
Abstract
Background:
Both remnant preservation (RP) and bone marrow stimulation (BMS) enhance the healing potential of the repaired rotator cuff by improving the biological milieu of the tendon-bone interface.
Purpose:
To evaluate the clinical and imaging outcomes of arthroscopic rotator cuff repair using a combined RP-BMS technique in patients with acute rotator cuff tears.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Between January 2016 and June 2019, a total of 56 patients were diagnosed with acute rotator cuff tears; 29 patients underwent conventional repair (group 1), and 27 patients underwent RP-BMS (group 2). At a minimum follow-up period of 2 years, the authors compared clinical outcomes with the University of California–Los Angeles; Constant; American Shoulder and Elbow Surgeons; and pain visual analog scale scores as well as shoulder range of motion. Tendon integrity and retear were assessed on magnetic resonance imaging according to the Sugaya classification (intact, grades 1-3; retear, grades 4-5). Between-group comparisons were conducted using the Student t test or Mann-Whitney U test for continuous variables and the Pearson chi-square test or Fisher exact test for categorical variables.
Results:
In both groups, patients had significant preoperative to postoperative improvement on all clinical outcome measures (P = .001 for all). Shoulder abduction in group 2 was significantly greater compared with group 1 at the postoperative 3-month (107.37° ± 8.32° vs 95.44° ± 8.78°; P = .001), 6-month (155.25° ± 10.02° vs 144.72° ± 9.28°; P = .001), and final (165.15° ± 9.17° vs 158.31° ± 8.01°; P = .021) follow-ups. At the final follow-up, significantly more patients in group 2 had intact tendons (Sugaya grades 1-3) compared with group 1 (P = .015), and the tendon retear rate was lower in group 2 (1/27; 3.70%) than in group 1 (7/29; 24.14%) (P = .033).
Conclusion:
Both surgical techniques led to satisfactory clinical outcomes, but shoulder abduction was greater after the RP-BMS technique compared with conventional repair. RP-BMS may be an alternative surgical technique to improve tendon integrity and retear rates after the repair of acute rotator cuff tears.
Keywords
Rotator cuff tears are one of the most common causes of shoulder pain and dysfunction, and arthroscopic repair is an effective treatment for rotator cuff tears. 9,19 There are many surgical methods for rotator cuff repair, including single-row or double-row anchor repair technology, layer-by-layer suture bridge technology, transosseous tunnel technology, and patch augmentation technology. The objective of these methods is to reattach the torn tendon to its footprint and fix it to create favorable conditions for tendon-bone healing at the native enthesis of the rotator cuff.
The normal native enthesis structure contributes to maintaining the balance of stress and greatly reducing the risk of normal rotator cuff tissue tearing. 28,38 However, in many traditional rotator cuff repair techniques, most clinicians choose to remove the remnant tissue and cortical bone of the torn rotator cuff footprint to achieve a fresh bone bed in the footprint and ensure that the torn tendon is accurately reattached to its footprint under direct visualization. 7,14 This type of surgical procedure completely eliminates the native enthesis, which provides stress relief to the rotator cuff tendon. A study found that disordered scar tissue eventually forms at the tendon-bone interface after adult rotator cuff repair. 11 Disordered scar tissue does not have a highly migrating layered gradient structure, and its mechanical conductivity is significantly weakened. In complex shoulder joint movements, stress will be too concentrated at the tear, resulting in rotator cuff retear. 30 Some studies have reported that the retear rate after rotator cuff repair is as high as 21% to 94%. 9,37
After acute rotator cuff tears, there is often a large amount of rotator cuff remnant tissue attached to the footprint area of the humeral tubercle, and native enthesis is usually preserved well. 3,33 A study found that these remnant tissues were rich in tendon-derived stem cells and new blood vessels, which may facilitate healing after rotator cuff repair. 16 Furthermore, several studies have demonstrated that there are a large number of mechanoreceptors at the rotator cuff tendon-bone junction, and retaining the remnant tissue of the rotator cuff may promote the recovery of proprioception after surgery. 5,8,31 Therefore, we have reason to believe that a modified surgical technique that utilizes the native enthesis of the rotator cuff by preserving the rotator cuff remnant tissue may stimulate the inherent healing potential of the rotator cuff tendon-bone interface. 3,28
Biological techniques to promote rotator cuff healing have also attracted extensive attention in recent years. Mesenchymal stem cells (MSCs), slow-release growth factors, and biological patches are increasingly used to improve the biological healing process of rotator cuff repair. 21,24,38 The bone marrow stimulation (BMS) technique is a safe, economic, and simple biological technique. It drills down on the surface of the footprint area to form multiple vents that can release endogenous MSCs, various growth factors, and platelets to enhance the biological milieu at the tendon-bone interface. 23 Some studies have demonstrated that BMS technology improves the healing effect and reduces the retear rate after rotator cuff repair. 1,2,18,32,37 Theoretically, both the preservation of the remnant tissue and the BMS technique can increase the healing potential of the repaired rotator cuff by improving the biological milieu of the tendon-bone interface. However, to our knowledge, there are currently no clinical studies combining these 2 techniques for the repair of acute rotator cuff tears.
