
Abstract
Background:
There is a paucity of literature reporting outcomes after revision hip arthroscopic surgery in obese patients.
Purpose:
To report the minimum 5-year survivorship, patient-reported outcomes (PROs), clinical benefit, and risk factors for conversion to total hip arthroplasty (THA) in obese patients after revision hip arthroscopic surgery.
Study Design:
Case series; Level of evidence, 4.
Methods:
Data were prospectively collected and retrospectively reviewed for patients who underwent revision hip arthroscopic surgery by a single surgeon between April 2010 and August 2016. Inclusion criteria were a body mass index ≥30 and baseline and minimum 5-year postoperative values for the modified Harris Hip Score (mHHS), Nonarthritic Hip Score (NAHS), Hip Outcome Score–Sport-Specific Subscale (HOS-SSS), and visual analog scale (VAS) for pain. Exclusion criteria were Tönnis grade >1 and hip dysplasia. Survivorship was defined as no conversion to THA. Clinical benefit was measured using the minimal clinically important difference (MCID). Survivors and nonsurvivors underwent further bivariate and regression analyses to determine the predictors of conversion to THA.
Results:
Included were 24 hips in 24 patients. The mean patient age was 39.3 ± 12.7 years, and the mean follow-up was 83.9 ± 26.5 months. The survivorship rate was 75.0%, and patients demonstrated a significant improvement in all PROs (P < .01). At 5-year follow-up, the MCID for the mHHS, NAHS, HOS-SSS, and VAS was achieved by 70.6%, 94.1%, 92.9%, and 64.7%, respectively, of the patients. Older age, higher grade ligamentum teres tears, and acetabuloplasty were significant on bivariate analysis for conversion to THA, and increased age was identified as a significant variable for conversion to THA on regression analysis (odds ratio, 1.297 [95% CI, 1.045-1.609]; P = .018), with a 29.7% greater risk for every additional year of age at the time of revision.
Conclusion:
In this study, 25.0% of obese patients who underwent revision hip arthroscopic surgery required conversion to THA. The study patients who did not need conversion to THA had a significant improvement in all PROs, with >90% achieving MCID for one or more outcome measures. Older age was identified as a significant predictor of conversion to THA.
Outcome data support hip arthroscopic surgery for the treatment of femoroacetabular impingement syndrome (FAIS). 4,26 Kyin et al 17 reported significant improvements in several patient-reported outcomes (PROs) in patients who underwent primary hip arthroscopic surgery at midterm to long-term follow-up.
Over half of the adults in the United States have at least 1 chronic disease, including obesity. 36 The adult obesity rate in the United States increased from 13.4% in 1962 to 39.8% in 2016, currently affecting over 93.3 million adults aged ≥20 years. 11 Patients with a body mass index (BMI) ≥30 (considered as obese) have demonstrated improvements in outcomes at short-term and midterm follow-up after hip arthroscopic surgery. 30 Despite consistent improvements in PROs after hip arthroscopic surgery, meaningful improvements are negatively influenced by a greater BMI. 15 Furthermore, BMI has been established as a positive predictor of conversion to total hip arthroplasty (THA) after hip arthroscopic surgery. 10 This is a finding that has been consistently reported in the current literature. 31 Kuroda et al 16 reported that conversion to THA and complication rates were 2.4 and 3.2 times higher, respectively, in the obese population compared to the nonobese population. Nevertheless, these findings pertain almost exclusively to primary hip arthroscopic surgery.
Patient selection errors, patient-related factors, and technical issues play a role in failed hip arthroscopic procedures. 20 Although improvements in PROs and clinical benefit can be achieved in the revision setting, 8,33 the relative risk for conversion to THA has been determined to be 2.6 times higher than in the primary scenario at midterm follow-up. 21
Obesity and revision hip arthroscopic surgery are indeed predictors of a higher rate of conversion to THA 10 ; however, data on this disadvantageous combination are scarce. The purpose of the present study was to report the survivorship, PROs, clinical benefit, and risk factors for conversion to THA in an obese patient population after revision hip arthroscopic surgery. It was hypothesized that at a minimum 5-year follow-up, (1) a high rate of conversion to THA would be reported, (2) a significant improvement in all PROs would be reported in patients who did not need to convert to THA, and (3) the rate of those who achieve the minimal clinically important difference (MCID) would be low.
