
Abstract
Background:
Rates of return to preinjury level of play after anterior cruciate ligament (ACL) reconstruction (ACLR) remain unsatisfactory, particularly for patients who undergo revision surgery. Psychological readiness is associated with successful return to sport (RTS) and self-perceived preinjury sport performance.
Purpose:
To compare psychological readiness at RTS between patients who underwent revision ACL autograft reconstruction and matched controls who underwent primary ACL autograft reconstruction.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Data were gathered using a single orthopaedic surgeon database of patients who underwent ACLR between 2015 and 2018. Patients who underwent revision ACLR and met the study criteria (N = 92) were matched by age, sex, graft type, and rehabilitation protocol to a control group of patients who underwent primary ACLR (n = 92). Functional assessment at release to play was examined using passive knee range of motion, single-leg squat, and single-leg hop testing. Self-reported outcomes included the International Knee Documentation Committee subjective function survey and the ACL–Return to Sport after Injury (ACL-RSI) psychological readiness scale. Time to release to play was recorded as the number of months needed to reach a ≥90% limb symmetry index from the date of the index ACLR. Data were assessed for normality using the Shapiro-Wilk test, and univariate general linear models were utilized with an alpha level of .05.
Results:
The overall mean patient age was 29.9 ± 10 years, and 40% of patients were women. No significant differences between groups were noted in any of the baseline patient characteristics or surgical findings. At RTS, the mean ACL-RSI score was significantly lower in the revision surgery group (77.4 ± 19.4 vs 85.3 ± 17.4; P = .011). In addition, the revision surgery group returned to play significantly later than the primary surgery group (9.4 ± 2 vs 8.1 ± 1.3 months, respectively; P < .001).
Conclusion:
When compared with primary ACL autograft reconstruction, revision reconstruction patients exhibited lower psychological readiness scores and a longer time to meet the objective criteria for RTS.
Registration:
NCT03704376 (ClinicalTrials.gov identifier).
Keywords
The common goal for many athletes undergoing anterior cruciate ligament (ACL) reconstruction (ACLR) is to return to their preinjury level of sport participation. 25 However, rates of return to preinjury level of play after ACLR remain unsatisfactory, particularly for those undergoing revision procedures. 2,3 Psychological readiness is associated with successful return to sport (RTS) and self-perceived preinjury sport performance. 4,5,10,11,13,18,23,29 Conversely, research suggests that half of high school and collegiate athletes identified fear of reinjury as a significant factor in choosing not to RTS after ACLR. 18
Psychological factors appear to have lasting consequences, as athletes reporting higher fear of reinjury have lower RTS rates for up to 7 years after surgical reconstruction. 4,14 In contrast, athletes who successfully return to their preinjury level of participation often exhibit more positive responses to psychological outcome measures, including higher knee-related quality of life, 11 greater self-reported patient satisfaction, 5 and lower fear-avoidance behaviors when compared with those who are unable to return to their preinjury participation level. 12,22 Furthermore, greater psychological readiness during rehabilitation appears to be a significant predictor of return to the previous level of sporting performance. 29
For patients who RTS, the risk of a second ACL injury after ACLR has been reported 9,10,17 to be as high as 33%. The implications of these high retear rates on psychological readiness and RTS after revision ACLR have yet to be fully elucidated in the current literature. Considering the association between psychological readiness and successful RTS, the purpose of this study was to compare psychological readiness and functional outcomes between patients who underwent revision autograft ACLR and matched controls who underwent primary autograft ACLR. Our hypothesis was that patients who underwent revision reconstruction would exhibit lower psychological readiness scores, longer time to meet the objective functional criteria, and longer time to RTS compared with patients who underwent primary autograft reconstruction.
Methods
Study Design
After receiving institutional review board approval for the study protocol, we conducted a retrospective, matched case-control study after reviewing a single orthopaedic surgeon database of 1273 patients who underwent a primary or revision ACLR between 2015 and 2018. This study was conducted in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology statement 27 and was registered with Clinicaltrials.gov (NCT03704376).
Participants
Patients were included if they were between the ages of 15 and 50 years and had undergone revision ACLR with bone–patellar tendon–bone, contralateral patellar tendon (PT), quadriceps tendon (QT), or hamstring (HS) tendon autograft. Exclusion criteria were meniscal transplant, bicruciate ligament injury, allograft reconstruction, staged revision procedures, malignancy, fracture, or infection. A total of 92 patients met the study's inclusion criteria. These patients were matched by age, sex, graft type, rehabilitation protocol, and preinjury level of sport participation (Marx score) to a control group of 92 patients who underwent primary ACLR. 8,29 As part of a larger ongoing cohort study, all patients were monitored until they successfully completed the release-to-play functional objectives established at our institution. A flowchart of the patient inclusion process is shown in Figure 1. Informed consent was provided by participants.

