
Abstract
Background:
Loss of knee extension (LOE) after anterior cruciate ligament reconstruction (ACLR) is associated with limited knee joint function and increased risk for knee osteoarthritis.
Hypothesis:
Preoperative LOE will affect postoperative LOE for up to 12 months after ACLR.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
Included were patients who underwent anatomic ACLR between June 2014 and December 2018. In all patients, the postoperative rehabilitation protocol was the same. A heel height difference (HHD) ≥2 cm between the affected and the contralateral leg was used as a measure of LOE. Based on preoperative HHD, patients were divided into LOE and no-LOE groups. The HHD was reevaluated at 1, 3, 4, 6, 9, and 12 months postoperatively. Proportional hazards analysis was used, with the dependent variable being whether a postoperative HHD <2 cm was achieved; the independent variables being the presence or absence of preoperative LOE; and the adjusted variables being age, sex, time to surgery, and presence of meniscal sutures.
Results:
A total of 389 patients (208 female, 181 male; median age, 21.0 years) were included in the study. There were 55 patients in the LOE group and 334 patients in the no-LOE group. The incidence of LOE at 12 months after ACLR was 13.8% in the no-LOE group and 38.2% in the LOE group (P < .001), with an absolute risk difference of 24.4%. The hazard ratio for achieving postoperative HHD <2 cm was 2.79 for the LOE group versus the no-LOE group (P < .001).
Conclusion:
Patients with preoperative LOE were nearly 3 times more likely than those without LOE to have LOE at 12 months after ACLR.
Anterior cruciate ligament reconstruction (ACLR) is performed in young, active patients and generally has good clinical outcomes. Nevertheless, knee pain, instability, quadriceps muscle weakness, and limited range of motion are sometimes reported after ACLR. 5,7,12,13 Therefore, some patients who undergo ACLR do not fully return to sports. In addition, patients with ACL injury are at high risk for knee osteoarthritis (OA), and even when ACLR is performed, it is difficult to predict progression to knee OA. 31 Despite improvements in surgical techniques, normal joint motion is not always regained. 23,30
Loss of knee extension (LOE) after ACLR is a common postsurgical problem. A longitudinal study by Shelbourne et al 24 revealed an association between LOE and knee OA. In their study, multivariate logistic regression revealed that the statistical factors predicting the presence of OA at 20 years after surgery were medial meniscal resection, LOE at the time of discharge from physical therapy (6.5 ± 2.7 months postoperatively), and older age at surgery. 24 LOE at 12 months postoperatively has been associated with weak extensor muscles, 22 and weak extensor muscles have also been associated with OA. 1 The incidence of postoperative LOE is reported to be 1.5% to 35% of patients with ACLR. 18 LOE after ACLR is associated with knee OA, 24 highlighting the importance of preventing LOE and improving knee extension. Anterior knee pain often occurs in patients with LOE. 17
Some studies have demonstrated that preoperative LOE affects the postoperative LOE after ACLR. These studies examined the associations between preoperative LOE and that at 4 weeks 14 or 6 months 15 after ACLR, which is generally when patients return to sporting activities. To observe the relationship between OA and LOE, the LOE should be observed for at least 2 to 5 years after ACLR, but no studies to date have examined this issue for more than 12 months. If preoperative LOE influences postoperative LOE over the long term, then the preoperative condition may be an important treatment target.
The purpose of the present study was to investigate the influence of the preoperative LOE on postoperative LOE for up to 12 months after ACLR. This was a preliminary study investigating the longitudinal influence of LOE on knee OA.
Methods
The protocol for this study received ethics committee approval, and informed consent to participate was provided by all participants. In this prospective cohort study, we enrolled 795 patients who underwent anatomic ACLR by 1 of 5 surgeons between June 2014 and December 2018. The inclusion criterion was initial ACLR using the knee flexor tendon without concomitant ligament injury, with or without meniscal tear. Exclusion criteria were complex ligament injuries, meniscal locking (mechanical block to extension: bucket-handle meniscus displaced and McMurray with intermittent mechanical complaints), revision surgery, bilateral injuries, previous lower extremity fractures or surgery, and patients with whom communication in Japanese was difficult. Basic information such as age, height, weight, waiting period before surgery, and participation in sports at the time of injury were extracted from the interview and medical records, and the presence or absence of meniscal sutures was extracted from the surgical records.
