
Abstract
Background:
Anterior cruciate ligament (ACL) injuries are common sports-related injuries with a high risk of reinjury after return to sport (RTS). Rehabilitation aims to regain symmetrical knee strength and function to minimize the risk of a second ACL injury after RTS.
Purpose:
To determine the effect of absolute quadriceps and hamstring strength, normalized by body weight, on the risk of a second ACL injury during the first 2 years after RTS in patients who have undergone ACL reconstruction (ACLR).
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Data from patients after index ACLR at the time of RTS were extracted from a rehabilitation registry—Project ACL. Patients who had performed isokinetic tests for quadriceps and hamstring strength and hop tests before RTS were included. The endpoint was a second ACL injury or a follow-up of 2 years after RTS after ACLR.
Results:
A total of 835 patients (46% women), with a mean age of 23.9 ± 7.7 years, were included. During the study period, 69 (8.3%) second ACL injuries (ipsilateral and contralateral) occurred. Greater relative quadriceps strength in the injured leg increased the risk of a second ACL injury (relative risk [RR], 1.69 [95% CI, 1.05-2.74]; P = .032). In patients who had recovered symmetrical quadriceps strength (limb symmetry index ≥90%), there was no effect of quadriceps strength on the risk of second ACL injury (RR, 1.33 [95% CI, 0.69-2.56]; P = .39). Quadriceps strength on the healthy side or hamstring strength, regardless of side, had no effect on the risk of a second ACL injury.
Conclusion:
Greater relative quadriceps strength in the injured leg at the time of RTS after ACLR was associated with an increased risk of a second ACL injury. There was no effect of relative quadriceps strength on the risk of a second ACL injury in patients who had recovered symmetrical quadriceps strength.
The results from tests of muscle function are used in clinical practice to help determine whether patients are ready to return to sport (RTS) after anterior cruciate ligament (ACL) reconstruction (ACLR). These test results are commonly reported as the limb symmetry index (LSI), which expresses the recovery of the injured knee with regard to the noninjured knee. 14,29,42 Passing RTS criteria are often set when achieving an LSI of ≥90% in a battery of muscle function tests. 16,41,42
A second ACL injury is, unfortunately, a concern after an ACLR 31 and can be the reason for an athlete’s deciding to end one’s career. 25,40 The collected evidence on the effect of symmetrical muscle function in a battery of tests before RTS on risk for second ACL injury is inconclusive. 3,16 However, patients treated with an ACLR often struggle to achieve RTS criteria in a battery of muscle function tests before RTS, 42 where passing rates are as low as 23% before RTS. 41 Despite several studies reporting differences in RTS passing rates, 14,33,41,42 as well as in the timing of RTS 1 –3,7,16,22,24,28,34 after ACLR, there are still patients who do not recover symmetrical muscle function before RTS. 41
There are concerns about the use of the LSI to evaluate muscle strength, as it only considers limb-to-limb symmetry and does not account for absolute muscle strength or absolute muscle strength normalized by body weight, that is, relative strength. It is yet to be determined whether greater relative quadriceps and hamstring strength has a protective effect on sustaining a second ACL injury. The purpose of this study was to evaluate the role of relative quadriceps and hamstring strength on the risks of (1) a second ACL injury, (2) an ACL graft rerupture, and (3) a contralateral ACL injury in patients after primary ACLR followed by RTS.
Methods
Study Design
This study was performed according to the REporting of studies Conducted using Observational Routinely-collected health Data statement, 5 which is an extension of Strengthening the Reporting of Observational Studies in Epidemiology. 39 This was a prospective cohort study based on data from an observational rehabilitation outcome registry—Project ACL. The Project ACL registry, located in Gothenburg, Sweden, was begun in 2014 to improve the care of patients with ACL injuries. 18 Participation in Project ACL is voluntary, and patients are able to withdraw at any time. Patients are provided with written information about the project and informed consent is obtained. In Project ACL, patients are regularly assessed using validated patient-reported outcome measurements and a battery of tests for muscle function. Follow-ups are scheduled as follows: 10 weeks; 4, 8, 12, and 18 months; 2 and 5 years; and then every fifth year after ACL injury or reconstruction. Project ACL received ethics approval from the Swedish Ethical Review Authority. Patients or the public were not involved in the design, conduct, reporting, or dissemination plans of this study.
