
Abstract
Background:
It is clear that the anterolateral ligament has an important role in rotational knee stability. However, whether patients undergoing anterior cruciate ligament (ACL) reconstruction (ACLR) can benefit from anterolateral augmentation (ALA) is still controversial.
Purpose:
To compare the effects of isolated ACLR versus ACLR combined with ALA (ACLR+ALA) on clinical outcomes and knee stability.
Study Design:
Systematic review; Level of evidence, 1.
Methods:
The methodology followed PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. A literature search of the PubMed, Embase, and Cochrane Library Central Register of Controlled Trials databases was undertaken to identify all randomized controlled trials (RCTs) comparing isolated ACLR with ACLR+ALA for the treatment of ACL injuries in the last 15 years. The Cochrane Collaboration risk-of-bias tool and the revised Jadad scale were utilized by 2 independent reviewers to determine the quality of RCTs. Relevant data were extracted and compared between procedures, and heterogeneity across the RCTs was assessed using the I 2 statistic.
Results:
The initial search yielded 849 articles. A total of 14 studies (1850 patients; 941 ACLR and 909 ACLR+ALA) satisfied the eligibility criteria for the meta-analysis. There were no significant differences between the procedures in terms of patient-reported outcomes (International Knee Documentation Committee score, Tegner score, Knee injury and Osteoarthritis Outcome Score) or return-to-sport rates. However, patients who underwent ACLR+ALA had better knee stability based on the pivot-shift test (risk ratio [RR], 1.06 [95% CI, 1.02 to 1.10]; P = .0008), Lachman test (RR, 1.03 [95% CI, 1.00 to 1.07]; P = .04), and side-to-side difference in anterior laxity (standardized mean difference, –0.55 [95% CI, –0.98 to –0.12]; P = .01) as well as a lower incidence of graft failure (RR, 0.30 [95% CI, 0.19 to 0.45]; P < .01) compared with patients who underwent isolated ACLR.
Conclusion:
ALA can be considered as a reinforcement of ACLR to improve anteroposterior and anterolateral rotational stability of the knee and reduce the risk of failure. The patient-reported outcomes of isolated ACLR were similar to those of ACLR+ALA, and both procedures provided improved knee function.
An anterior cruciate ligament (ACL) tear is a serious injury that can result in residual knee instability, chronic pain, secondary meniscal injuries, and knee osteoarthritis. 4,31,58 Arthroscopic reconstruction is the standard approach and provides good or excellent results in more than 90% of patients. However, a percentage of instability ranging from 15% to 35% during follow-up is reported in the literature 8,15 ; in particular, residual instability as revealed by a positive pivot-shift test finding has been reported, suggesting that other support structures may affect stability. Residual rotational instability after ACL reconstruction (ACLR) is multifactorial, but residual anterolateral rotatory laxity is a potential contributing factor for recurrent injuries. 5,8
The function of controlling knee internal rotation may be performed by the anterolateral complex of the knee, especially the anterolateral ligament (ALL). 22 Recent magnetic resonance imaging (MRI) studies have shown that concomitant ALL injuries can be identified in the majority of acutely ACL-injured knees, 11,16,57 and this rate was even higher on 3-dimensional MRI. Some studies have shown that the ALL has a synergic effect on controlling rotational stability of the knee, together with the ACL. 24,48 Other studies, however, have shown that concomitant ALL and ACL injuries in knees have no effect or a minor effect on rotatory knee laxity. 2,33 Temponi et al 51 demonstrated via MRI that the ALL has intrinsic healing potential after nonoperative treatment. Therefore, the structure and function of the ALL remain controversial, as does its proposed role in aiding the restraint of internal rotation in ACL-injured knees. 9,28,35
Several controlled laboratory studies have illustrated the relationship among rotational instability, the ALL, and the recovery of native knee kinematics by performing additional lateral extra-articular reconstruction. 10,11,20,34,43 Because some ACL injuries are accompanied by anterolateral complex damage, resulting in increased rotational instability, 12,26,37 the addition of an extra-articular procedure to intra-articular ACLR may maintain the stability of the rotational knee joint and decrease forces on the graft. 47,55 The combined ACLR and anterolateral augmentation (ALA) procedure (ACLR+ALA) is an effective and safe solution, leading to good functional outcomes in patients with ACL injuries. 15,24 Additionally, Sonnery-Cottet et al 45 suggested that ALA has a protective effect on medial meniscal repair performed at the time of ACLR. However, both cadaveric and clinical studies have shown a high risk of tunnel convergence with ACLR+ALA, which may compromise graft fixation and integrity or lead to graft damage, thus resulting in poor clinical outcomes. 21,41 In addition, there is a concern regarding overconstraint of the knee with ACLR+ALA. 40 The extra-articular ALA procedure requires more technical support and an additional incision and is more time consuming and expensive. 38 The loss of knee motion and the increased incidence of patellofemoral crepitation might also be associated with certain extra-articular techniques. 32 Furthermore, some clinical studies have failed to show the superiority of ACLR+ALA over isolated ACLR. 52
The purpose of this systematic review and updated meta-analysis was to evaluate clinical results and knee stability by analyzing high-quality studies between 2006 and the present. We hypothesized that ACLR+ALA would result in (1) increased stability as measured by the pivot-shift and Lachman tests, (2) better knee function as evaluated by the International Knee Documentation Committee (IKDC) or Tegner score, and/or (3) a lower graft failure rate.
