide relief regardless of the compartment and their differential congruencies. In the neutrally aligned knee, a greater proportion of force is transmitted through the medial compartment, and therefore one may hypothesize that this could negatively influence graft survivorship. 27,33 On the contrary, 1 study 10 reported that the survival of medial MAT is actually 6 months longer than that of lateral MAT. While this statistical difference does not likely translate to clinical significance, prior literature 12 supports the findings of this meta-analysis that laterality is not associated with graft failure. Therefore, it appears that MAT laterality is a less important consideration in determining optimal surgical candidates for MAT.
In our analysis, patient sex did not demonstrate an association with MAT graft failure, but the literature surrounding the effect of sex on MAT survival is conflicting, with any statistical relationships likely because of poorly powered reports. Frank et al 8 reported that female patients were more likely to undergo revision MAT (1.9% vs 8.4%); however, there were no significant differences in complications or time to reoperation. Interestingly, female patients were more likely to have undergone prior meniscectomy before meniscal transplant compared with male patients, while male patients <40 years of age were more likely to undergo concomitant high tibial osteotomy than female patients of the same age. However, female patients demonstrated greater postoperative patient-reported outcome scores compared with male patients. Parkinson et al 26 reported on the outcomes of 124 patients (one was lost to follow-up), noting that there was no significant difference in rates of graft failure or need for revision surgery between male and female patients. Mahmoud et al 19 also demonstrated in their series of 45 consecutive MAT procedures that sex was not associated with graft survivorship. Despite conflicting results in the literature, the increased statistical power associated with pooling data in the current meta-analysis provides greater clarity into this association and suggests that MAT graft survivorship is not associated with patient sex.
Limitations
The current study is not without limitations. First, the quality of the meta-analysis is a product of the evaluated studies. While standard pooling and analytic techniques were applied to mitigate this risk, the conclusions are limited by the quantity and methodology of the included studies. As an example, only 3 studies were included in the analysis that found patient sex was not a statistically significant risk factor for MAT graft failure. It is important to note that not a single analyzed study included a prospective cohort or randomized controlled trial. Second, several risk factors were not amenable to meta-analysis because of heterogeneity in reporting, and therefore additional risk factors may or may not exist whose effect could not be quantitatively estimated given the current data. Future studies, especially those of higher levels of evidence, are warranted to both establish causation between risk factors and failure and provide more insight into potential risk factors for failure not captured in the current study. Third, publication bias is always a risk with systematic reviews, although all risk factors identified in the current review were reported regardless of whether the association with failure was positive, negative, or neutral.
Several risk factors were noted in the literature although not amenable to formal analysis because of (1) variability in reporting (such as age), (2) infrequent reporting (such as graft under- or oversizing), or (3) reporting associations or lack thereof without presenting data (underreporting). Importantly, this does not indicate that these factors are unimportant but rather that further studies are warranted to clarify these potential associations. Several variably and underreported factors, including age, BMI, and sex, are strongly believed to affect the survivorship of MAT grafts. Furthermore, graft-specific factors, such as fixation method and storage method (ie, fresh-frozen vs cryopreserved), may be important factors associated with graft failure. However, causation is limited in the setting of low-power, retrospective series. Data transparency and reporting therefore become essential because methods that may clarify these relationships, such as meta-analyses and machine learning–based processes, depend on these practices. The finding that only 3 variables among the 39 identified in the MAT literature could be explored quantitatively underscores the need for an improved quality and clarity in reporting the clinical outcomes of MAT. 22,23 This is particularly important when considering the narrow patient selection criteria and high functional expectations accompanying this procedure. This study suggests that emphasis must be placed on reducing the methodological heterogeneity present in MAT research to optimize insight and better guide surgeons and the patients they serve.
Conclusion
There is strong evidence to suggest that degree of cartilage damage at the time of MAT is associated with graft failure; however, based on the current data, there is inconclusive evidence that laterality or patient sex is associated with graft failure.