In the present study, we introduce a surgical technique that combines BMS with rotator cuff remnant preservation (RP) for the repair of acute rotator cuff tears. The technique is named the RP-BMS technique. The purpose of this study was to compare clinical outcomes and repair integrity between the RP-BMS technique and the conventional repair technique for acute rotator cuff tears. We hypothesized that the RP-BMS technique would improve the clinical outcomes and tendon integrity of repair in acute rotator cuff tears compared with conventional repair.
Methods
Patient Enrollment
The protocol for this study was approved by our institution, and all patients provided written informed consent. We retrospectively reviewed the medical records of 420 consecutive patients with rotator cuff tears between January 2016 and June 2019; the acute rotator cuff tear was repaired in 70 of these patients. Notably, the duration of the acute rotator cuff tear was within 8 weeks of injury, and there was no obvious fat infiltration and muscle atrophy on preoperative magnetic resonance imaging (MRI) in the acute rotator cuff tear. 26 In addition, patients were also confirmed to have acute rotator cuff tears by intraoperative arthroscopic inspection.
The study inclusion criteria were (1) acute and isolated supraspinatus tears (within 8 weeks of injury 26 ); (2) <5 cm rotator cuff tear (according to the Cofield classification 4 ); (3) use of RP-BMS or the conventional repair technique for acute rotator cuff tear repair; (4) complete preoperative and final follow-up MRI scans and shoulder functional assessment; and (5) a minimum follow-up period of 24 months. The study exclusion criteria were (1) a history of surgery on the affected shoulder; (2) massive rotator cuff tears according to the Cofield classification 4 ); (3) Goutallier fatty infiltration grade 13 >2; (4) chronic rotator cuff tear (injured for >8 weeks 26 ); (5) patients older than 70 years; and (6) patients with glenohumeral dislocation. After application of the inclusion and exclusion criteria, the remaining patients were classified according to rotator cuff repair technique: conventional repair (group 1) and RP-BMS (group 2).
Surgical Techniques
All surgeries were performed by a senior arthroscopic surgeon (F.B.) with 10 years of surgical experience. Through inspection under arthroscopy, all 56 patients were confirmed to have acute rotator cuff tears. All patients were treated with general anesthesia combined with brachial plexus anesthesia and were placed in the beach-chair position. Schematic diagrams of the surgical techniques are shown in Figure 1, and details of both procedures are shown in the Video Supplement to this article.

Schematic diagrams of the surgical techniques. (A and B) Conventional repair technique. The rotator cuff remnant was removed and the footprint area was freshened (black arrow). (C and D) Remnant preservation combined with bone marrow stimulation (RP-BMS) technique. The rotator cuff remnant was preserved (black arrow), and BMS was performed in the footprint (black arrow).
