
Abstract
Background:
Despite increased awareness for promoting diversity, orthopaedics remains one of the least diverse specialties. Studying health care providers in women’s professional sports provides a unique opportunity to analyze gender and racial diversity.
Hypotheses:
There would be low female and minority representation across the various women’s professional sports leagues. There would be an increased number of female head certified athletic trainers (ATCs) when compared with head team physicians (HTPs).
Study Design:
Cross-sectional study.
Methods:
We evaluated the perceived race and sex of designated HTPs and ATCs in the Women’s National Basketball Association, National Women’s Soccer League, and National Women’s Hockey League. Type of doctorate degree, specialty, and years in practice were also collected. Kappa (κ) coefficient measurements were used to determine interobserver agreement on race. Categorical and continuous variables were analyzed using chi-square and t tests, respectively.
Results:
There were significantly more female ATCs than female HTPs (74.1% vs 37.5%; P = .01). Minority representation between HTPs and ATCs was not significantly different (20.8% vs 40.7%; P = .13). Black HTPs (12.5%) and Black ATCs (22.2%) composed the largest proportion among the minority groups. There was high interobserver agreement of perceived race across HTPs (κ = 1.0) and ATCs (κ = 0.95).
Conclusion:
Although there were more female ATCs than HTPs in women’s professional sports leagues, both cohorts lack perceived racial diversity. These data suggest an opportunity for diversification in medical and training staff of women’s professional sports.
Patient-physician gender and racial concordance has become recognized as an important factor in a patient-physician relationship, and as such, discordance may contribute to health care disparities. 4,9,31 Perceived personal similarity is associated with higher ratings of trust, satisfaction, and intention to adhere to physician recommendations. 35 Despite the growing importance placed on these issues, the American Academy of Orthopaedic Surgeons (AAOS) has revealed that orthopaedic surgery is the least diverse of any surgical specialty. 2 When compared with the overall US population, there is an overrepresentation of Caucasian and Asian American physicians within the field, while Black, Hispanic/Latino, and Native American physicians remain underrepresented. 28 Although there has been some improvement in diversity in recent years, this change is not proportional to the increase in minorities or women entering medicine. In a 2018 AAOS report, only 15.3% of orthopaedic surgeons identified as a minority and just 7.6% as female. 2 In contrast, in 2019 the Association of American Medical Colleges reported that 44% of active physicians identified as a minority and 36% as female. 3
The underrepresentation of minorities and women within orthopaedic surgery may contribute to the perpetuation of health disparities. Patient-physician concordance can foster more genuine patient-provider relationships, which improve communication and decision making between patients and physicians. 7,8,30 Discordance in race—or a difference in shared outward physical characteristics and some commonalities of culture and history—has been shown to negatively affect patients’ treatment and health outcomes across various fields of medicine. 4,9,18,31 Discordance of gender may also play a role. Greenwood et al 10 evaluated 581,845 emergency department admissions for acute myocardial infarctions at a Florida hospital between 1991 and 2010 and found that female patients treated by female physicians had a 2- to 3-times greater survival rate compared with those treated by male physicians. While patient-physician concordance is not necessarily essential for patients to receive the best quality of care, these studies support improved representation across all fields of medicine, which may enhance outcomes for a wider range of patients.
Orthopaedic surgeons have a prominent role in various professional sports leagues. However, disparities exist in the diversity of orthopaedic surgeons caring for these athletes. In a study of team physicians for the National Basketball Association (NBA) and Women’s National Basketball Association (WNBA) between 2009 and 2019, Hinkle et al 11 found that just 3 (2.4%) of the 125 team physicians in the NBA identified as female and 8 (28.6%) of 28 in the WNBA. Given the increased awareness regarding diversity in ownership and coaching positions among various leagues, coupled with the lack of representation within orthopaedic surgery, it is important to further analyze the diversity of medical providers within professional sports leagues. 13 –17
Maintaining athletes’ health and wellness is a priority for the owners, coaches, physicians, and athletic trainers of sports teams. Yet, there is little research on the demographic makeup of the health professionals who care for some of the world’s best athletes. The aim of this study was to characterize the perceived racial and gender demographics of the head team physicians (HTPs) and head certified athletic trainers (ATCs) for the major women’s professional sports leagues. We hypothesized that ATCs and HTPs would demonstrate low rates of minority and female representation. Furthermore, we hypothesized that ATCs would have a greater percentage of positions filled by women than HTPs.