Methods
Literature Search
In this study, we followed the recommendations of the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement. 25 The search engines utilized included PubMed, Embase, and the Cochrane Library. The search protocol used was consistent with that reported in a published study. 61 Specifically, the retrieval method was divided into 2 parts. First, the keywords “ACL,” “anterior cruciate ligament,” and “anterolateral ligament” were searched in the 3 databases separately to identify meta-analyses and systematic reviews evaluating the outcomes between ACLR and ACLR+ALA between database inception and May 20, 2022 (see Appendix Table A1 for details). Then, original randomized controlled trials (RCTs) in those systematic reviews or meta-analyses were further screened. Second, the databases were searched again using the same search strategy as in the first part to identify additional RCTs published between January 1, 2006, and May 20, 2022. The publication languages were limited to English and Chinese for accuracy of the data extraction process.
Inclusion and Exclusion Criteria
The inclusion criteria for enrolling studies were RCTs with prospective data collection that compared primary ACLR with or without ALA; studies reporting clinical outcomes as measured by postoperative IKDC scores; and/or studies of graft laxity as measured by the arthrometric side-to-side difference (SSD), Lachman test, or pivot-shift test among surviving grafts. The exclusion criteria were as follows: retrospective comparative studies, case reports, narrative reviews, or imaging reviews; studies of multiligament injuries, other concomitant knee disorders that required surgery, or revision surgery; studies failing to clearly report the data that met our interest; and animal or biomechanical studies. When articles that reported details of the same patient cohort were identified, the most recent data were utilized. Disagreements on study selection were resolved by a discussion and consensus between the 2 reviewers (S.L and Z.Z).
Data Extraction
Data from eligible studies were independently extracted by 2 authors (S.L. and Z.Z.) based on predefined selection criteria and included sample size, patient age, length of follow-up, and details of the ACLR and ALA techniques. The primary outcomes were failure rates (including revision surgery and graft rupture) and knee stability as defined by the pivot-shift test, Lachman test, and SSD in anterior laxity between the injured knee and the contralateral healthy knee. Outcome measures (IKDC score, Tegner score, Knee injury and Osteoarthritis Outcome Score [KOOS], and return-to-sport [RTS] rate) were also extracted. Any discrepancies were resolved by a third author (W.F.).
Quality and Risk-of-Bias Assessment
The methodological quality and risk of bias of the eligible studies were independently assessed by 2 reviewers (S.L. and Z.Z.). The revised Jadad scale was utilized for the estimation of study quality by the 2 independent reviewers. 30 Specifically, an article was considered to be of poor quality if the revised Jadad score was 0 to 3 points and of high quality if the score was 4 to 7 points. The risk of bias for all included studies was assessed using the Cochrane Collaboration risk-of-bias tool, which contains 7 items as follows: random sequence generation (selection bias), allocation concealment (selection bias), blinding of participants and personnel (performance bias), incomplete outcome data (attrition bias), blinding of outcome assessment (detection bias), selective reporting (reporting bias), and other bias. 17 Each of the included studies was rated as having low, unclear, or high bias regarding the above items. The 2 reviewers resolved all disagreements through a discussion and consultation with a third investigator (W.F.).