Main Outcome
The heel height difference (HHD) between the affected and contralateral leg was used as a measure of LOE. 22 HHD was used because of its high reproducibility and ability to evaluate small variations in knee extension deficits. In the HHD measurement, 1 cm of HHD is equal to 1.2° of knee extension limitation as measured by a goniometer; thus, HHD was considered suitable for evaluating small degrees of LOE. 22 We defined LOE as an HHD ≥2 cm according to a study by Shelbourne et al. 27
For the measurement, the patient lay prone with the patella on the edge of a table, and the HHD was measured using a ruler and level (Figure 1). 22 Independent physical therapists who were blinded to the patients’ previous HHD values measured HHD preoperatively and at 1, 3, 4, 6, 9, and 12 months postoperatively. The reliability of the measurements was verified with the intraclass correlation coefficient (ICC) before performing the present study. The intrarater reliability (ICC1,1; n = 6) was 0.90, and the interrater reliability (ICC1,2; n = 6) was 0.94. For knee joint angle evaluation by a standard goniometer, the interrater reliability of knee extension range of motion measurements is 0.59 to 0.80. 21

Measurement of heel height difference (HHD). The patient lay facing down with the patella on the edge of the table; HHD was measured using a ruler and level.
Rehabilitation Protocol
All cases were treated with the same postoperative rehabilitation protocol. Before ACLR, almost all cases underwent preoperative rehabilitation to regain normal range of motion and strength. The protocol was rigid from the day after surgery to day 14 (while in the hospital), and the time for outpatient visits depended on the patient. For all periods, we focused on the patient regaining normal knee extension and checked knee extension at the time of visits. Range of motion was assessed beginning the day after surgery. On day 3 after surgery, continuous passive motion (Gadelius Medical) was initiated (beginning at 0°-90° and gradually advancing to 0°-135°), and on day 8, active flexion was started, with the range of motion gradually increased over time.
Immediately after surgery, the patient’s knee was immobilized with an Alcare Knee Brace FX (Alcare), except for during rehabilitation exercises and continuous passive motion, and the patient was required to wear a rigid knee brace from postoperative day 8 until 3 months after surgery. Patients were allowed no weightbearing on the affected leg on days 1 and 2 after surgery, one-third partial weightbearing starting on day 3, one-half partial weightbearing starting on day 7, and full weightbearing starting on day 14. The schedule for the return to sports was as follows: ergometer exercise was started at 2 months postoperatively, and jogging was started at 3 to 4 months postoperatively after assessing the absence of LOE, swelling, and pain; a ratio of operated/non-operated knee extensor strength >60%; and the absence of major problems in one-leg squatting movements. If patients did not meet the criteria to begin jogging at 3 to 4 months, they were evaluated again at a later date. After the start of jogging, patients were permitted partial participation in practice from 6 months postoperatively and full participation after 9 months.
Statistical Analysis
Continuous data are reported as medians with interquartile ranges (IQRs), and categorical data are reported as counts and percentages. For comparison of the patient characteristics, the chi-square test and Mann-Whitney U test were used. A proportional hazards analysis was used to determine the relationship between preoperative and postoperative LOE, with the dependent variable being whether HHD <2 cm was achieved at 12 months postoperatively, and the independent variables being the presence or absence of preoperative LOE. The adjusted variables were age, sex, body mass index (BMI), time from injury to surgery, and the presence of meniscal sutures. These variables were chosen because older age, 8 male sex, 7 acute-phase surgery after ACL injury, 16,28,29 and limited knee extension after surgery 7,25 are reported to be factors affecting LOE after ACLR. In addition, the meniscus may be sutured to the posterior articular capsule, which may affect LOE. The absolute risk difference was calculated from the hazard ratio. All statistical analyses were performed using EZR (Saitama Medical Center, Jichi Medical University). 10 Results with P <.05 were considered statistically significant.
Results
Included were 795 patients who underwent ACLR, which was performed using the knee flexor tendon (semitendinosus tendon or semitendinosus and gracilis tendon) in 610 patients and bone–patellar tendon–bone grafts in 185 patients. Of the 610 cases reconstructed with the knee flexor tendon, 9 had complex ligament injuries, 22 had meniscal locking, 4 had revision, 59 had bilateral injuries, 61 had previous fractures or surgery in the lower limb, and 10 had difficulty communicating in Japanese. In addition, 16 patients could not provide consent, 37 patients had difficulty coming to the hospital because of relocation, and 3 patients had to change their schedule because of a change in the surgical technique. Thus, 389 patients were included in the study: 55 patients in the LOE group and 334 patients in the no-LOE group (Figure 2).

Flowchart of patient inclusion and study groups. ACLR, anterior cruciate ligament reconstruction; HHD, heel height difference; LOE, loss of knee extension.