Test Battery
The assessments in Project ACL comprise validated tests for quadriceps and hamstring strength and 3 hop tests: vertical hop, hop for distance, and 30-second side hop. The tests of muscle function are supervised by registered physical therapists trained in standardized testing procedures. Hop testing starts at 4 months after ACLR if patients are deemed to be “ready” (have practiced a maximum hop test similar to the test procedure with their responsible physical therapist) by their responsible physical therapist. Hop tests were not used in this study.
In the present study, patients followed Project ACL test procedures and were instructed to warm up according to a standardized procedure previously published, 32 consisting of 10 minutes on a stationary bicycle and submaximal trials on each test. Strength testing was performed in a seated position on an isokinetic dynamometer (Biodex System 4; Biodex Medical System) at an angular speed of 90 deg/s. Three maximal trials were performed with 40 seconds of rest between each trial and the maximum torque in newton meters was recorded and registered in Project ACL. The Biodex System has an intraclass correlation coefficient of 0.95 for measuring isokinetic strength in the quadriceps and the hamstring muscle groups. 11
Patient-Reported Outcome Measures
We used the Tegner activity scale to determine RTS. The questionnaire is completed at each follow-up to assess the requirements of the knee. The Tegner is a numerical rating scale used to assess the level of knee-strenuous activity. 38 The physical demands gradually increase for every increased level of the Tegner scale, where the Tegner activity level 10 is defined as the most knee-strenuous activity with participation in elite-level sports (football or rugby). 38 The original scale ranges from 0 to 10, where a score of 0 represents being on sick leave. However, Project ACL uses a modified version of the Tegner scale that starts at level 1 (sedentary work). 4 RTS in this study was defined as a Tegner score ≥6 (ie, returning to knee-strenuous sport).
Study Patients
Patients registered in Project ACL, aged 15 to 50 years with a primary ACL injury, treated with primary ACLR and rehabilitation, and with a preinjury activity level of at least 6 on the Tegner scale were eligible for inclusion. Patients who had not performed strength tests at the time of RTS or had not returned to a Tegner score ≥6 were excluded. Previous publications reported a Tegner score ≥6 as a proxy for athletic exposure that puts patients at risk for a second ACL injury. 3
Data Collection
Demographic characteristics and relative strength data from the test closest in time to that at which patients had returned to a Tegner score ≥6 (ie, RTS) were extracted for analysis on April 23, 2021. This means that for a patient who returned to sport at 9 months, we used test results from 8 months, whereas if a patient returned to sport at 11 months, we used the test results from 12 months. Data from strength tests of quadriceps and hamstrings were normalized by body weight in kilograms (ie, N·m/kg) 19 as measured at the time of testing.
Outcome Measures
The primary outcome was the occurrence of a second ACL injury, defined as a graft rupture of the surgically reconstructed ACL or a contralateral ACL injury. The endpoint was set as a second ACL injury or a follow-up of 2 years after RTS after ACLR. The second ACL injury was determined by a registered “new ACL injury” to a patient’s profile in Project ACL, added either by the patients themselves or the treating physical therapist. Relative strength as a risk factor for a second ACL injury was determined by analyzing the relative risk (RR) of a second ACL injury for every 1 N·m/kg increase in relative strength at the time of RTS. Patient characteristics, including sex, age at the time of ACLR, preinjury Tegner score, and time to RTS were used as confounders in a multivariable analysis, alongside relative quadriceps and hamstring strength. Secondary outcome variables were ACL graft rupture and contralateral ACL injuries.
Statistical Analysis
Statistical analyses were performed with the SAS Statistics for Windows (Version 9.4; SAS Institute). Demographic data were recorded as mean values with standard deviations and medians with ranges. For a comparison of characteristics between sexes, the Mantel-Haenszel chi-square exact test was used for ordered categorical variables. The Fisher nonparametric permutation test was used for continuous variables.
The impact of relative strength on the occurrence of a second ACL injury was presented as the RR with 95% CI for risk estimates and P values. The P values were estimated using generalized linear models with a binomial distribution and log-link function. Univariable and multivariable analyses with confounders were used to determine the effect of relative strength on a second ACL injury. In addition, we performed sensitivity analyses using symmetry (LSI ≥90%) in quadriceps or hamstring strength. The P value and RR are based on a continuous analysis of the original values from strength tests and their increase of 1 N·m/kg and not on stratified groups presented in Table 2 or the Supplemental Material available for this study. Cumulative incidence curves are given for the time from RTS to the second ACL injury. All of the tests were 2-sided and conducted at the 5% significance level.