Methods
Data Collection
The WNBA, National Women’s Soccer League (NWSL), and National Women’s Hockey League (NWHL) were selected as the women’s professional sports leagues to study, based on each league’s consistent staffing of the HTP and ATC positions as well as their high level of visibility among professional women’s sports. Two independent investigators (O.A. and A.J.W.; both orthopaedic surgery residents) performed online searches for each team in those leagues. Using the leagues’ websites and publicly available team information, we identified the medical and training staff and included those designated as the HTP and ATC in the data collection. When a team had >1 HTP or ATC, all individuals were included for analysis.
After the identification of each team’s HTP and ATC, the same 2 observers reviewed photographs of these individuals and assigned a perceived race. The race designations reflect those utilized by the AAOS 2 : Caucasian, Black, Asian, Hispanic/Latino, and Native American. These designations are similar to the categories used by the US census and were therefore deemed reasonable to employ for a US-based study population. 1 In our study, those individuals who were designated as non-Caucasian were considered part of the minority cohort. These methods were chosen to capture the entire landscape of perceived diversity of the study population. Direct survey techniques, although more accurate on an individual basis, may be incomplete on a broader cross-sectional level as direct surveys are often fraught with low response rate and response bias that can skew results. 2,5,19,20,38
The gender of each HTP and ATC was determined by the 2 independent investigators (O.A. and A.J.W.) using publicly available biographical information and photographs when self-reported data were unavailable. Gender was determined using binary designation of male or female as previously described. 11,37 Additional data were collected on the HTP, including the type of doctorate degree received, the medical or surgical specialty, as well as the number of years in practice based on the year of residency completion or fellowship training, when applicable. The study was exempt from instituional review board review.
Statistical Analysis
Kappa coefficients were calculated to assess interobserver agreement on race, and values were categorized according to the Landis and Koch method: 12 0 signified no agreement; 0.10 to 0.20, slight agreement; 0.21 to 0.40, fair agreement; 0.41 to 0.60, moderate agreement; 0.61 to 0.80, substantial agreement; 0.81 to 0.99, near-perfect agreement; and 1, perfect agreement. Chi-square tests were used to analyze categorical variables, and continuous variables across leagues were analyzed using independent t tests. Statistical analyses were performed using Prism 7 software (Version 7.0a; GraphPad Software, Inc) with statistical significance defined as P < .05.
Results
HTP Demographics
Across all leagues studied, 24 HTPs were identified from 27 teams. There was high interobserver agreement of perceived race across HTPs (κ = 1.0). Three teams did not have an HTP designated when this study was performed. Findings indicated that minority representation was 20.8% (5/24 HTP positions) (Figure 1A, Table 1), with Black HTPs composing the largest proportion at 12.5% (3/24) of the minority cohort. The league with the highest percentage of perceived minority HTPs was the WNBA at 30.0% (3/10), all of whom were Black. The NWSL had the lowest minority percentage at 10.0% (1/10) (Table 2). There were variable minority compositions among the 3 leagues; however, there were no significant differences in the total HTP minority percentage across the leagues (P = .53). In regard to the gender of the HTPs, 37.5% were female (9/24 HTP positions) (Figure 2A). Of the HTPs who were perceived as minority, 20% (1/5) were female as compared with the 42.1% (8/19) of Caucasian HTPs who were female, although this difference was not significant (P = .36).

Percentage of (A) head team physicians and (B) head certified athletic trainers (ATCs) by race.
Comparison of HTPs and ATCs by Race a

a Data are reported as % (No.). ATC, certified athletic trainer; HTP, head team physician.
HTP and ATC Race Percentage by League a

a ATC, certified athletic trainer; HTP, head team physician; NWHL, National Women’s Hockey League; NWSL, National Women’s Soccer League; WNBA, Women’s National Basketball Association.
b There were no Native American HTPs or ATCs.

Percentage of (A) head team physicians and (B) head certified athletic trainers (ATCs) by gender. * denotes P < .05 comparing female percentage between physicians and ATCs.