RP-BMS Technique
A standard posterior portal was used to explore the glenohumeral joint, long head of the biceps tendon, humeral head cartilage, and rotator cuff tear on the joint side; then planer and radiofrequency electrocautery were performed to properly release adhesions superficial and deep to the rotator cuff. The synovial tissue of the acromion was cleaned in the subacromial space, and acromioplasty was performed in patients with acromion impingement. Tenodesis of the long head of the biceps and labrum repair were performed if necessary. The tendon tear was then exposed (Figure 2A), the torn rotator cuff tendon was grasped with a grasper to pull the tendon to its footprint, and the tension of the torn tendon and the tear size were assessed (Figure 2B). The frayed torn end was appropriately freshened. Unlike conventional bone bed freshening in the footprint area, this technique was selected to preserve the native enthesis of the rotator cuff remnant in the footprint area (Figure 2C).

Remnant preservation combined with bone marrow stimulation (RP-BMS) technique. (A) Supraspinatus tendon tear (black arrow). (B) The tension of the torn tendon and the tear size were assessed (black arrow). (C) Native enthesis of the torn tendon remnant. (D) The bone marrow stimulation technique (black arrow). (E) The inner-row anchors were inserted (black arrow). (F) The sutures were passed through the full thickness of the torn supraspinatus tendon with lasso loop stitches (black arrow) and a supraspinatus tendon tear (black triangle). (G) A mattress stitch was tied medially (black arrow). (H) The free suture limbs were anchored laterally (black arrow). (I) The torn rotator cuff was anatomically reattached (black arrow). HF, footprint area of the humeral tubercle; RE, native enthesis of the rotator cuff remnant.
Next, we performed BMS. A 3 mm–diameter bone punch (Smith & Nephew) was used to create 4 or 5 small holes with a depth of 5 mm perpendicular to the surface of the footprint area of the humeral tubercle so that part of the blood and bone marrow leaks out of the holes (Figure 2D). The holes were made at a distance of approximately 3 to 5 mm. It was necessary to avoid the area where the subsequent inner-row anchors were placed. After BMS, we began repairing the torn rotator cuff with the double-row anchor suture technique: according to the size and shape of the tendon tear, two or three 5.5 mm–diameter inner-row anchors (China Ruijian Medical) were inserted at the postero- and anteromedial edges of the footprint near the cartilage-bone interface (Figure 2E). The sutures were passed through the full thickness of the torn supraspinatus tendon from the articular side to the bursa side at the area of the tendon-ventral junction with lasso loop stitches (Smith & Nephew) (Figure 2F). The tendon was anatomically reattached, and the contact area between the torn tendon and its native enthesis was maximized by adjusting the suture tension. Afterward, a mattress stitch was tied medially (Figure 2G). Next, the free suture limbs were anchored 10 mm lateral to the greater tuberosity with 1 or 2 lateral knotless anchors (China Ruijian Medical) according to tear size (Figure 2H). The rotator cuff was reattached, and the tension was appropriate (Figure 2I).
Conventional Repair Technique
Systematic glenohumeral joint and subacromial exploration was performed. Adhesions superficial and deep to the rotator cuff were released. A tenodesis of the long head of the biceps, labrum repair, and acromioplasty were performed if necessary. The tendon tear was then exposed (Figure 3A), and an attempt was then made to pull the tendon to its footprint with a grasper (Figure 3B). Afterward, any remnant tissue of the torn tendon was carefully debrided from its native enthesis, and the superficial cortical bone of the footprint was removed with a shaver and radiofrequency electrocautery (Figure 3, C and D). Cancellous bone and oozing blood could be observed on the surface of the freshened bone bed (Figure 3E). Then, we repaired the torn tendon using the same double-row anchor suture technique used in the RP-BMS technique (Figure 3, F-I). Notably, we could see that the torn tendon would be reattached to the fresh bone bed of the humeral tubercle footprint, and the native enthesis of the torn tendon remnant was no longer visible (Figure 3H).

Conventional repair technique. (A) Supraspinatus tendon tear (black arrow). (B) The tension of the torn tendon and the tear size were assessed (black arrow). (C and D) Remnant tissue of the torn tendon was debrided, and cortical bone of the footprint was removed (black arrow). (E) The freshened bone bed (black arrow). (F) The inner-row anchors were inserted (black arrow ). (G) The sutures were passed through the full thickness of the torn tendon with lasso loop stitches (black arrow). (H) The torn tendon was reattached to the fresh bone bed of the humeral tubercle footprint (black arrow). (I) The torn rotator cuff was anatomically reattached (black arrow). HF, footprint area of the humeral tubercle.