Methods
Patient Selection
Institutional review board approval was received for the study protocol. Data from a single institutional database were prospectively collected and retrospectively reviewed on all patients who had undergone hip arthroscopic surgery by the senior surgeon (B.G.D.) between April 2010 and August 2016. Patients were considered eligible if they had a BMI ≥30 (defined as obese 16 ). Patients included in the study had preoperative (prerevision) and minimum 5-year postoperative PRO scores. Patients were excluded from the study if they had Tönnis grade >1 hip osteoarthritis; had hip conditions such as avascular necrosis, ankylosing spondylitis, Ehlers-Danlos syndrome, Legg-Calve-Perthes disease, pigmented villonodular synovitis, or slipped capital femoral epiphysis; had hip dysplasia (lateral center-edge angle [LCEA] <18°) 22 ; or were unwilling to participate.
Participation in American Hip Institute Hip Preservation Registry
All study patients consented and participated in the American Hip Institute hip preservation registry. This study presents novel findings, but the data of some patients may have been used in previous studies.
Preoperative Evaluation and Indications for Revision Hip Arthroscopic Surgery
All study patients had no improvement after undergoing 3 months of nonoperative treatment such as activity modification, nonsteroidal anti-inflammatory drugs, physical therapy, intra-articular ultrasound-guided injections, and rest and had pain interfering with daily activities before the senior surgeon (B.G.D.) recommended them as candidates for revision hip arthroscopic surgery. The senior author (B.G.D.) evaluated all surgical candidates by conducting an extensive patient history, physical examination, and radiographic imaging review. Magnetic resonance arthrograms (1.5 T) were also reviewed for all patients.
During the physical examination, variables such as gait, range of motion, and signs of FAIS or mechanical symptoms (snapping, catching, locking) were recorded. Radiographs using the anteroposterior, Dunn 45°, and false-profile views were obtained. Radiographic measurements included the LCEA, anterior center-edge angle, alpha angle, and Tönnis angle of acetabular inclination. The Tönnis classification was used to grade osteoarthritis. Cam-type morphology was defined as an alpha angle ≥55°. 9,23 All radiographs were evaluated by board-certified musculoskeletal radiologists and confirmed by board-certified orthopaedic surgeons specializing in hip preservation.
Surgical Technique
Patients were administered general anesthesia, were placed in the modified supine position, and had traction applied to the hip as needed. At least 3 portals were created: anterolateral, midanterior, and distal anterolateral accessory. A diagnostic arthroscopic examination to assess the labrum and intra-articular cartilage was performed. The Seldes classification was used to grade labral tears. 34 The acetabular labrum articular disruption (ALAD) and Outerbridge classifications were used to assess the chondrolabral junction and cartilage lesions, respectively. 13 Ligamentum teres tears were graded using a scale previously established by Botser et al 3 in which grade 0 is no tear, grade 1 is a low-grade partial tear (<50%), grade 2 is a high-grade partial tear (>50%), and grade 3 is a full-thickness tear.
When indicated, labral tears underwent repair, reconstruction, or selective debridement. Fluoroscopic guidance was used while performing acetabuloplasty and femoroplasty to correct pincer- and cam-type morphologies, respectively. At the end of every procedure, the capsule was repaired unless the senior surgeon determined that there was insufficient capsular tissue, excessive stiffness, or adhesive capsulitis.
Postoperative Rehabilitation Protocol
Patients were provided with individualized rehabilitation protocols: specifically, 2 weeks with a hip brace and crutches restricted to 20 lb (9.1 kg) of weightbearing after labral repair or debridement, 2 weeks with a hip brace and 6 weeks with crutches restricted to 20 lb of weightbearing after labral reconstruction, and 2 weeks with a hip brace and 8 weeks with crutches restricted to 20 lb of weightbearing after acetabular or femoral microfracture. Additionally, 3 months of physical therapy was indicated. Furthermore, 6 weeks of naproxen 500 mg to be taken twice daily was prescribed to patients to minimize the possibility of heterotopic ossification.