Results
There were 2622 patients in Project ACL on April 23, 2021, of whom 835 patients (46% women) were included. Figure 1 presents the inclusion process.

Flowchart of patient inclusion and exclusion. ACL, anterior cruciate ligament; Tegner, Tegner activity scale.
The included patients had a mean age of 23.9 ± 7.7 years and a body mass index of 23.6 ± 2.7 at index ACLR. On average, patients returned to sport at 10.2 ± 5.5 months after ACLR. A hamstring tendon autograft was the most commonly used autograft for ACLR (81.8%). Table 1 presents patient characteristics stratified by sex. Demographic characteristics and patient differences regarding second ACL injury are presented in Supplemental Table S1.
Characteristics of the Study Patients Stratified by Sex a

a Data are presented as n (%) for categorical variables and as mean ± SD and median (range) for continuous variables. Bold P values indicate statistically significant differences between groups (P < .05). BMI, body mass index; RTS, return to sport.
b The Mantel-Haenszel chi-square exact test was used for ordered categorical variables, the chi-square exact test was used for nonordered categorical variables, and the Fisher nonparametric permutation test was used for continuous variables.
Risk of a Second ACL Injury
A total of 69 (8.3%) patients reported a second ACL injury during the first 2 years after RTS. There were 47 (68%) ipsilateral ACL graft ruptures and 22 (32%) contralateral ACL injuries. Of the 69 second ACL injuries, 53 (77%) were sustained during the first year after RTS—39 (76%) ipsilateral and (3.8%) contralateral.
Figure 2 illustrates the cumulative incidence of a second ACL injury based on relative quadriceps strength for the ACL-reconstructed side. The analyses adjusted for patient sex, age at index surgery, time to RTS (months), and preinjury Tegner score on the relative quadriceps strength of the ACL-reconstructed side resulted in a 1.69 times greater risk of a second ACL injury for every 1 N·m/kg increase in relative strength during the first 2 years after RTS (RR, 1.69 [95% CI, 1.05-2.74]; P = .032) (Table 2). Relative strength had no effect on the risk of a second ACL injury for either quadriceps strength on the noninjured side or hamstring strength on either side.