Postoperative Rehabilitation
Postoperative rehabilitation was the same in both study groups. The patients were instructed to perform wrist and hand function exercises immediately after surgery. All patients wore a shoulder abduction brace after surgery, and the shoulder was immobilized for 6 weeks. Passive shoulder exercise was allowed within 6 weeks postoperatively. Six weeks postoperatively, the shoulder abduction brace was removed, and patients performed active-assisted shoulder exercises. The range of motion of the shoulder gradually increased. Strengthening exercises were allowed 3 months postoperatively. A full return-to-sports activities was allowed at 6 months postoperatively.
Clinical and MRI Assessment
Shoulder function was evaluated with the Constant score, 36 the American Shoulder and Elbow Surgeons (ASES) score, 25 and the University of California–Los Angeles (UCLA) score 34 ; pain was evaluated on visual analog scale (VAS) preoperatively and at the final follow-up. Forward flexion, external rotation in abduction, and abduction were measured preoperatively and on postoperative 2-month, 3-month, 6-month, and final follow-ups.
Preoperative and follow-up MRI scans were performed on a 3.0-T scanner (MAGNETOM Skyra; Siemens). All MRI scans were evaluated by a musculoskeletal radiologist with 10 years of experience, and he was blinded to the groups. Tendon integrity was evaluated with the classification of Sugaya et al 29 (grades 1-3 indicated intact tendons, grades 4-5 indicated retears). Muscle fat infiltration was evaluated with the MRI grading criteria of Fuchs et al 10 (grade 0 [no fat infiltration] to 4 [more fat than muscle]). Muscle hypotrophy was evaluated with the grading criteria of Thomazeau et al 35 (grade 1 [slight atrophy] to 3 [severe atrophy]).
Statistical Analysis
The power of this retrospective study was calculated based on the abduction between the study groups. Using a 2-sided alpha error of .05, a power of 0.82 was calculated. Paired t tests or Wilcoxon signed-rank tests were used to compare the functional scores and shoulder range of motion preoperatively and at the final follow-up according to the normality of the data. The Student t test or Mann-Whitney U test was used to compare continuous variables between groups 1 and 2, and the Pearson chi-square test or Fisher exact test was used to compare categorical variables. Statistical significance was set as P < .05. The data were analyzed using SPSS (Version 23.0; IBM Corp).
Results
Patient Data
After application of the inclusion and exclusion criteria, 56 patients with acute rotator cuff tears were enrolled. There were 29 patients in group 1 (conventional repair) and 27 patients in group 2 (RP-BMS) (Figure 4). Table 1 shows the general characteristics of the study groups. There were no significant differences in any of the patient and surgery characteristics between the 2 groups.

Flow diagram of patient inclusion and exclusion. RP-BMS, remnant preservation combined with bone marrow stimulation.
Characteristics of the Study Patients (N = 56). a

a Data are presented as mean ± SD unless otherwise indicated. BMI, body mass index.
Clinical Outcomes
In both groups, patients had significant improvement on all clinical outcome measures at the final follow-up compared with preoperatively (P = .001 for all) (Table 2). Shoulder abduction in group 2 was significantly greater compared with group 1 at the postoperative 3-month (107.37° ± 8.32° vs 95.44° ± 8.78°; P = .001), 6-month (155.25° ± 10.02° vs 144.72° ± 9.28°; P = .001), and final (165.15° ± 9.17° vs 158.31° ± 8.01°; P = .021) follow-ups (Figure 5). None of the other scores were significantly different between the 2 groups (Table 2). Complications such as shoulder infection, shoulder stiffness, and shoulder dislocation were not observed in either group.
Functional Score Outcomes a

a Data are presented as mean ± SD. Boldface P values indicate a statistically significant difference between groups compared (P < .05). ASES, American Shoulder and Elbow Surgeons; UCLA, University of California–Los Angeles; VAS, visual analog scale.