Surgical Outcomes
Patients completed the modified Harris Hip Score (mHHS), 1 Nonarthritic Hip Score (NAHS), 6 Hip Outcome Score–Sport-Specific Subscale (HOS-SSS), 24 and visual analog scale (VAS) for pain 5 during clinic visits. Those patients unable to complete questionnaires in the clinic were contacted using encrypted email or by telephone. The preoperative, minimum 2-year, and minimum 5-year outcome scores were analyzed. In addition, patient satisfaction at 2- and 5-year follow-up was determined by having patients answer a series of questions on whether their preoperative goals were met after surgery. 18,19,29 Moreover, the MCID at 5-year follow-up was calculated for the mHHS, NAHS, HOS-SSS, and VAS for pain using the method described by Norman et al. 27
Statistical Analysis
All statistical analyses were conducted with Excel with the Real Statistics add-in package (Microsoft). The F test and Shapiro-Wilk test were used to determine the variance equality and normality of quantitative data. A 2-tailed t test or its nonparametric t test was used to assess quantitative data. P < .05 was determined to establish statistical significance.
Logistic regression was performed using the Real Statistics add-in package in Excel. Conversion to THA was considered an endpoint. Hips were categorized into those that converted to THA versus survivors, and bivariate analysis was conducted for demographic, radiographic, intraoperative, and surgical variables. Variables with P < .05 on bivariate analysis were included in regression analysis. 14 Significant variables found on regression analysis were reported as odds ratios and 95% CIs. A receiver operating characteristic (ROC) curve and area under the ROC curve (AUC) were included to assess the validity of the regression. Previous AUC values reported by Copay et al 7 were used to determine the quality of the model: 0.50 indicated a random assignment, 0.70 was a fair model, 0.80 was a high-quality model, and 1.00 indicated a perfect assignment.
Results
Patient Demographics
Of 30 hips that met the inclusion criteria, 24 hips (24 patients; 80.0%) had a minimum 5-year follow-up and were included (Figure 1). There were 11 female (45.8%) and 13 male (54.2%) patients, with a mean age of 39.3 ± 12.7 years. The mean follow-up time was 83.9 ± 26.5 months. Patient characteristics are shown in Table 1. The indications for revision hip arthroscopic surgery were labral retearing (n = 22) and heterotopic ossification removal (n = 2). A cam deformity was also a concurrent indication for revision hip arthroscopic surgery in some patients.

Patient selection flowchart. BMI, body mass index.
Patient Demographics (n = 24) a

a Data are presented as mean ± SD, mean ± SD (range), or n (%). BMI, body mass index.
Radiographic Measurements
There were 21 patients (87.5%) who had a Tönnis grade of 0. The mean LCEA was 28.7° ± 5.9°. All other radiographic measurements are found in Table 2.
Radiographic Measurements a
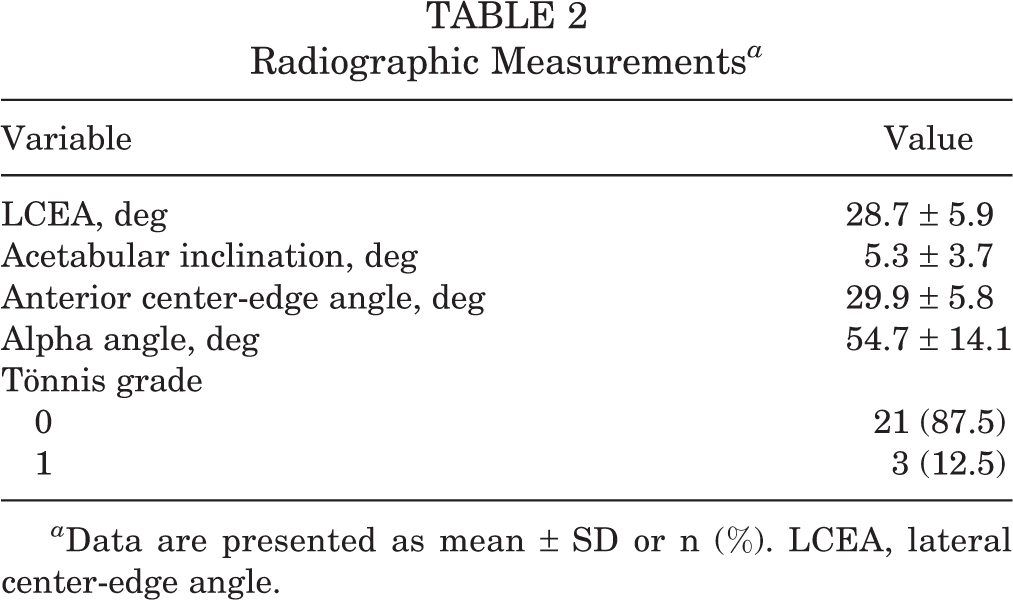
a Data are presented as mean ± SD or n (%). LCEA, lateral center-edge angle.