Cumulative incidence of a second ACL injury after RTS, stratified by relative quadriceps strength on the ACL reconstructed side. ACL, anterior cruciate ligament; RTS, return to sport.
Relative Risk of Second ACL Injury for Every 1 N·m/kg Increase in Relative Strength a
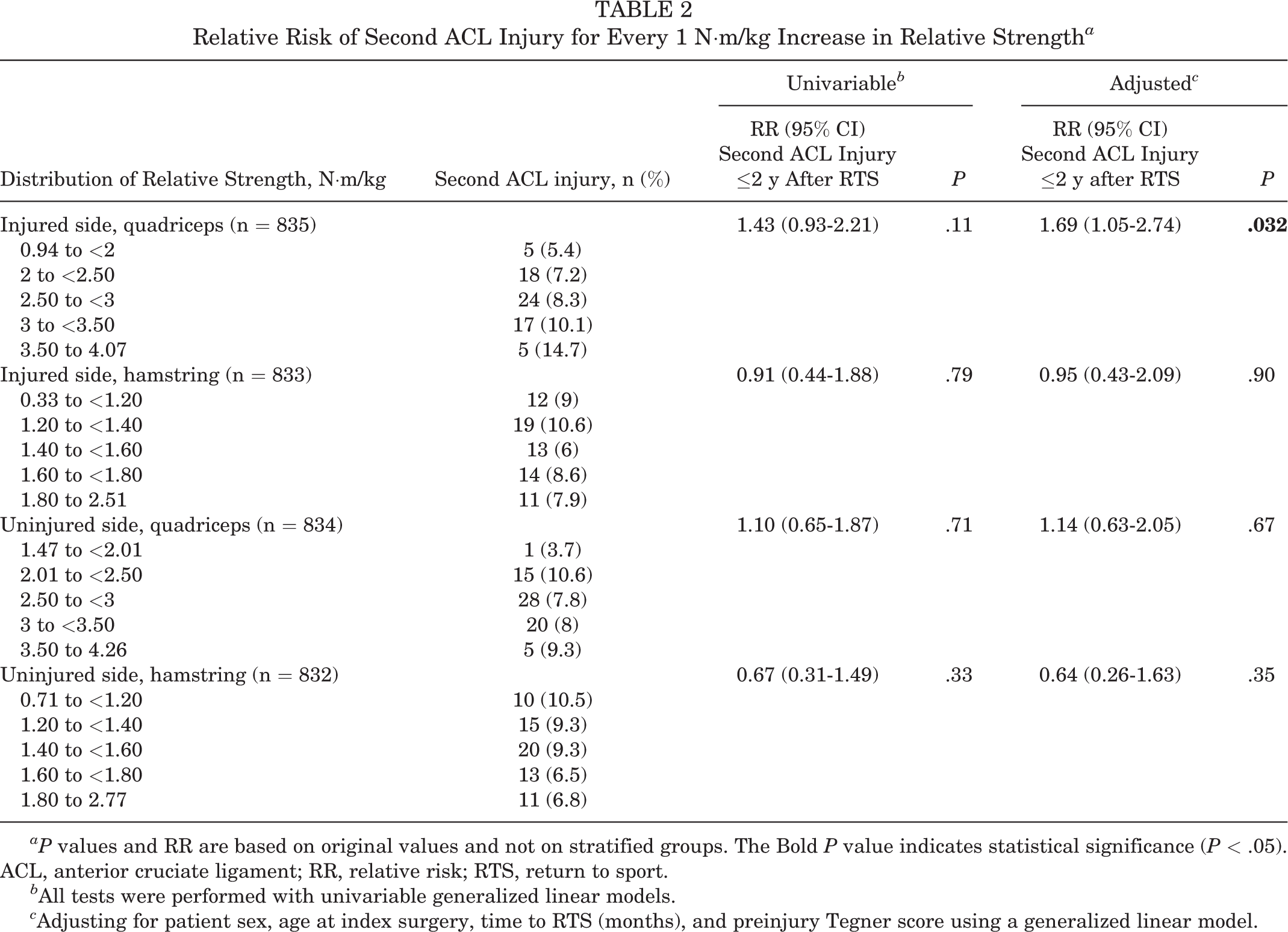
aP values and RR are based on original values and not on stratified groups. The Bold P value indicates statistical significance (P < .05). ACL, anterior cruciate ligament; RR, relative risk; RTS, return to sport.
b All tests were performed with univariable generalized linear models.
c Adjusting for patient sex, age at index surgery, time to RTS (months), and preinjury Tegner score using a generalized linear model.
Sensitivity analyses were performed on the significant finding of a greater risk of a second ACL injury for every 1 N·m/kg increase in relative quadriceps strength on the ACL-reconstructed side (Supplemental Table S2). Relative quadriceps strength had no effect on the risk of a second ACL injury when accounting for symmetrical quadriceps strength (1.33 [95% CI, 0.69-2.56]; P = 0.39).
Risk of ACL Graft Rupture and Contralateral ACL Injury
Increased relative quadriceps or hamstring strength had no effect on the risk of ACL graft rupture or contralateral ACL injury after RTS in patients after a primary ACLR (Supplemental Tables S3 and S4). A multivariable analysis was not possible to perform because of the small number of contralateral ACL injuries. Figure 3 presents the cumulative incidence of ipsilateral graft rupture and contralateral ACL injury.
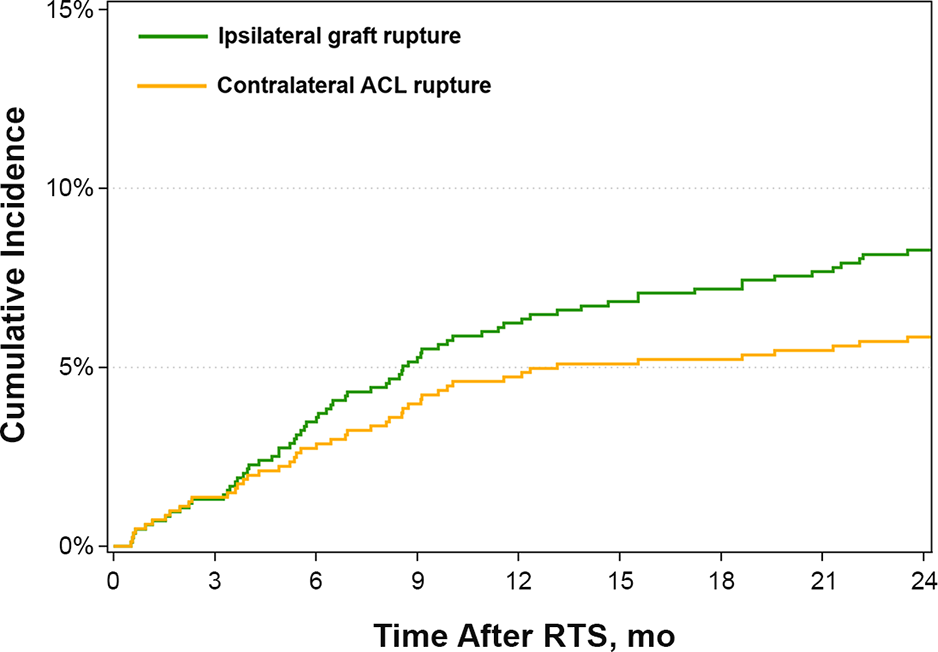
Cumulative incidence of ipsilateral graft rupture and contralateral ACL rupture after RTS. ACL, anterior cruciate ligament; RTS, return to sport.