Statistical Analysis
Data analyses were performed with Review Manager software (Version 5.3; Cochrane Collaboration). The risk ratio (RR) and its corresponding 95% CI were calculated for dichotomous data. For continuous variables assessed in the same way between studies, we calculated the mean difference (MD) and 95% CI, while for continuous variables assessed in different ways between studies, the standardized MD (SMD) and 95% CI were calculated. Heterogeneity was assessed by the I 2 statistic, and an I 2 value >50% and P < .05 were considered to indicate significant heterogeneity. 18 Random-effects or fixed-effects models were used depending on the heterogeneity of the study. A random-effects model was utilized for I 2 values >50%, whereas a fixed-effects model was applied for outcome data with no evidence of significant heterogeneity. Publication bias was assessed by funnel plot asymmetry, and the Egger regression test for funnel plot asymmetry was conducted for items with at least 10 studies and included in the meta-analysis.
Sensitivity analysis was performed by excluding each individual study from the overall analysis. Subgroup analysis was performed based on the follow-up time (≤24 vs >24 months), ALA technique (lateral extra-articular tenodesis [LEAT] vs ALL reconstruction [ALLR]), and ACLR technique (single bundle vs double bundle).
Results
Characteristics of Included Studies
The initial search of systematic reviews or meta-analyses generated a total of 28 records; 22 studies remained after removing duplicates. Then, the full-text articles were assessed for study inclusion, and 10 were excluded for not meeting eligibility criteria (Figure 1); of the 12 remaining, 3 studies were biomechanical or anatomy reviews, 1 study was a comment, and 1 study reported the data of only ACLRand so were removed, leaving 7. Of the 17 RCTs included in the 7 systematic reviews or meta-analyses, 10 RCTs met the inclusion criteria and were included in this study. In our subsequent search to identify individual RCTs in databases, we identified 821 published references. Overall, 26 full-text articles were reviewed in detail, and 22 were excluded, leaving 4 additional RCTs that met the inclusion criteria. Eventually, 14 unique RCTs involving 1850 participants were included in this review (Figure 1).

Literature search and screening process. ACL, anterior cruciate ligament; RCT, randomized controlled trial.
The included studies involved 941 patients treated by isolated ACLR and 909 patients who underwent ACLR+ALA (Table 1). All 14 studies were RCTs with an evidence level of 1. As determined by the Jadad scale, the score of included RCTs ranged from 2 to 6 points, with 10 studies § being of high quality (Jadad score ≥4) and 4 studies 1,19,53,59 being of poor quality (Jadad score <4).
Characteristics of Included Studies a

a ACLR, anterior cruciate ligament reconstruction; ALA, anterolateral augmentation; ALLR, anterolateral ligament reconstruction; DB, double bundle; LEAT, lateral extra-articular tenodesis; SB, single bundle.
Risk of Bias
The assessment of the risk of bias is summarized in Figure 2. Most of the RCTs described adequate randomization processes, allocation concealment, and blinding. The nature of the different interventions typically made the blinding of patients and surgical personnel effectively impossible. A blinded assessment of outcomes was used by some studies 6,13,14,19,44,56,59 to partially avoid this potential source of bias, while some studies 1,7,36,53,54,60 did not provide comprehensive blinding details, and one study 29 mentioned that the outcome assessment was not blinded. One study 6 lost more than 20% of patients during follow-up and was considered to have a high risk of attribution bias. There were 5 studies 6,36,44,53,56 that were rated as having a high risk of other sources of bias. The sources of bias included the following: the method of grouping introduced another element of variability or the included participants were either all female or all male. We judged the remaining studies to have an unclear risk of bias because of a lack of information.

Risk-of-bias results based on the Cochrane risk-of-bias tool. + = low risk of bias; − = high risk of bias; ? = unclear risk of bias.