Among the 389 patients, injury to the ACL occurred during participation in basketball (n = 94), volleyball (n = 45), soccer (n = 40), handball (n = 30), skiing (n = 29), futsal (n = 28), badminton (n = 11), rugby (n = 10), dance (9), judo (n = 7), and other sports (n = 52); during falls and traffic accidents (n = 17); other (n = 11); and unknown (n = 6). The median Tegner activity score was 7.0 (IQR, 4.0-8.0). The patients comprised 208 women and 181 men; 234 did not have meniscal sutures and 155 had meniscal sutures. The patient characteristics are shown in Table 1. Comparison of age at reconstruction, height, weight, and waiting time before surgery between the no-LOE and LOE groups revealed significantly higher age (P = .021) and weight (P = .004) in the LOE group (Table 1).
Characteristics of the Study Patients a

a Data are reported as median [interquartile range] or n (%). Boldface P values indicate a statistically significant difference between groups (P < .05). BMI, body mass index; LOE, loss of knee extension.
The percentage of patients who achieved an HHD <2 cm by 12 months after ACLR was 86.2% (288/334) in the no-LOE group and 61.8% (34/55) in the LOE group (P < .001). The incidence of LOE was 13.8% in the no-LOE group and 38.2% in the LOE group. The absolute risk difference was 24.4%. Table 2 shows the median number of days observed to achieve an HHD <2 cm, and the HHD values from preoperatively to 12 months postoperatively in both groups. Proportional hazards analysis showed that the hazard ratio for achieving an HHD <2 cm by 12 months after ACLR was 2.79 (95% CI, 1.95-4.02) for patients with preoperative LOE (P < .001) (Table 3). Figure 3 shows the survival curve of the percentage of patients with postoperative HHD ≥2 cm. In the no-LOE group, approximately 50% of patients in the 100-day postoperative period, 15% in the 200-day postoperative period, and 15% in the 12-month postoperative period remained limited in extension. On the other hand, in the LOE group, 80% of patients in the 100-day postoperative period, 50% of patients in the 200-day postoperative period, and 30% of patients in the 12-month postoperative period remained limited in extension.
HDD From Preoperatively to 12 Months Postoperatively a

a Data are reported as median [interquartile range]. Boldface P values indicate a statistically significant difference between groups (P < .05). HHD, heel height difference; LOE, loss of knee extension.
Proportional Hazards Analysis Model for Predicting Postoperative LOE a

a Boldface P values indicate statistical significance (P < .05). LOE, loss of knee extension.
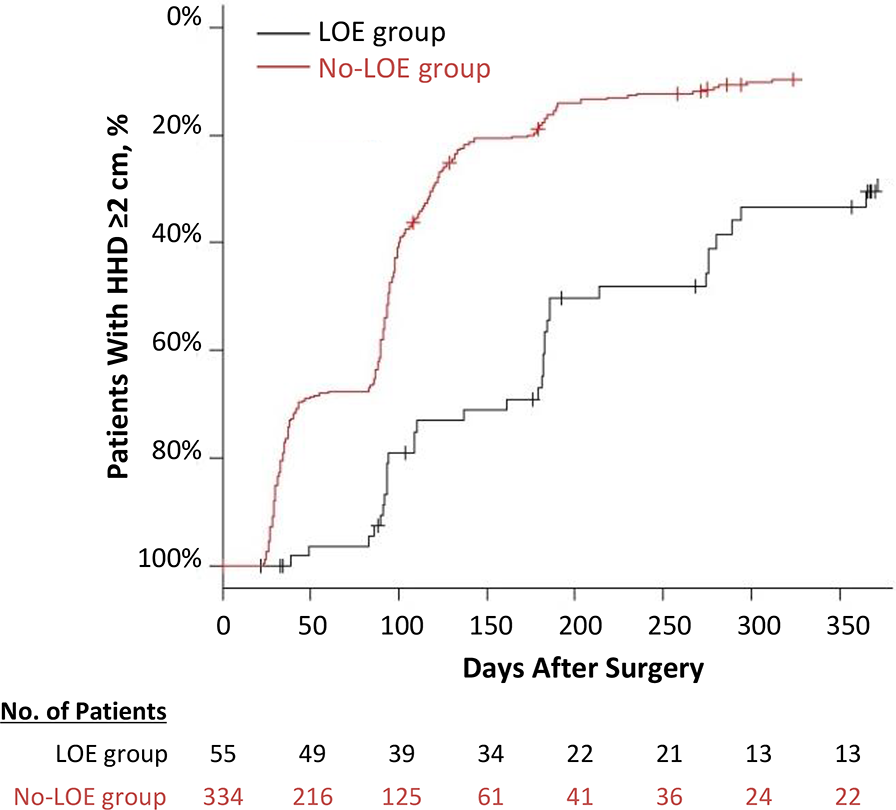
Survival curve of percentage of patients with a heel height difference (HHD) ≥2 cm after adjusting for sex, age, time from injury to surgery, and presence of meniscal sutures. LOE, loss of knee extension.