Intraoperative Findings and Surgical Procedures
Most patients had a Seldes type 2 labral tear (n = 15 [62.5%]). The most common labral treatment was selective debridement (n = 14 [58.3%]). Further, 14 patients (58.3%) underwent femoroplasty. Intraoperative findings and surgical procedures are recorded in Tables 3 and 4, respectively.
Intraoperative Findings a

a ALAD, acetabular labrum articular disruption.
Surgical Procedures

Survivorship and Complications
The survivorship rate at final follow-up was 75.0%. Patients who required THA (n = 6) were converted at a mean time of 19.1 ± 16.5 months after the revision procedure. A Kaplan-Meier survivorship curve for conversion to THA is shown in Figure 2. None of the patients underwent tertiary hip arthroscopic surgery. One patient who underwent THA had a superficial non–Staphylococcus aureus infection in one portal, which resolved with oral antibiotics .
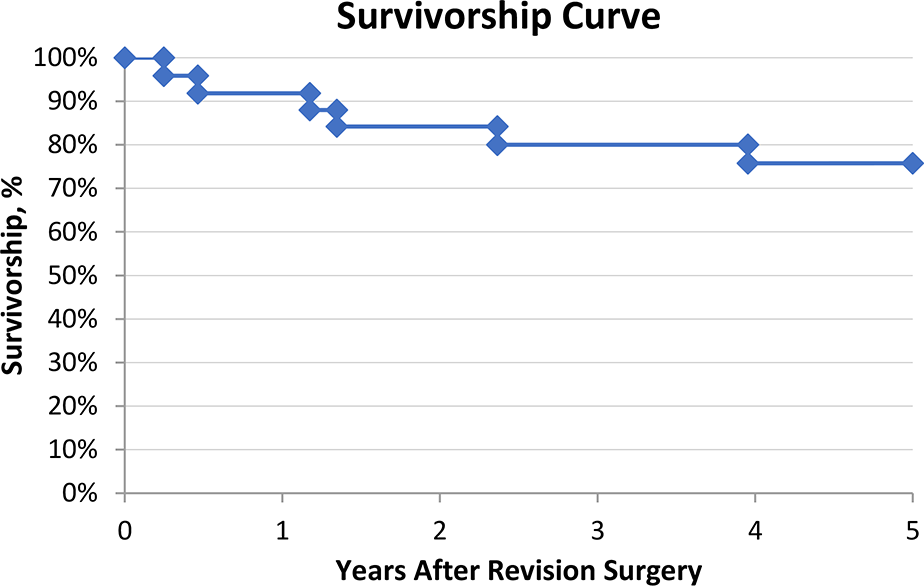
Survivorship curve for patients who converted to total hip arthroplasty (n = 6).
Surgical Outcomes
The patients who did not require conversion to THA had a significant preoperative to postoperative improvement in all PROs (P < .01 for all) (Table 5). Additionally, these patients reported high satisfaction (defined as ≥7/10) 25 at the minimum 2- and 5-year time points (7.2 ± 2.7 and 7.1 ± 2.4, respectively). Also, 16 patients (94.1%) achieved the MCID for the NAHS, and 13 patients (92.9%) achieved the MCID for the HOS-SSS (Table 6).
PROs for Patients Who Did Not Convert to THA (n = 18) a

a Data are presented as mean ± SD unless otherwise indicated. Boldface P values indicate a statistically significant difference between preoperative and latest follow-up (P < .05). HOS-SSS, Hip Outcome Score–Sport-Specific Subscale; mHHS, modified Harris Hip Score; NAHS, Nonarthritic Hip Score; PRO, patient-reported outcome; THA, total hip arthroplasty; VAS, visual analog scale.
MCID Achievement for Patients Who Did Not Convert to THA a

a HOS-SSS, Hip Outcome Score–Sport-Specific Subscale; MCID, minimal clinically important difference; mHHS, modified Harris Hip Score; NAHS, Nonarthritic Hip Score; THA, total hip arthroplasty; VAS, visual analog scale.