There was no significant difference in the number of years in practice between minority HTPs (mean ± SD; 14.0 ± 7.8) and their Caucasian counterparts (15.3 ± 7.7; P = .74) (Figure 3A). Similarly, there were no differences in years in practice by gender (male, 16.5 ± 7.5; female, 12.7 ± 7.4; P = .24) (Figure 3B). In terms of HTP specialty, 54.2% (13/24) were trained as orthopaedic surgeons across all the leagues. The league with the greatest percentage of orthopaedic surgeon HTPs was the NWSL at 60.0% (6/10), with the WNBA (5/10) and NWHL (2/4) with only 50.0% (P = .89) (Table 3). The nonorthopaedic specialties included family medicine, physical medicine and rehabilitation, and pediatrics. While 66.7% (10/15) of male HTPs tended to be orthopaedic surgeons, just 33.3% (3/9) of female HTPs were orthopaedic surgeons, although this difference was not significant (P = .11) (Table 4). In addition, there were no differences in HTP specialty by race, with 60.0% (3/5) of minority HTPs being orthopaedic surgeons as compared with 52.6% (10/19) of Caucasian HTPs (P = .77).
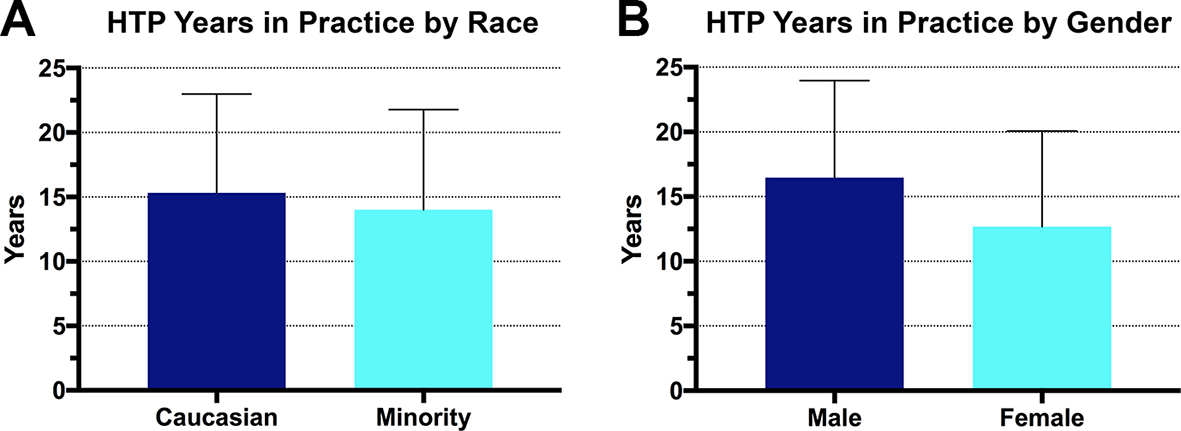
Years that head team physicians (HTPs) spent in practice by (A) race and (B) gender. Error bars represent SD.
Comparison of HTPs With an Orthopaedic Specialization by League a

a Data are reported as % (No.). HTP, head team physician; NWHL, National Women’s Hockey League; NWSL, National Women’s Soccer League; WNBA, Women’s National Basketball Association.
Comparison of HTPs With an Orthopaedic Specialization by Gender a
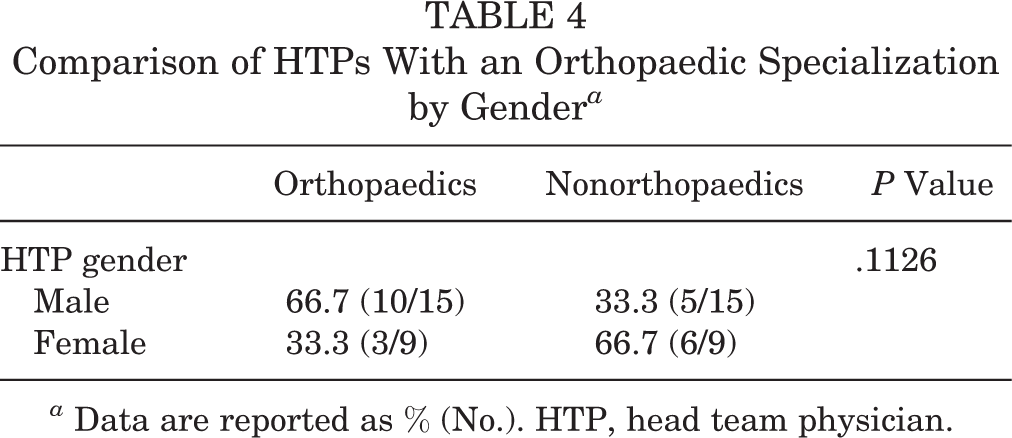
a Data are reported as % (No.). HTP, head team physician.