Failure
A total of 12 studies ∥ (746 patients for isolated ACLR and 757 patients for ACLR+ALA) reported failure rates. The meta-analysis found that patients who underwent ACLR+ALA were less likely to have graft failure and/or revision surgery than patients who underwent isolated ACLR (RR, 0.30 [95% CI, 0.19-0.45]; P < .01) (Figure 3). No significant heterogeneity was found (I 2 = 0%; P = .89). The funnel plot and Egger test results revealed no evidence of publication bias for failure rates (P = .786) (Appendix Figure A1).

Forest plot showing failure rates for isolated anterior cruciate ligament reconstruction (ACLR) versus combined ACLR and anterolateral augmentation (ACLR+ALA). M-H, Mantel-Haenszel.
Anterior Laxity
There were 9 studies ¶ (355 patients for isolated ACLR and 363 patients for ACLR+ALA) that reported the SSD in postoperative anterior laxity. Considering that different measurement tools were used, the SMD of the SSD was determined. A random-effects model was utilized because of the significant heterogeneity. The outcomes revealed greater anterior knee laxity in patients who underwent ACLR compared with those who underwent ACLR+ALA (SMD, –0.55 [95% CI, –0.98 to –0.12]; P = .01) (Figure 4).

Forest plot showing postoperative knee laxity for isolated anterior cruciate ligament reconstruction (ACLR) versus combined ACLR and anterolateral augmentation (ACLR+ALA). Std., standardized; IV, inverse variance.
Pivot-Shift Test Findings
The pivot-shift test findings (graded as A, B, C, or D) were divided into good results (A or B) and poor results (C or D). Pivot-shift test findings were compared among 12 studies # (457 patients for isolated ACLR and 460 patients for ACLR+ALA). A higher proportion of good results was found in patients who underwent ACLR+ALA (RR, 1.06 [95% CI, 1.02-1.10]; P = .0008). No significant heterogeneity was found (I 2 = 14%; P = .31) (Figure 5). The funnel plot revealed that studies were scattered near the effect estimates, and no evidence of publication bias was detected for the pivot-shift test findings (P = .413; Egger test) (Appendix Figure A2).
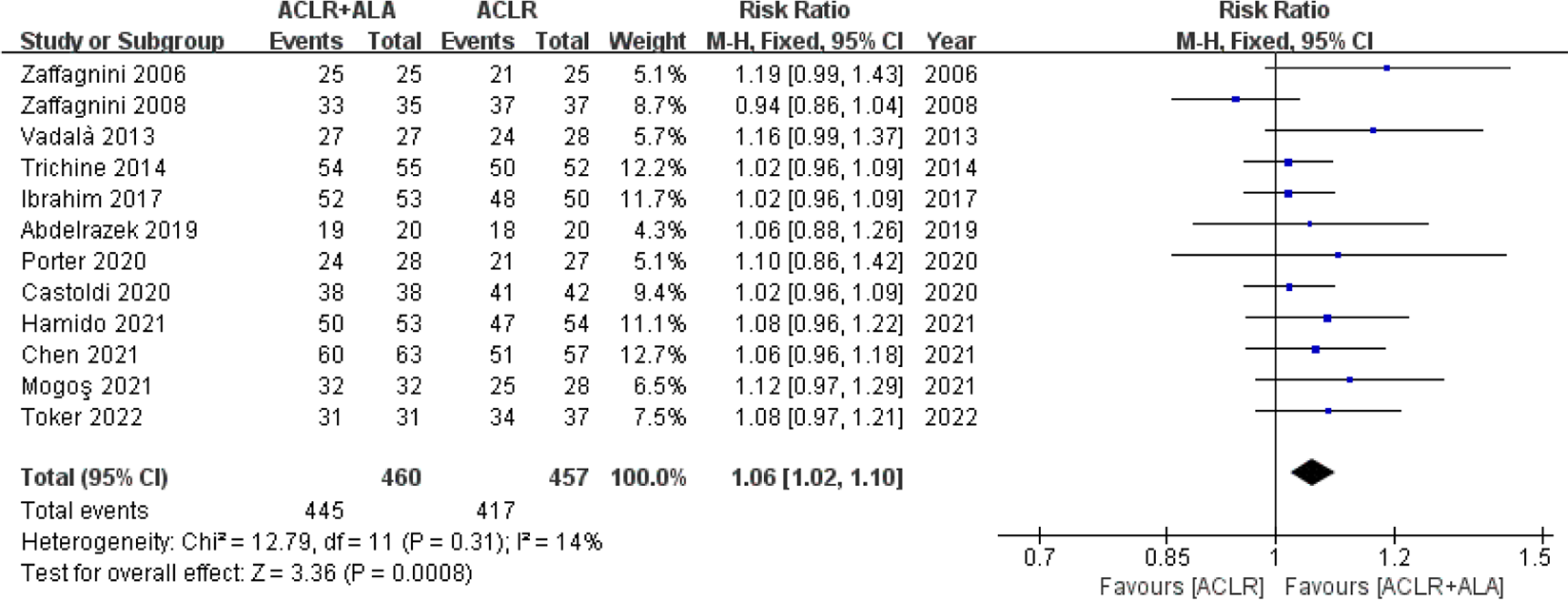
Forest plot showing pivot-shift test findings for isolated anterior cruciate ligament reconstruction (ACLR) versus combined ACLR and anterolateral augmentation (ACLR+ALA). M-H, Mantel-Haenszel.