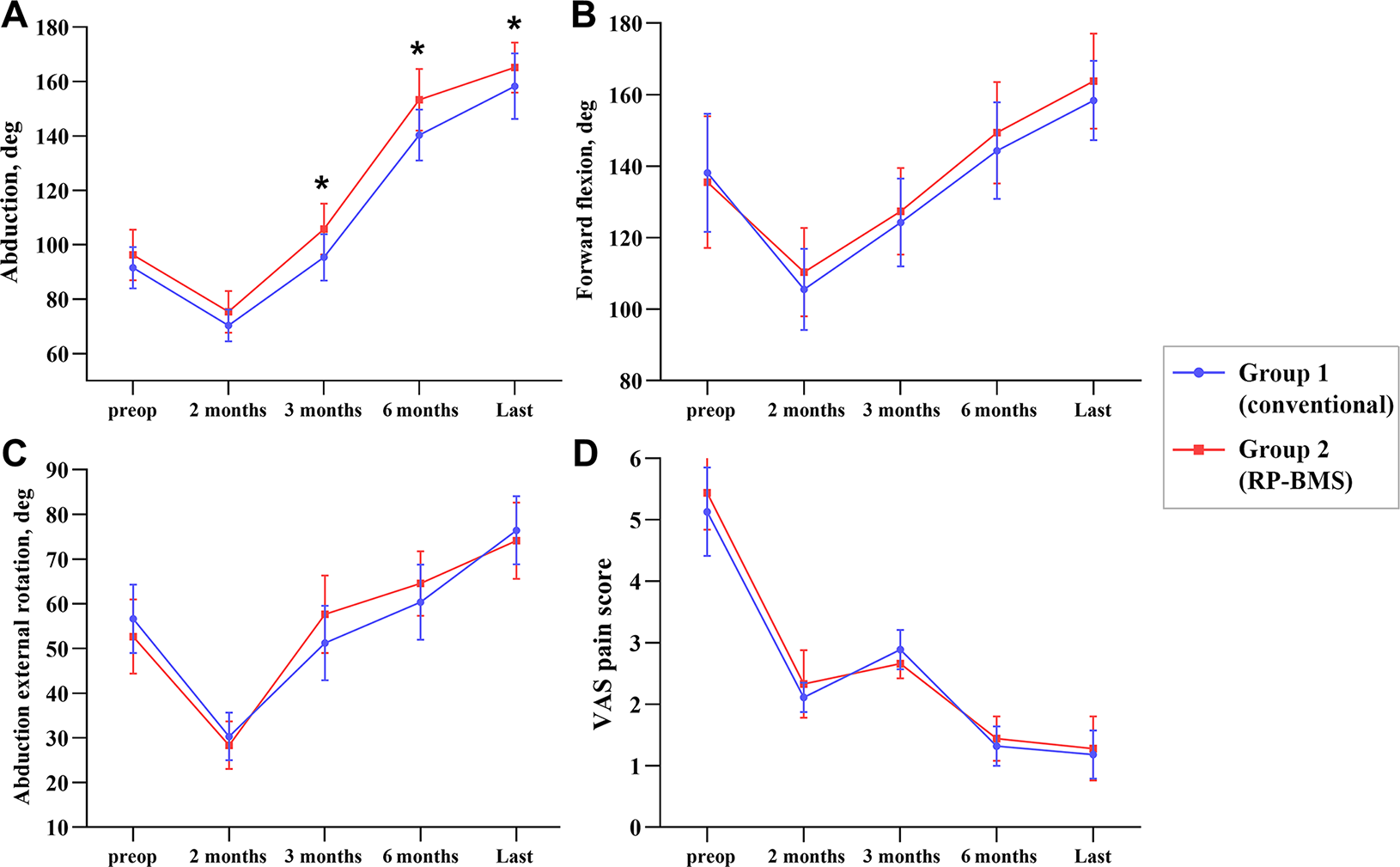
Comparison of preoperative and postoperative mean shoulder range of motion and pain values in groups 1 and 2: (A) abduction; (B) forward flexion; (C) external rotation in abduction; and (D) visual analog scale (VAS) pain score. Error bars represent standard deviations. *Statistically significant difference between groups (P < .05). RP-BMS, remnant preservation combined with bone marrow stimulation.