Results of Regression Analysis
On bivariate analysis, acetabuloplasty (P = .012), higher grade ligamentum teres tears (P = .020), and older age (P < .001) were identified as significant variables for conversion to THA. Each variable was individually run in the regression, and older age was found to be significant in the regression for conversion to THA (odds ratio, 1.297 [95% CI, 1.045-1.609]; P = .018). The AUC of the ROC curve was 0.972 (Figure 3).
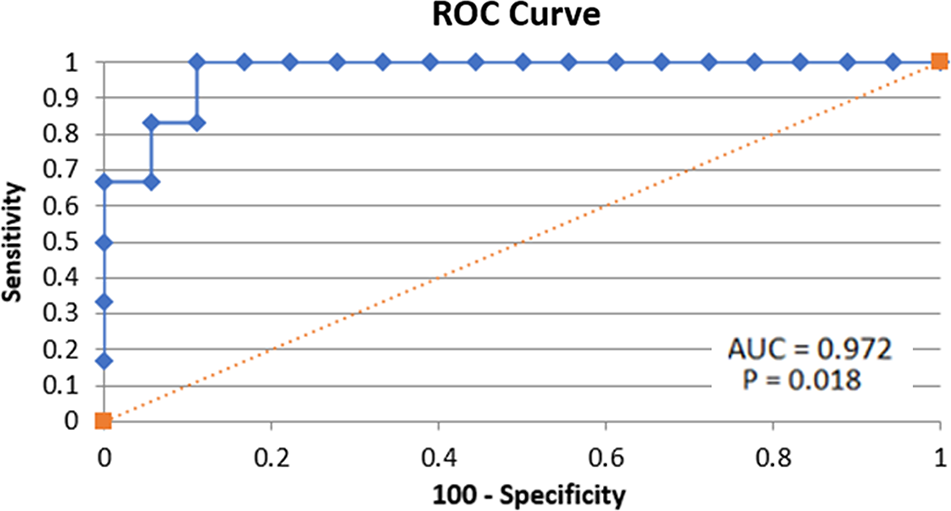
Receiver operating characteristic (ROC) curve and area under the curve (AUC).
Discussion
The main finding of the present investigation was that the rate of survivorship, defined as no conversion to THA, after revision hip arthroscopic surgery in obese patients was 75.0% at a minimum 5-year follow-up. Within the patients who did not convert to THA, a significant improvement was shown in all the PROs collected in addition to achieving high rates of the MCID. Increased age was identified as a significant predictor on regression analysis, with every additional year of age involving a 29.7% greater risk of conversion to THA at the time of revision.
Bech et al 2 reported that although obese patients show comparable improvements after hip arthroscopic surgery for FAIS compared to nonobese patients, revision and conversion to THA rates were 4.7 and 2.2 times higher, respectively. Similarly, Kuroda et al 16 reported that complication and conversion to THA rates were 3.2 and 2.4 times higher, respectively, in the obese population compared to the nonobese population. Using machine learning analysis of preoperative risk factors, Haeberle et al 12 determined that increased BMI was among the important predictive factors for revision hip arthroscopic surgery and conversion to THA, with model accuracies of 76% and 81%, respectively. Using bivariate and multivariate analyses, Domb et al 10 determined that BMI and revision hip arthroscopic surgery were predictive of conversion to THA at a minimum 5-year follow-up. The conversion to THA rate reported was 15.4%, which included primary and revision procedures. The conversion rate was considerably higher in the present study (25.0%).
Within the primary setting, Parvaresh et al 30 reported significant improvements in at least one PRO in patients classified as morbidly obese (BMI >35) and obese (BMI = 30-34.9) after arthroscopic FAIS treatment. However, obese patients were 14.1 and 7.8 times less likely, respectively, to achieve the patient acceptable symptomatic state and substantial clinical benefit compared to nonobese patients. Perets et al 31 reported that obese patients undergoing primary hip arthroscopic surgery had a conversion to THA rate as high as 29.7%, which is comparable with the rate reported in the present study. However, 51.4% of patients in the primary group presented by Perets et al 31 had ALAD grade 3 or 4 versus only 12.5% of patients in the current study with ALAD grade 3 or 4. This may have confounded the results, and further studies are necessary to determine, irrespective of cartilage damage, if BMI is correlated with an increased risk of secondary surgery in the revision setting.