Strengthening the Reporting of Observational Studies in Epidemiology diagram of patient inclusion. ACL, anterior cruciate ligament; ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury; MARX, Marx Activity Rating Scale.
Surgical Procedure and Rehabilitation Protocol
An anatomic single-bundle ACLR was performed as previously described 6 with an autologous PT graft, a free QT graft, or an autologous HS tendon. The femoral tunnel was drilled independently through the accessory anteromedial portal within the center of the native ACL footprint. 7 The anteromedial tibial tunnel was drilled retrograde with a RetroReamer (Arthrex) through the residual tibial footprint. 1 The femoral and tibial sides of the graft were secured with an interference screw or over a 6.5 × 25–mm post. Before tibial fixation, the graft was tensioned between 10 and 20 N, cycled 15 times, and retensioned again if necessary. Once the graft was tensioned, the arthroscope was inserted into the joint to assess for wall and roof impingement.
A standardized, criterion-based rehabilitation protocol was initiated on postoperative day 1 as described by Worsham et al. 30 The protocol is guided by phased progressions contingent on tissue healing timelines and physical performance measures that entail an immediate weightbearing progression, progressive knee range of motion, and programs aimed at lower extremity strength and agility. While compliance was not tracked, standardized patient follow-up with the orthopaedic surgeon at 4- to 6-week intervals and associated criterion-based physical performance measures were tracked through RTS.
Return to Sport
Functional assessment at release to play was gauged according to passive knee range of motion, single-leg balance, 20,21 and single-leg hop for distance. 16 Time to release to play for both patient groups was recorded as the number of months needed to reach a limb symmetry index of ≥90% between operative and nonoperative limbs from the date of the index ACLR.
Patient and Surgical Characteristics
Patient and surgical characteristics were acquired from an ongoing database (REDCap Version 12.04.0; Vanderbilt University) and from the patient medical record. Variables obtained for between-group comparisons included graft type, meniscal injury location, and number of sutures utilized for repair. The prevalence of meniscal injury locations was categorized into 3 levels: (1) isolated medial meniscus; (2) isolated lateral meniscus; (3) or both medial and lateral meniscus. The number of meniscal sutures for all repairs was also included to quantify the relative size of the repair. Data on partial meniscectomies, including the amount of tissue removed, were not accounted for in the present study. Patient-reported outcomes were assessed with the International Knee Documentation Committee 13 subjective function survey and the ACL–Return to Sport after Injury (ACL-RSI) psychological readiness scale. 28
Self-reported Psychological Measure
The ACL-RSI is a 12-item instrument utilized to assess an athlete’s psychological readiness to RTS and evaluates emotions, confidence, and risk appraisal. 28 The ACL-RSI is scored from 0 to 100, with 0 indicating an extremely negative psychological response (ie, increased fear of reinjury, decreased confidence). 20 Each of the 12 items on the measure is rated on an 11-point scale, with responses ranging from “extremely” to “not at all.” The ACL-RSI has documented validity, internal consistency, high construct validity, and high test-retest reliability. 28
Statistical Analysis
An a priori power analysis was performed using G*Power (Version 1.3, Heinrich-Heine-Universität Düsseldorf) to determine an adequate sample size according to previously published work by Ardern et al, 3 which compared ACL-RSI scores of 209 patients. Based on these results and the anticipation of a moderate effect size (d = 0.5), a 1-tailed alpha of .05, and a power of 0.80, the estimated sample size was 62 participants per group for a total of 134 patients. Data are reported as means and standard deviations for continuous variables or absolute values and frequencies for categorical variables. Data were assessed for normality using the Shapiro-Wilk test. The independent Student t test was used for continuous data and the chi-square test was used for categorical data to examine baseline differences in patient and surgical characteristics. Univariate (group) general linear models were used to calculate differences in their ACL-RSI and performance of release-to-play testing at the time of release. An a priori alpha of .05 was statistically significant for between-group comparisons. All statistical analyses were performed with SPSS Statistics (Version 24; IBM Inc) statistical software.