MRI Outcomes
MRI outcomes at the final follow-up are shown in Table 3 and Figure 6. In both groups, there were more patients with intact tendons (Sugaya grades 1-3) at the final follow-up compared with preoperatively (P = .001), with significantly more patients in group 2 having intact tendons compared with group 1 (P = .015). In addition, the tendon retear rate was significantly lower in group 2 compared with group 1 (3.70% vs 24.14%, respectively; P = .033).
MRI Outcomes a
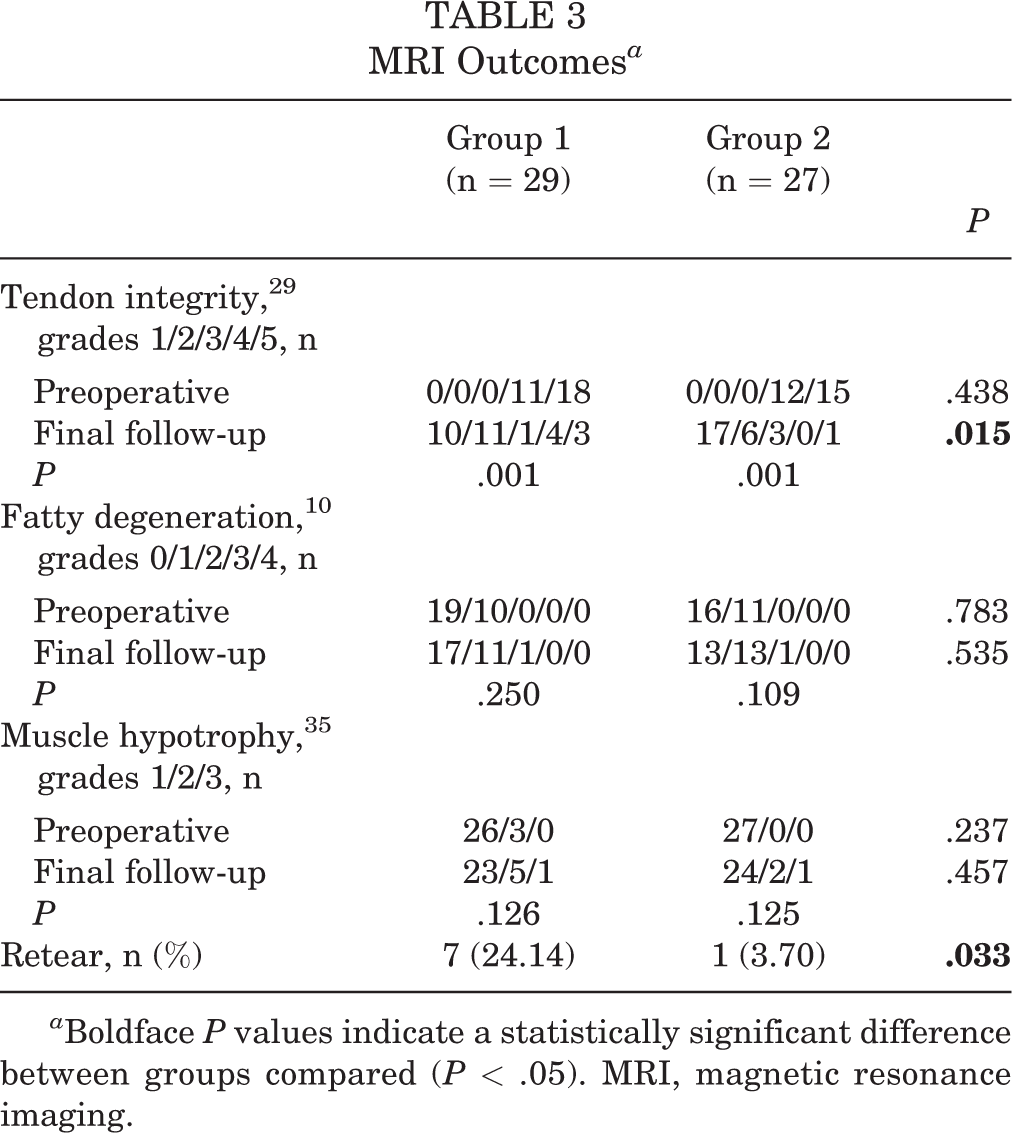
a Boldface P values indicate a statistically significant difference between groups compared (P < .05). MRI, magnetic resonance imaging.