Discussion
The main finding in this study was an increased risk of a second ACL injury with every 1 N·m/kg increase in relative quadriceps strength on the ACL-reconstructed side when accounting for differences in patient age, sex, preinjury activity level, and time to RTS. However, when adjusting for symmetrical quadriceps strength, there was no effect of relative quadriceps strength on the risk of a second ACL injury. This supports the importance of recovery of both preoperative absolute muscle strength and LSI to minimize the risk of second injury in patients before RTS after ACLR. In addition, increased relative quadriceps or hamstring strength had no effect on a second ACL injury on the ipsilateral or contralateral knee alone.
Risk of a Second ACL Injury
The study findings indicated that for every 1 N·m/kg increase in relative quadriceps strength on the ACL-reconstructed side, the risk of a second ACL injury increased 1.69 times when accounting for patient characteristics and time of RTS, which adds a new perspective to the complexity of a second ACL injury. Although the exact mechanisms behind our results cannot be determined by this study, our results indicate that the stronger the patients’ quadriceps on the ACL-reconstructed side are, normalized by body weight, the greater the risk of a second ACL injury. During sports, when athletes contract their quadriceps muscle, an anterior translation of the tibia is induced, which imposes a strain on the ACL. 17 Sagittal plane control has recently been shown to play an important role during sporting tasks where limited impact absorption through the hip and trunk and a more asymmetrical center of mass through the knee in the sagittal plane can increase loading through the knee. 8,20,21 Our results may be explained by the patients’ being able to expose their knees to greater forces without being fully recovered, that is, not being able to handle the induced excessive strain on their ACLs. This is supported by the fact that relative quadriceps strength in patients with a symmetrical quadriceps strength had no effect on second ACL injury, suggesting that these patients may be better prepared for RTS or have a better capacity in the reconstructed knee to cope with the forces during sports participation. In addition, no significant effect was found for hamstrings strength on the risk of a second ACL injury. As the hamstrings are believed to play a role in rotatory stability and act to limit excessive tibial anterior translation, 36 a reduced absolute hamstring strength relative to body weight may influence the risk for second ACL injuries. However, no effect was found in our results.
Although there is conflicting evidence on the effectiveness of RTS testing, 26 the current proposed RTS criteria 14,16 are based on limb-to-limb symmetry, that is, achieving an LSI ≥90% to be defined as ready to RTS, 27 which is believed to have a protective effect on the risk of sustaining a second ACL injury. In contrast, Bodkin et al 6 presented results suggesting an increased risk for a second ACL injury with 2.1% for every 1% increase in quadriceps strength symmetry at 6 months for patients who return to activity <8 months after ACLR. Our sensitivity analysis showed that our finding of increased risk for second ACL injury was no longer present in patients who had symmetrical strength. One concern about recovering symmetry after ACLR is whether it is achieved by a strength decrease in the nonreconstructed leg, thereby masking bilateral weakness. 42 However, when interpreting our results, the recovery of symmetrical quadriceps strength after ACLR appears to eliminate the association between increased quadriceps strength and risk for a second ACL injury. In addition, we acknowledge that strength deficits have been associated with more severe knee-related symptoms, 10,35,44 which suggests that encouraging patients to increase their strength as part of recovering symmetrical function is advised.