Previous systematic reviews on outcomes after revision hip arthroscopic surgery have reported that although revision hip arthroscopic surgery improved PROs, the magnitude of improvement was smaller when compared with the primary hip arthroscopic surgery group. 8,32,33,35 Currently, data on the obese population after revision hip arthroscopic surgery are scarce. Compared to nonobese patients in the revision setting, obese patients fared worse. In a recent systematic review on outcomes after revision hip arthroscopic surgery, O’Connor et al 28 reported that the conversion to THA rate ranged from 0% to 14.3%. The conversion rate in the present study was over 1.5 times higher than the highest rate reported in the abovementioned systematic review, hinting that obese patients may have a greater risk of converting to THA than their nonobese counterparts. According to the results of the present study, a significant improvement can be expected in this context. However, it is important to note that all patients had identifiable sources of pain that did not resolve with nonoperative treatment. Patients without identifiable sources of pain should be cautioned against surgery.
Strengths and Limitations
This study has several strengths. It is the only study assessing and reporting survivorship, PROs, and clinical benefit at a minimum 5-year follow-up in obese patients who underwent revision hip arthroscopic surgery. We reported the MCID to contextualize patient improvement and determine if the patients who did not require conversion to THA experienced noticeable clinical benefits and satisfactory postoperative outcomes. Maldonado et al 21 reported that after revision hip arthroscopic surgery, 66.1%, 68.4%, 66.9%, and 80.0% of patients achieved the MCID for the mHHS, HOS-SSS, NAHS, and VAS for pain, respectively. Overall, the rates in the current study were higher for the mHHS, NAHS, and HOS-SSS (70.6%, 94.1%, and 86.7%, respectively) but not for the VAS for pain (64.7%). These differences may be because of the smaller sample size included in the present study, and larger sample sizes may be needed to validate whether obese patients can achieve high rates of clinical benefit after revision hip arthroscopic surgery.
This study has limitations that must be acknowledged. First, the retrospective nature of the study introduces bias. Second, all surgical procedures were conducted by a single surgeon at a high-volume surgery center, so results may not be generalizable; moreover, it is important to highlight that the reproducibility of the results may be affected, as data were obtained from a single institution. Third, the sample size was modest, and future studies with a larger sample size are needed to validate the findings. Fourth, patients who required conversion to THA were considered an endpoint; therefore, these patients were excluded from PRO analysis. Fifth, data on primary surgery were limited, and not all surgical procedures may have been performed by the senior author.
Conclusion
In this single-surgeon case series study, 25.0% of obese patients who underwent revision hip arthroscopic surgery required conversion to THA. The patients who did not require conversion to THA had a significant improvement in all PROs, with 70.6%, 94.1%, 92.9%, and 64.7% achieving the MCID for the mHHS, NAHS, HOS-SSS, and VAS, respectively, at a minimum 5-year follow-up. Increasing age was identified as a significant predictor of conversion to THA in the regression, and every additional year of age at the time of revision was identified as a 29.7% greater risk of conversion to THA.
Footnotes
Final revision submitted October 13, 2022; accepted November 8, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: D.R.M. has received research support from Arthrex; education payments from Arthrex, Micromed, and Smith & Nephew; speaking fees from Arthrex; and hospitality payments from Stryker. A.E.J. has received grant support and education payments from Arthrex. B.G.D. has received research support from Arthrex, ATI, the Kauffman Foundation, Pacira Pharmaceuticals, and Stryker; has received consulting fees from Adventist Hinsdale Hospital, Arthrex, MAKO Surgical, Medacta, Pacira Pharmaceuticals, and Stryker; has received educational support from Arthrex and Breg; has received speaking fees from Arthrex, Pacira Pharmaceuticals, and Stryker; has received honoraria from Medacta; has received royalties from Amplitude, Arthrex, DJO, MAKO Surgical, Medacta, Orthomerica, and Stryker; and has had ownership interests in the American Hip Institute, SCD#3, Hinsdale Orthopaedics, the Munster Specialty Surgery Center, and North Shore Surgical Suites. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Advocate Health Care (No. 5276).