Comparison of Race Between HTPs and ATCs
An overall 27 ATCs were identified across all the leagues studied, with each team designating 1 ATC. Interobserver agreement for ATC race designations was 0.95, indicating near-perfect agreement between the 2 independent observers. In total, there was 1 instance of disagreement for race designation, which required resolution by a third independent observer (A.D.). In total, minorities represented 40.7% (11/27) of ATC positions across all leagues, with Black ATCs accounting for greatest percentage at 22.2% (6/27) (Figure 1B, Table 1). Although there was a greater percentage of total minority ATCs (40.7%) versus total minority HTPs (20.8%; 5/24), this difference was not significant (P = .13). In addition, we found no differences when we assessed the composition of ATC and HTP minority cohorts across all leagues studied (P = .19). The league with the highest percentage of minority ATCs was the WNBA at 58.3% (7/12), with the minorities occupying 20.0% (1/5) and 30.0% (3/10) of NWHL and NWSL ATC positions, respectively. Within each league, there were no significant differences in minority percentage between ATCs and corresponding HTPs (Table 5).
Comparison of Minority HTPs and ATCs by League a
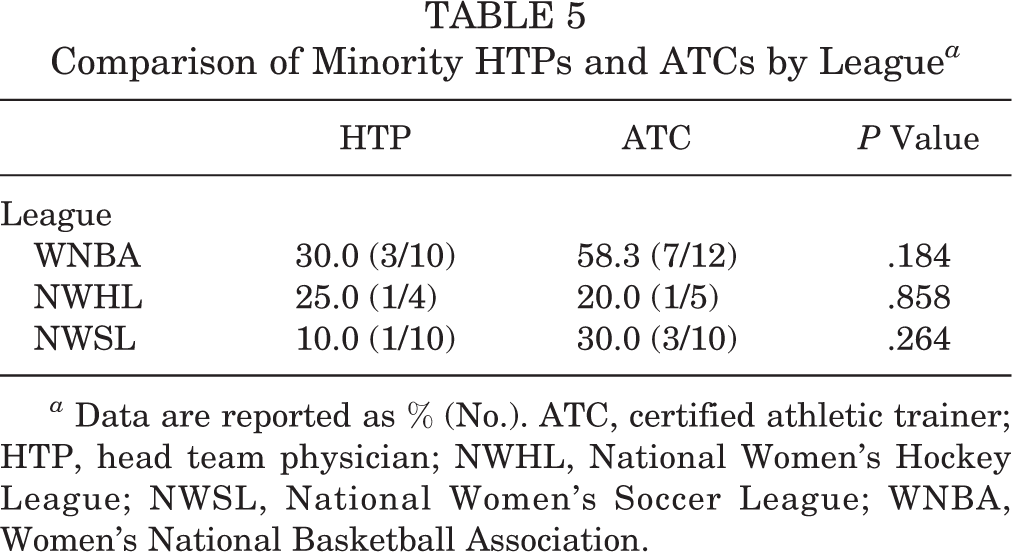
a Data are reported as % (No.). ATC, certified athletic trainer; HTP, head team physician; NWHL, National Women’s Hockey League; NWSL, National Women’s Soccer League; WNBA, Women’s National Basketball Association.
Comparison of Gender Between HTPs and ATCs
Women held 74.1% (20/27) of total ATC positions, which was significantly greater than the 37.5% (9/24) of HTPs who were female (P = .01) (Figure 2B). The majority of ATCs were female in each of the 3 leagues, with the highest percentage in the NWSL at 80.0% (8/10), followed by the WNBA and NWHL at 75.0% (9/12) and 60.0% (3/5), respectively. When compared within each league, there was a significantly higher rate of female representation among the NWSL’s ATC staff as compared with its HTPs (80.0% vs 30.0%; P = .03) (Table 6). The other 2 leagues did not demonstrate significant differences in their percentages of female-held ATC and HTP positions.