Discussion
In the present study, we investigated the influence of preoperative LOE on postoperative LOE 12 months after ACLR. The rate of achieving an HHD <2 cm by 12 months after surgery was 86.2% in the no-LOE group and 61.8% in the LOE group (P < .001). The absolute risk difference was 24.4%. A proportional hazards analysis with the presence or absence of preoperative LOE as an independent variable; with age, sex, BMI, waiting time to surgery, and presence or absence of meniscal sutures as adjustment variables; and with or without achieving an HHD <2 cm as the dependent variable resulted in a hazard ratio of 2.79. The observation period for achieving an HHD <2 cm was 92.5 days in the no-LOE group and 183 days in the LOE group.
Some reports indicate that preoperative LOE affects postoperative LOE, with the incidence of postoperative LOE ranging from 11.1% to 35%. 7,14,15,18,29 McHugh et al, 15 comparing the preoperative range of motion in 3 groups of patients (0°, 1-4°, and ≥5°), reported that the 0° group had a significantly lower incidence of LOE than the other 2 groups. The results of the present study are consistent with previous reports, but the previous reports did not begin assessing LOE until 12 months after ACLR and included only a small number of cases.
LOE is related to muscle strength and performance. Preoperative LOE is one of the factors that affects LOE at 4 weeks after surgery. 14 LOE at 6 weeks and 3 months predicts quadriceps strength at 6 months after ACLR. 9 Weak quadriceps strength is associated with poor knee performance, 20 anterior knee pain, 17 a low Lysholm score, 4 and knee OA. 3 Therefore, improving the preoperative LOE may reduce the occurrence of postoperative LOE and decrease postsurgical problems.
Several causes of LOE are suggested, including preoperative LOE, 28 poor graft tunnel positioning, 2 and inappropriate postoperative rehabilitation. 25,26 Therefore, Shelbourne and Nitz 25,26 advocated accelerated rehabilitation to achieve full extension in the early postoperative period, and reported good clinical results. In addition, hamstring contracture is a factor in cyclops syndrome. 19 In the present study, we started interventions, including hamstring relaxation, for LOE the day after surgery. Because standard postoperative rehabilitation protocols were followed, 25,26 we believe that the postoperative LOE is strongly influenced by the preoperative period.
As stated above, the observation period for achieving an HHD <2 cm was shorter in the no-LOE group compared with the LOE group. The time to start jogging again is approximately 3 months after surgery, 11 and clinically, the patient must have no swelling or pain, and good range of motion and muscle strength. In a study of 100 patients, the inability to return to sports after ACLR was because of pain, fear of reinjury, muscle weakness, and LOE. 6 In the present study, in the no-LOE group, the knee extension limitation was expected to improve within approximately 3 months after surgery, and the conditions for starting jogging according to the protocol may be improved. The preoperative LOE group, however, required approximately 6 months to resolve the limitations in extension, which may interfere with the protocol progression and delay the return to sport.
Limitations
This study has some limitations. First, the patients were observed for up to 12 months, but longer observation is needed to investigate the association between preoperative LOE and knee OA. Second, strength and lower extremity function scores, and the relationship between the timing of starting jogging and return to sports was not assessed. Third, the impact of the frequency of rehabilitation after hospital discharge was not considered. Finally, only patients with initial reconstruction using the hamstring tendon were included; patients with bone–patellar tendon–bone grafts and patients with revision ACLR were not studied.
Conclusion
Study findings indicated that preoperative LOE is associated with postoperative LOE at 12 months after ACLR.
Footnotes
Acknowledgment
The authors express their gratitude to Mio Funato, Yui Masuoka, Ryuta Tanihara, Syota Sasaki, and Yusuke Shinchi, physical therapists at the Department of Rehabilitation, Juko Memorial Hospital, for their cooperation in obtaining the measurements used to conduct this study.
Final revision submitted September 10, 2022; accepted October 21, 2022.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Seijoh University (reference No. 2018C15).