Lachman Test Results
The outcomes of the Lachman test were divided into good results (ie, normal and nearly normal) and poor results (ie, abnormal and severely abnormal). Overall, 8 studies 1,6,7,14,19,53,56,60 (308 patients for isolated ACLR and 304 patients for ACLR+ALA) reported postoperative Lachman scores. No significant heterogeneity was found (I 2 = 0%; P = .93). A greater proportion of good results according to the Lachman test was found in patients who underwent ACLR+ALA (RR, 1.03 [95% CI, 1.00-1.07]; P = .04) (Figure 6).
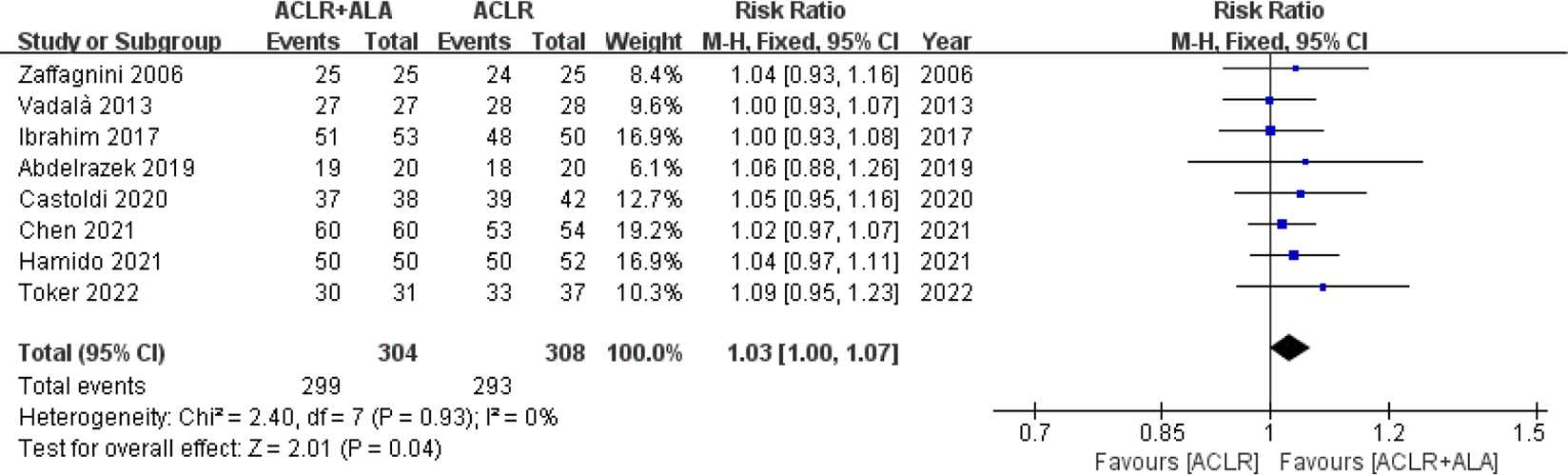
Forest plot showing Lachman test results for isolated anterior cruciate ligament reconstruction (ACLR) versus combined ACLR and anterolateral augmentation (ACLR+ALA). M-H, Mantel-Haenszel.