Magnetic resonance imaging (MRI) assessment. (A) Preoperative coronal T2-weighted (T2W) MRI showing a supraspinatus tear (Sugaya grade 5, yellow arrow) in group 2. (B) Coronal T2W MRI at the final follow-up showing intact tendon structure (Sugaya grade 1) with a visible remnant tissue that was preserved in the remnant preservation combined with bone marrow stimulation repair technique (yellow arrow). (C) Oblique sagittal T2W MRI at the final follow-up showing muscle with atrophy (grade 1) but without obvious fatty infiltration (grade 0) in group 2 (yellow arrow). (D) Preoperative coronal T2W MRI showing a supraspinatus tear (Sugaya grade 5) in group 1. (E) Coronal T2W MRI at the final follow-up showing intact tendon structure (Sugaya grade 2) without a visible remnant tissue that was moved in the conventional repair technique (yellow arrow). (F) Oblique sagittal T2W MRI at the final follow-up showing partial muscle atrophy (grade 2) but no fatty infiltration (grade 0) in group 1 (yellow arrow).
Discussion
The main findings of the present study were that (1) both surgical techniques led to satisfactory clinical outcomes in patients with acute rotator cuff tears, but greater shoulder abduction was seen after RP-BMS compared with conventional repair at the 3-month, 6-month, and final follow-ups (P < .05 for all); and (2) the tendon repair integrity and tendon retear rate were better in patients who underwent the RP-BMS technique compared with the conventional repair technique (P = .015 and .033, respectively).
The native enthesis of the rotator cuff is a gradual transitional layered structure at the tendon-bone junction. 12,38 In complex shoulder movement, this special structure contributes to the stable transmission of stress from the rotator cuff tendon to the humerus, ensuring the stress balance of the shoulder. 17 However, there is currently no technology that fully regenerates the native enthesis. For chronic rotator cuff tear cases, most of the remnant tissue of the torn rotator cuff is absorbed so that the native enthesis disappears, and the footprint area is covered by fibrous tissue and inflammatory synovium. 17,33,38 In this case, the degenerated remnant tissue in the footprint area was completely removed, and decorticalization was performed to improve the blood supply of the tendon-bone interface. In contrast, several studies found that the native enthesis was well preserved in 75% of acute rotator cuff tear cases. 3,26,33 Therefore, we believe that the RP-BMS technique may be more appropriate for the repair of acute rotator cuff tears than the conventional repair technique. This technique may improve tendon integrity of repair by preserving the remnant tissue of the torn tendon in acute rotator cuff tear.
One of the main goals of rotator cuff repair surgery is to relieve pain and restore shoulder function. A recent study from Kim et al 19 used en masse suture bridge techniques for full-thickness supraspinatus tears. At the final follow-up, the VAS, Constant, ASES, and UCLA scores were 1.1 ± 0.9, 84.3 ± 16.4, 88.3 ± 17.4, and 31.1 ± 6.0, respectively. Heuberer et al 15 used the knotless cinch-bridge technique for supraspinatus tears. At the final follow-up, the VAS, Constant, and ASES scores were 1.0 ± 0.3, 78.8 ± 11.2, and 88.4 ± 11.2, respectively. These results were consistent with our study. Both surgical techniques led to satisfactory clinical outcomes in patients with acute rotator cuff tears. However, the RP-BMS technique improved abduction of the patients compared with the conventional repair technique. An animal study by Su et al 28 found that retaining the rotator cuff remnant during repair surgery helped to improve the degree of scarring at the tendon-bone interface during rotator cuff healing. A biomechanical study found that increasing the footprint area of the greater tubercle in rotator cuff repairs improved tendon tensile loads and balanced stress distribution. 27 Because it retains the rotator cuff remnant, we thought that the RP-BMS technique may increase the footprint area coverage and improve scar healing of the tendon-bone interface. Furthermore, there were a large number of mechanoreceptors at the rotator cuff remnant, and mechanoreceptors contribute to maintaining proprioception in the rotator cuff. 5,8,31 The presence of proprioception will help improve muscle reflex activity and the kinematics of the muscle-tendon unit. These factors may optimize the mechanical performance of the repaired supraspinatus, resulting in better abduction function in the patient compared with the conventional repair technique.