Risk of ACL Graft Rupture and Contralateral ACL Injury
The overall rate of a second ACL injury in the present study appears to be lower compared with a previous study—8% versus 15% to 25%. 30 Previous results from a systematic review showed a greater rate of contralateral injuries as second ACL injuries, 12% contralateral versus 8% ipsilateral ACL injuries, during a 51-month follow-up after ACLR. 43 Our findings suggest a greater rate of ipsilateral graft rupture as a second ACL injury, 6% ipsilateral versus 3.8% contralateral, during the first 2 years after RTS following ACLR. The difference in ipsilateral graft rupture or contralateral injury as a second ACL injury may be due to different periods of follow-up, 24 months after RTS in our study versus 51 months after ACLR in the systematic review, 43 as other researchers have suggested that ipsilateral graft ruptures are more common during the first 2 years after RTS following ACL reconstruction. 9
Our results revealed no significant effect of relative quadriceps or hamstring strength on the risk of either an ACL graft rupture or a contralateral second ACL injury when analyzed separately 2 years after RTS following ACLR. Future studies on risk factors for ipsilateral and contralateral secondary ACL injuries separately are therefore warranted; however, this requires a larger cohort of patients sustaining a second ACL injury. The present study was underpowered to perform multivariable analyses for contralateral second ACL injury.
Strengths and Limitations
In this study, we analyzed the risk of a second ACL injury in patients after primary ACLR. The use of a rehabilitation registry provided a large cohort of 835 patients who underwent ACLR, increasing generalizability to the population of patients returning to a physical activity level corresponding to a Tegner score ≥6 after ACLR and enabling sensitivity analyses with known confounders. Although we had a large number of eligible patients for inclusion, a considerable number of patients were excluded, as they had not returned to sport or had not attended the follow-ups in Project ACL.
The definition of RTS used in our study was a Tegner score ≥6, which means that some patients may not have returned to their preinjury level of activity or may have returned to sport in the early stage of rehabilitation. As the Tegner is self-reported, patients in our cohort who had a preinjury activity level ≥6 may have returned to a more knee-strenuous activity than other patients and were therefore exposed to a greater risk of a second ACL injury. It is also worth mentioning that there were no patients in our cohort who sustained a second ACL injury before returning to Tegner activity level 6. In addition, the Tegner score accounts for neither time of exposure nor the intensity of physical activity, which are known to influence the risk of a second ACL injury, 15 especially if the increase in load/exposure exceeds the patient’s knee capacity. 12,13 This is especially important considering the greater rate of a second ACL injury that occurred during the first year after RTS compared with the second year. Furthermore, the test analyzed in this study was the test closest in time to RTS, which means that there may be a difference in time between RTS and time of testing between patients, and quadriceps strength may also differ because of this time gap, which could have led to an over- or underestimation of quadriceps strength at the time of RTS.
Since the reasons for a second ACL injury are multifactorial, we acknowledge that there might be other measurements of muscle function and surgical techniques 37 that could help explain the risk of a second ACL injury 23 that were are not accounted for in this study. To account for the risk of type 1 error, we presented confidence intervals for every analysis.
Conclusion
Greater quadriceps strength in the injured leg at the time of RTS after ACLR was associated with an increased risk of a second ACL injury. In patients who had recovered symmetrical quadriceps strength, there was no effect of relative quadriceps strength on the risk of a second ACL injury.
Supplemental material for this article is available at http://journals.sagepub.com/doi/suppl/full/10.1177/23259671231157386#supplementarymaterials
Supplemental Material
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671231157386 - Effect of Quadriceps and Hamstring Strength Relative to Body Weight on Risk of a Second ACL Injury: A Cohort Study of 835 Patients Who Returned to Sport After ACL Reconstruction
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671231157386 for Effect of Quadriceps and Hamstring Strength Relative to Body Weight on Risk of a Second ACL Injury: A Cohort Study of 835 Patients Who Returned to Sport After ACL Reconstruction by Rebecca Simonson, Ramana Piussi, Johan Högberg, Carl Senorski, Roland Thomeé, Kristian Samuelsson and Eric Hamrin Senorski in Orthopaedic Journal of Sports Medicine
Footnotes
Acknowledgment
Special thanks to Bengt Bengtsson at Statistiska Konsultgruppen for assistance with the statistical analysis.
Final revision submitted November 15, 2022; accepted January 1, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: R.S. received salary support from the Local Research and Development Council of Gothenburg and Södra Bohuslän. K.S. is a board member of Getinge AB. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Swedish Ethical Review Authority (ref No. 2020-02501).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.