Comparison of Female HTPs and ATCs by League a
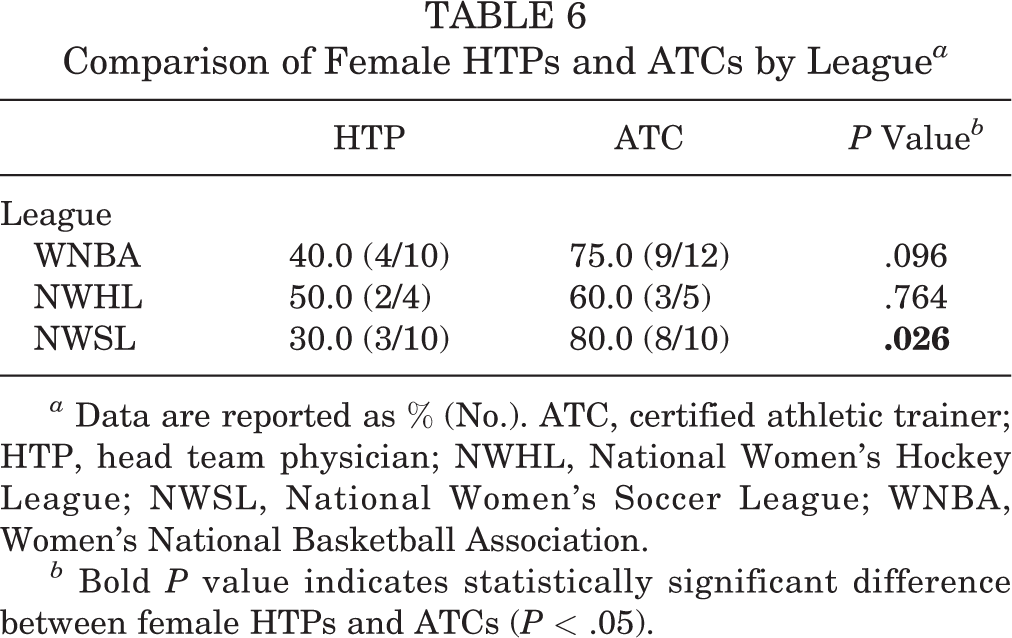
a Data are reported as % (No.). ATC, certified athletic trainer; HTP, head team physician; NWHL, National Women’s Hockey League; NWSL, National Women’s Soccer League; WNBA, Women’s National Basketball Association.
b Bold P value indicates statistically significant difference between female HTPs and ATCs (P < .05).
Discussion
In this study, we evaluated the rates of perceived minority and female representation among women’s US professional sports leagues in terms of HTP and ATC positions. The majority of HTPs were Caucasian at 79.2%. Among ATCs, a higher percentage of this position was held by minorities at 40.7%. There were no significant differences in the composition of minority cohorts across leagues or in the perceived minority representation between HTP and ATC staff within each league. Women held a significantly greater proportion of ATC positions (74.1%) than HTP positions (37.5%; P = .01). The majority of ATC positions within each of the 3 leagues studied was occupied by women. Comparing female representation of the 2 job classes within each league revealed a higher percentage of female ATCs than HTPs in the NSWL (80.0% vs 30.0%; P = .03). Of note, HTPs demonstrated no significant differences based on years in practice by race or sex. Moreover, differences in HTP specialty by race and sex did not reach significance.
The field of US professional sports offers an intriguing opportunity to study diversity, as there has historically been a high percentage of minority players within these leagues and they represent a highly publicized aspect of society. 13 –17 Because of their increased visibility, there is great interest into the inner workings of these franchises worldwide. However, the current literature has a paucity of data on the topic of gender and race demographics for staff of women’s professional sport teams. In a cross-sectional study in 2018, O’Reilly et al 24 studied the percentage of female team physicians across the WNBA, NBA, National Football League, Major League Baseball, and select National Collegiate Athletic Association Division I conferences using an online search of publicly available data and found that 12.7% of team physicians were women. Specifically, the authors reported that the WNBA had the highest rate of female team physicians at 32.4%, slightly less than the 40.0% in our study. This may indicate an increase in female representation among team physician between 2018 and 2020, although O’Reilly et al examined all team physicians, including those outside the designated “head team physician” position, which may account for the observed difference.