Results
No differences were noted in any baseline patient characteristics or surgical findings between the primary and revision surgery groups (Table 1). At RTS, the revision surgery group had a significantly lower ACL-RSI score than the primary group (77.4 ± 19.4 vs 85.3 ± 17.4; P = .011). However, no other objective performance or self-reported functional differences were observed between the 2 groups (Table 2). Additionally, the revision surgery group returned to play significantly later than the primary surgery group (9.4 ± 2 vs 8.1 ± 1.3 months, respectively; P < .001).
Patient and Surgery Characteristics a
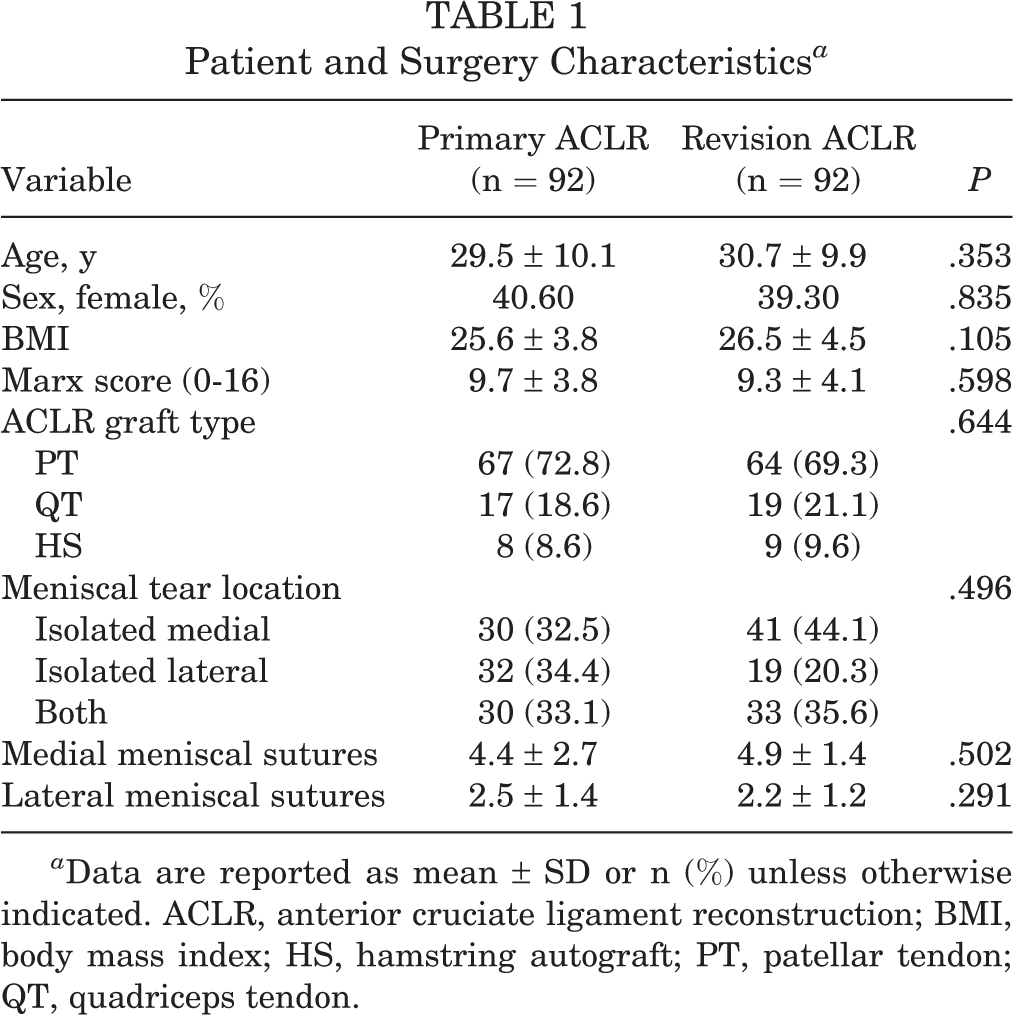
a Data are reported as mean ± SD or n (%) unless otherwise indicated. ACLR, anterior cruciate ligament reconstruction; BMI, body mass index; HS, hamstring autograft; PT, patellar tendon; QT, quadriceps tendon.
Functional Performance at Release to Play a

a Values are reported as mean ± SD. Bold P values indicate statistically significant differences between groups (P ≤ .05). ACLR, anterior cruciate ligament reconstruction; ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury; IKDC, International Knee Documentation Committee; LSI, limb symmetry index.