IKDC Scores
A total of 10 studies ** (414 patients for isolated ACLR and 430 patients for ACLR+ALA) provided postoperative IKDC scores that could be used in the meta-analysis, and no heterogeneity was found (I 2 = 0%; P = .68) (Figure 7). IKDC scores were compared among patients in each group in the form of ordered categorical data. The proportion of patients with IKDC grades A and B did not differ between the isolated ACLR and ACLR+ALA groups (RR, 1.02 [95% CI, 0.98-1.05]; P = .32).

Forest plot showing International Knee Documentation Committee scores for isolated anterior cruciate ligament reconstruction (ACLR) versus combined ACLR and anterolateral augmentation (ACLR+ALA). M-H, Mantel-Haenszel.
Tegner Scores
There were 6 studies 14,19,44,56,59,60 (280 patients for isolated ACLR and 292 patients for ACLR+ALA) that reported postoperative Tegner scores, and significant heterogeneity was found (I 2 = 65%; P = .01) (Figure 8). Tegner scores reported as means and standard deviations were used in the meta-analysis. No significant differences were found between the 2 procedures in terms of postoperative Tegner scores (MD, 0.24 [95% CI, –0.16 to 0.65]; P = .24).

Forest plot showing Tegner scores for isolated anterior cruciate ligament reconstruction (ACLR) versus combined ACLR and anterolateral augmentation (ACLR+ALA). IV, inverse variance.
KOOS Subscores
Only 3 studies 13,36,44 reported KOOS subscores. As the KOOS Sport/Recreation subscore was the most reported, the meta-analysis was conducted in terms of this subscale (413 patients for isolated ACLR and 421 patients for ACLR+ALA). Significant heterogeneity was detected (I 2 = 95%; P < .01); hence, a random-effects model was utilized. No significant difference was found between the ACLR and ACLR+ALA groups (MD, 3.89 [95% CI, –1.20 to 8.98]; P = .13) (Figure 9).

Forest plot showing Knee injury and Osteoarthritis Outcome Score subscores for isolated anterior cruciate ligament reconstruction (ACLR) versus combined ACLR and anterolateral augmentation (ACLR+ALA). IV, inverse variance.
Return to Sport
Overall, 7 studies 6,7,13,29,54,59,60 (536 patients for isolated ACLR and 539 patients for ACLR+ALA) reported RTS rates (Figure 10). No significant heterogeneity was found between studies (I 2 = 25%; P = .24). No significant differences were found between the 2 procedures in terms of RTS rates (RR, 0.98 [95% CI, 0.94-1.02]; P = .32).
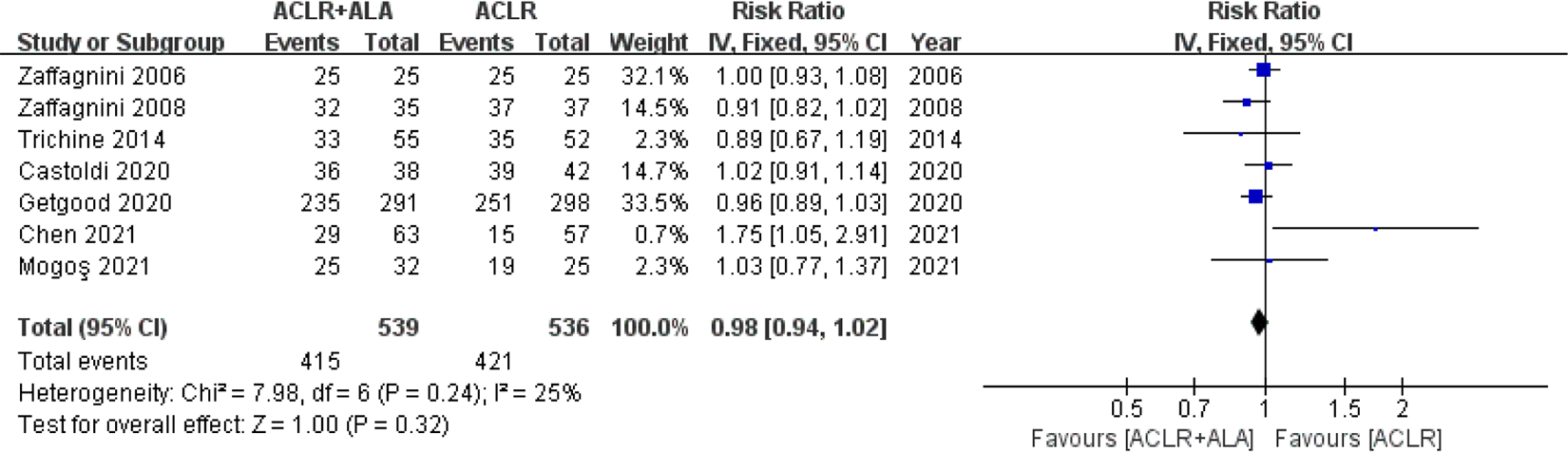
Forest plot showing return-to-sport rates for isolated anterior cruciate ligament reconstruction (ACLR) versus combined ACLR and anterolateral augmentation (ACLR+ALA). IV, inverse variance.