As part of the Racial and Gender Report Card 2021 series, Lapchick 17 reported that 53.8% of head athletic trainers in the WNBA were people of color, with those of Black racial background composing the largest proportion at 38.5%; 7.7% were Hispanic/Latino athletic trainers. In addition, this previous study found that women held 76.9% of the head athletic trainer positions. No such analysis was performed on the NWHL or the NWSL. These figures are comparable to those in our study, with WNBA demonstrating 58.3% perceived minority representation among its ATC staff: 50.0% Black, 8.3% Hispanic/Latino, and 75.0% female. These previous studies did not report on race demographics for team physicians. Therefore, to the best of our knowledge, our study is the first to report on the racial demographics of team physicians in women’s professional sports.
Comparing the results of the current study with the rates of female and minority representation within men’s professional sports in terms of medical and athletic training staff may provide insights into patterns of diversity of these leagues. Hinkle et al 11 examined NBA team physician demographics between 2009 and 2019 and found that only 2.4% (3/125) during that period were female, which represents a markedly lower rate than the 37.5% seen in our current study. In a similar study performed in 2021 by our group, we examined the perceived diversity the HTPs and ATCs of the 5 major US men’s professional sport leagues—NBA, Major League Baseball, National Football League, National Hockey League, and Major League Soccer—using an internet search of publicly available data and race and sex designations according to 2 independent observers. 37 In that study, minorities held 15.5% (24/155) of HTP positions and 20.7% (31/150) of ATC positions. Of the 155 HTPs, just 6 were women (3.9%). Female representation was even lower among the ATCs in the men’s leagues, with only 2 (1.3%) of 150 positions being filled by women. These results suggest that the physician and training staff in women’s sport professional leagues tend to be more diverse than their male counterparts. However, a similarly low rate of minority HTPs remains among women’s and men’s professional sports leagues.
When compared with men’s professional leagues, women’s professional leagues appear to have higher minority and female representation in their HTP and ATC personnel. However, when the composition of the minority cohort is analyzed, certain groups still lack representation. For example, Asian and Hispanic/Latino staff accounted for just 4.2% of the HTP workforce, and no Asian ATCs were identified per our analysis. According to the most recent US census data, Hispanic/Latino individuals compose 18.5% of the general population, a far greater proportion than the 4.2% of HTPs in our study. 1 To further contextualize the HTP results, one must consider potential bias in hiring practices more broadly in such organizations. 13 –17 In addition, the national demographic composition of orthopaedic surgeons and other represented specialties likely plays a role in the subset that goes on to become HTPs.
Historically, orthopaedic surgeons have been recruited as HTPs given their expertise and the types of injuries that athletes tend to incur. Therefore, the amount of diversity among HTPs is likely some degree a reflection of the orthopaedic workforce nationally. The AAOS stated in a recent biannual report on diversity that 84.7% of orthopaedic surgeons nationally were Caucasian, followed by Asian at 6.7%. 2 Hispanic/Latino and Black surgeons composed 2.2% and 1.9% of the workforce, respectively. In addition, only 7.6% of surgeons were women. Other studies have examined diversity in orthopaedics at various levels of training. 21 –25,27 For example, Poon et al 25 –27 found that between 2005 and 2016, the mean female and minority representation among orthopaedic surgery residents was 13.3% and 25.6%, respectively. These data suggest that orthopaedics has remained one of the least diverse specialties. The reasons for this are likely multifactorial, including factors such as bias in hiring as well as the possible discouraging effect that baseline underrepresentation may have on potential future minority and female applicants into the field. The results in our study indicate that HTPs in women’s professional sports are more diverse in terms of female representation (37.5%) than the orthopaedic surgeon cohort nationally but are likely on par in terms of minority representation (20.8%). One should consider, however, that just 54% of HTPs had orthopaedic training. The large contribution of nonorthopaedic physicians to the HTP workforce may be one factor contributing to the higher rate of female HTPs, although we did not find any significant differences in HTP specialty by race or gender. 3
Roter et al 29 performed a systematic review to quantify the effects of physician gender on the various parameters of medical visits and found that female providers offered significantly more positive talk and partnership behaviors with their patients. In a large matched cohort study evaluating the health outcomes of 104,630 patients undergoing surgery by 3314 surgeons (774 female, 2540 male), Wallis et al 36 stated that those patients who were treated by female surgeons demonstrated a significant decrease in 30-day mortality as compared with those treated by male surgeons. In addition, multiple studies have reported on correlations among gender and race concordance of the patient-provider relationship, improved physician-patient communication, and greater intent to follow treatment recommendations. 7,8,30,32,33,35 Taken together, these studies and ours may further encourage the hiring of a more diverse set of HTPs, especially those who better align with the demographics of the female professional athletes for whom they care. Whether improved demographic concordance among HTPs, ATCs, and female professional athletes is correlated with improved health outcomes of the athletes will be the focus of subsequent studies.