Discussion
The study results confirmed our hypothesis that patients who undergo revision autograft reconstruction will exhibit lower ACL-RSI scores, delayed time to meet objective functional criteria for RTS, and longer time for release to RTS when compared with patients who undergo primary ACLR.
Although the mean difference in the ACL-RSI was statistically significant, it did not exceed the smallest detectable change of ±17 points, 25 calling into question the clinical relevance of these results. Despite not exceeding the smallest detectable change threshold, these differences are consistent with the results of previous research 15,24 comparing self-reported outcomes, objective functional performance, and RTS rates between primary and revision ACLR. Therefore, we encourage further investigation to elucidate the potential clinical differences in psychological readiness for these patient groups. Perhaps more importantly, we recommend that further research be conducted to investigate the effectiveness that various cognitive behavioral therapies and physical training strategies may have on this psychological construct.
The mean ACL-RSI scores for both groups in our study met or exceeded a recently reported 12-month postoperative cutoff score of 77 that corresponded to a 90% sensitivity for athletes to sustain a second ACL injury. 19 Prior research also has indicated that ACL-RSI scores improve over time, particularly for athletes who return to competitive sport. 15 Sadeqi et al 24 evaluated athletes who successfully returned to sport at 2 years postoperatively and reported a mean ACL-RSI score of 72 at 1-year follow-up and 81.6 at 2-year follow-up; the ACL-RSI scores in the present study at RTS (85.3 for primary surgery, 77.4 for revision surgery) are consistent with those in the study by Sadeqi et al and suggest that athletes may be able to achieve sufficiently high ACL-RSI scores after revision ACLR surgery.
It is relevant to note that graft selection differences are present in our study compared with currently published work on psychological readiness to RTS. In contrast to the current literature utilizing the ACL-RSI after HS autograft ACLR, the majority of patients in the present study received PT or free QT tendon autografts. These graft selection differences may affect the generalizability of proposed RTS cutoff scores to the PT/free QT population. 18,24 Additionally, research has suggested that athletes with PT autografts may require a prolonged time to meet clinical rehabilitation and RTS criteria when compared with those with allografts or HS autografts. 26 However, our research demonstrated that both patients with primary and revision PT autografts took less time to meet RTS criteria (8.1 ± 1.3 and 9.4 ± 2 months, respectively). More research is needed to determine the impact of graft selection on psychological readiness of athletes returning to sport. As we seek to understand the overall recovery process, it is important to consider that psychological readiness and ACL-RSI scores may improve at a variable rate throughout rehabilitation. For example, ACL-RSI scores in those with PT autografts may potentially lag behind those with other graft types early in the rehabilitation process secondary to anterior knee pain, but they ultimately demonstrate similar or higher ACL-RSI scores at mid- and long-term follow-up than those with other graft types. As surgical trends continue to evolve, appraising the multifaceted aspects of recovery is critical. Based on the results of the present study, it is evident that comparisons of rehabilitation timeframes, clinical outcomes, and psychological readiness at different postoperative stages are important in improving the rehabilitation process.
Limitations
There are limitations to this study that should be considered when examining these results. The study was retrospective, and we used a single orthopaedic surgeon database with a highly integrated rehabilitation program that included repeated testing examinations for our subjective and objective functional testing criteria. While this process supports a consistent patient experience, rehabilitation structure, and testing procedure, it may limit the generalizability of our results to other studies. Additionally, we did not isolate these comparisons to a single graft source. Future studies should consider including sample sizes that adequately represent any potential differences between various autograft sources in a prospective manner to confirm these results.
Conclusion
Patients with revision ACL autograft reconstruction exhibited lower psychological readiness scores and longer time to meet the objective criteria when assessed at RTS when compared with patients with primary autograft reconstruction. Serial monitoring of psychological readiness during the rehabilitation process may improve outcomes for RTS in patients undergoing revision ACLR and identify those at risk for being unable to successfully RTS.
Footnotes
Acknowledgment
The authors thank Jena-Claire Auten, PT, DPT, PhD, and Natalie L. Myers, PhD, ATC, for manuscript preparation. Part of this work was presented at the APTA Combined Sections Meeting in February 2021.
Final revision submitted October 10, 2022; accepted November 15, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded intramurally through the Memorial Hermann Health System. W.L. has received consulting fees from DJO; speaking fees and royalties from Arthrex; and hospitality payments from Linvatec. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Texas Health Science Center of Houston (ref No. HSCMH-14-0734).