The tendon retear rate after surgical repair has been a topic of interest in research. Kim et al 20 used double-layer repair for the treatment of delaminated rotator cuff tears. The average follow-up period was 25.9 ± 1.2 months, and 6 (18%) of 34 patients showed retears on MRI. Heuberer et al 15 used the knotless cinch-bridge technique for supraspinatus tears. The average follow-up period was 29.1 ± 9.3 months, and only 1 (3%) of 33 patients showed retears. A study from Levy et al 22 demonstrated that the remnant tissue of the torn rotator cuff had higher vascularity than the normal rotator cuff. An anatomic study found that the posterior humeral circumflex artery provided blood to the rotator cuff flowing from the greater tubercle footprint toward the proximal rotator cuff. 6 Furthermore, there are a large number of vasoactive and chemotactic factors, such as vascular endothelial growth factor and transforming growth factor–beta, in the remnant tissue of acute rotator cuff tears. 21 Therefore, retention of the remnant tissue may improve the healing environment at the tendon-bone interface.
The BMS technique, as a biological approach, provides endogenous MSCs, platelets, and growth factors for the tendon-bone interface. 23 Although traditional bone bed freshening techniques can release endogenous MSCs and cytokines, the disadvantage of the technique was that the uncovered footprint would not keep the bone marrow droplet, which is rich in MSCs, around the repaired tendon-bone junction and the droplet could vanish into the subacromial space in an instant. In contrast, the remnant tissue can cover the bone bed of BMS for the containment of the bone marrow droplet, forming a tight seal to sustain the action of MSCs for tendon-bone healing. 37 Therefore, we believe that the RP-BMS technique enhances the biological milieu of the tendon-bone interface compared with the conventional repair technique.
On the other hand, a biomechanical study from Sun et al 30 demonstrated that when the remnant tissue was preserved in rotator cuff repair, the repaired tendon had greater maximum load and stiffness 12 weeks after surgery compared with the control group. Furthermore, in some medium to large full-thickness supraspinatus tears, excessive removal of the rotator cuff remnant tissue may increase the distance between the footprint and the retractor tendon. This results in the need to apply more tension to the tendon for anatomic reattachment. In contrast, the retained remnant tissue in the footprint resembles an autologous biocompatible patch, forming a bridge between the proximal end of the tear and the footprint, which may result in lower tension while preserving the integrity of the torn tendon. 24 Therefore, we believe that the superior biological milieu and repair integrity of the RP-BMS technique may be considered to be the 2 essential factors for increasing the healing rate compared with the conventional repair technique.
Limitations
This study has some limitations. First, we used only a short follow-up time and a small sample size to assess retear rates after repair. Therefore, the research results may not be adequately representative. Second, our study included only acute tear cases, and we were uncertain whether the use of this technique would benefit patients with subacute or chronic cases whose tear remnant was well preserved. Third, the retrospective and nonrandomized design of this study should be regarded as an important limitation.
Conclusion
Both surgical techniques led to satisfactory clinical outcomes in patients with acute rotator cuff tears, but the RP-BMS technique improved the abduction of patients compared with the conventional repair technique. Furthermore, the RP-BMS technique may be an alternative surgical technique to improve tendon integrity of repair and retear rates in acute rotator cuff tears.
A Video Supplement for this article is available at https://journals.sagepub.com/doi/full/10.1177/23259671231152233#supplementary-materials
Footnotes
Acknowledgment
The authors thank Dr Ling Chen for academic advice.
Final revision submitted November 30, 2022; accepted December 8, 2022.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Third Affiliated Hospital of Zunyi Medical University (reference No. 2016-1-057).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.