Limitations
This study has limitations. First is the relatively small sample size in terms of leagues and teams within each league in our analysis. Other potential women’s professional sports leagues were excluding owing to the high rate of unfilled HTP and ATC positions within them or a substantial lack of publicly reported information about these job positions generally. Historical differences in the shorter duration in which these leagues were established, less public visibility, and fewer resources available to them vs men’s professional sports all likely play a large role in the discrepancy. 6,34 Our study aimed to capture and quantify these metrics with the currently available data. Furthermore, gender and racial designations were made by 2 independent observers using publicly available information on team websites, online databases, online searches, and photographs. Similar methods of using publicly available data were used in 3 similar studies, including a recent study examining similar variables among the major men’s professional leagues. 11,37 Moreover, the perfect and near-perfect interobserver agreement for the HTP and ATC race designations, with only 1 instance of disagreement across both cohorts (resolved by a third independent observer), lends confidence to the accuracy of our designations. However, it is possible that an incorrect designation may have been made as compared with what an individual’s self-identified racial background may be. This includes risk of misdesignation of a minority individual as Caucasian, which could result in a lower rate of racial minorities. In addition, those with multiracial backgrounds could be missed in the analysis.
In terms of gender, we used a binary male or female designation, which may not be correct for those who identify as nonbinary. However, these limitations are not fundamentally at odds with the aim of this study, which was to quantify the perceived diversity of this specific study population. Alternative methods that rely on direct survey methods are often severely limited by the low response rates, which can result in the volunteer and nonresponse bias that can skew results. 2,5,19,20,38 We aimed to characterize the whole perceived diversity landscape of the women’s professional leagues included in this study, of which survey may not be as effective given the shortcomings listed here. To our knowledge, this is the first study to examine race and sex demographics among these women’s leagues; therefore, it may serve as the benchmark for follow-up studies with the potential for participation directly from the leagues with more robust data collection.
Conclusion
This study demonstrates that ATCs in women’s professional sports have a higher rate of female representation than their HTP counterparts. ATCs tend to be more racially diverse, although not significantly more than the HTPs. The overall lack of female and minority representation among HTPs may be influenced by national physician workforce trends, specifically within orthopaedics. Improving the diversity of the leadership staff within these various leagues may lead to improved trust, communication, and outcomes for the many athletes who often experience patient-provider discordance. In addition, improving representation offers added benefits for health care professionals, such as promoting an inclusive environment as well as supporting further recruitment of those historically underrepresented in medicine to orthopaedics. The findings within this study serve as a reference point for future research to track the trends of diversity among women’s professional sports leagues and inform the evaluation of diversity, equity, and inclusion efforts over time.
Footnotes
Final revision submitted September 27, 2022; accepted October 26, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: K.J.J. has received education payments from Arthrex and Micromed; consulting fees from Linvatec; nonconsulting fees from Arthrex, Linvatec, and Vericel; and honoraria from Joint Restoration Foundation and Musculoskeletal Transplant Foundation. B.T.F. has received education payments from Evolution Surgical. N.K.P. has received education payments from Evolution Surgical and consulting fees from OrthoPediatrics. S.E.W. has received education support from Evolution Surgical and consulting fees from Encore Medical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.