Footnotes
Notes
Final revision submitted December 2, 2022; accepted January 17, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: P.N.R. has received consulting fees from Pacira Pharmaceuticals. J.C. has received education payments from Arthrex and Smith & Nephew; consulting fees from Arthrex, DePuy, ConMed Linvatec, Ossur, Smith & Nephew, and Vericel; speaking fees from Linvatec; and hospitality payments from Stryker. B.U.N. has received grant support from Arthrex; education payments from Arthrex and Smith & Nephew; and consulting fees from Stryker, Wright Medical, and Zimmer Biomet; and has stock/stock options in BICMD. R.J.W. has received research support from Histogenics; consulting fees from Arthrex, JRF Ortho, and Lipogems; royalties from Arthrex; and hospitality payments from Stryker; and has stock/stock options in MICMD, Cymedia, Engage Surgical, Gramercy Extremity Orthopedics, Pristine Surgical, and RecoverX. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Appendix
Qualitative Analysis of Risk Factors With Data Not Amenable to Meta-analysis a

| Lead Author (Year) | Risk Factor | Findings |
|---|---|---|
| Descriptive/Clinical | ||
| Park (2021) 25 | Age | Not associated with graft failure (OR, 1.0; 95% CI, 0.9-1.1; P > .05) |
| Kim (2020) 17 | Age | Not associated with graft failure (P = .77) |
| Lee (2017) 18 | Age | Significantly associated with graft failure (HR, 1.095; 95% CI, 1.039-1.154; P = .001; 9.5% increase in graft failure per each additional year of age) |
| Noyes (2016) 24 | Age | Age >30 y not associated with graft failure (P > .05) |
| Mahmoud (2018) 19 | Age | Age >35 y significantly associated with increased risk of graft failure (P < .05) |
| Frank (2022) 8 | Age | Age ≥40 y not associated with graft failure (P > .05) |
| Song (2020) 29 | Age | Age ≥43 y significantly associated with increased risk of graft failure (P = .01), which became insignificant after controlling for cartilage status and time from previous meniscectomy |
| Zaffagnini (2016) 34 | Age | Age >50 y not associated with graft failure (P > .05) |
| Park (2021) 25 | Sex | Not associated with graft failure (OR, 1.2; 95% CI, 0.2-8.7; P > .05) |
| Kim (2020) 17 | Sex | Not associated with graft failure (P = .22) |
| Park (2021) 25 | BMI | Not associated with graft failure (OR, 0.7; 95% CI, 0.5-81.1; P > .05) |
| Jimenez-Garrido (2021) 15 | BMI | BMI ≥30 significantly increased risk of graft failure (HR, 11.8; 95% CI, 1.5-91.4; P < .05) |
| Zaffagnini (2016) 34 | BMI | BMI ≥25 not associated with graft failure (P > .05) |
| Park (2021) 25 | Time from meniscectomy | Not associated with graft failure (OR, 1.0; 95% CI, 0.9-1.1; P > .05) |
| Stone (2006) 31 | No. of prior surgeries | Greater number of surgeries significantly associated with increased risk of graft failure (P = .012) |
| McCormick (2014) 20 | Subsequent procedures | Significantly associated with increased risk of graft failure (OR, 8.4; 95% CI, 1.6-43.4; P = .007) |
| Procedural/Intraoperative | ||
| Park (2021) 25 | Concomitant cartilage procedures | Not associated with graft failure (P > .05) |
| Noyes (2016) 24 | Concomitant cartilage procedures | Significantly associated with increased risk of graft failure at 7 y (P < .05) |
| Kim (2020) 17 | Concomitant cartilage procedures | Not associated with graft failure (P = .72) |
| Kim (2020) 17 | Concomitant ligamentous procedures | Not associated with graft failure (P = .30) |
| Kim (2020) 17 | Concomitant osteotomy procedures | Not associated with graft failure (P = .30) |
| Stone (2006) 31 | Any concomitant procedure | Not associated with graft failure (P = .20) |
| Zaffagnini (2016) 34 | Any concomitant procedure | Not associated with graft failure (P > .05) |
| Park (2021) 25 | Allograft coverage of chondral defect | Significantly associated with increased risk of graft failure (OR, 20.5; 95% CI, 1.8–2872.4; P = .011) |
| Stevenson (2019) 30 | MAT sizing | MATs undersized by >5 mm had an increased risk of mechanical failure (OR, 5.66; P = .046) |
| Lee (2017) 18 | High-grade bipolar cartilage damage | Significantly associated with increased risk of graft failure (OR, 3.56; 95% CI, 1.272-9.967; P = .016) compared with low-grade chondral degeneration |
| McCormick (2014) 20 | MAT laterality | No significant differences in failure between medial, lateral, or bicompartmental MAT (P = .61) |
| Stone (2006) 31 | Allograft material (fresh-frozen vs cryopreserved) | Not associated with graft failure (P > .05) |
| Faivre (2014) 7 | Open vs arthroscopic MAT | Open vs arthroscopic MAT not associated with graft failure (P > .99) |
| Abat (2013) 1 | Suture-only vs osseous-only fixation | Suture-only vs osseous-only fixation not associated with graft failure (P > .05) |
| Imaging | ||
| Park (2021) 25 | LTP chondral defect size >3 cm2 on MRI | Significantly associated with increased risk of graft failure (OR, 28.3; 95% CI, 2.5–4006.7; P = .004) |
| Park (2021) 25 | LFC defect size | Significantly associated with increased risk of graft failure (OR, 3.3; 95% CI, 1.4-11.6; P = .005) |
| Park (2021) 25 | LTP defect size | Significantly associated with increased risk of graft failure (OR, 2.3; 95% CI, 1.1-7.5; P = .026) |
| Park (2021) 25 | Mechanical axis deviation on radiograph | Not associated with graft failure (OR, 1.2; 95% CI, 0.9-2.0; P > .05) |
| Kim (2020) 17 | Mechanical axis deviation on radiograph | Not associated with graft failure (P = .31) |
a BMI, body mass index; HR, hazard ratio; LFC, lateral femoral condyle; LTP, lateral tibial plateau; MAT, meniscal allograft transplantation; MRI, magnetic resonance imaging; OR, odds ratio.