Sensitivity and Subgroup Analyses
Sensitivity analysis demonstrated that no single study had any overall influence. Subgroup analysis based on follow-up time (≤24 vs >24 months), ALA technique (ALLR vs LEAT), and ACLR technique (single bundle vs double bundle) was performed using the RR for the IKDC score, RTS rate, pivot-shift test, and Lachman test as well as the MD for the Tegner score and the SMD for SSD in anterior laxity. Subgroup analysis was performed only if the subgroup included at least 2 studies.
We did not identify any subgroup effects according to follow-up time (Table 2). However, subgroup analysis according to ALA technique showed that the use of ALLR significantly improved SSD in postoperative anterior laxity (SMD, –1.10 [95% CI, –1.74 to –0.46]; P < .01) while the use of LEAT did not have the same effect (SMD, –0.11 [95% CI, –0.31 to 0.09]; P = .29). However, an improvement in the Tegner score was seen with LEAT (MD, 0.56 [95% CI, –0.47 to 1.59]; P = .01), while no such effect was observed after ALLR (MD, 0.03 [95% CI, –0.22 to 0.29]; P = .79) (Table 3). Subgroup analysis of ACLR technique indicated that pivot-shift test findings and SSD in anterior laxity were significantly improved with double-bundle ACLR (pivot shift: RR, 1.02 [95% CI, 0.95 to 1.09]; P = .53) (anterior laxity: SMD, –0.11 [95% CI, –0.37 to 0.15]; P = .40) compared with the single-bundle approach (pivot shift: RR, 1.07 [95% CI, 1.03 to 1.12]; P < .01) (anterior laxity: SMD, –0.76 [95% CI, –1.35 to –0.18]; P = .01) (Table 4).
Subgroup Analysis Based on Follow-up Time a

a Boldface P values indicate statistical significance (P < .05). IKDC, International Knee Documentation Committee; MD, mean difference; RR, risk ratio; RTS, return to sport; SMD, standardized mean difference; SSD, side-to-side difference.
Subgroup Analysis Based on ALA Technique a

a Boldface P values indicate statistical significance (P < .05). ALA, anterolateral augmentation; ALLR, anterolateral ligament reconstruction; IKDC, International Knee Documentation Committee; LEAT, lateral extra-articular tenodesis; MD, mean difference; RR, risk ratio; RTS, return to sport; SMD, standardized mean difference; SSD, side-to-side difference.
Subgroup Analysis Based on ACLR Technique a

a Boldface P values indicate statistical significance (P < .05). ACLR, anterior cruciate ligament reconstruction; IKDC, International Knee Documentation Committee; MD, mean difference; RR, risk ratio; RTS, return to sport; SMD, standardized mean difference; SSD, side-to-side difference.
Discussion
This meta-analysis was conducted to obtain a precisely focused comparison of clinical results, including graft failure, patient-reported outcomes, stability, postoperative knee laxity, and RTS, between isolated ACLR and ACLR+ALA. The most important finding of the present study was that knee stability based on the pivot-shift and Lachman tests and knee laxity based on the SSD were worse in the isolated ACLR group and that the graft rupture rate was lower in the ACLR+ALA group (pivot shift: P = .0008; Lachman: P = .04; SSD in anterior laxity: P = .01; graft failure: P < .01), although the patient-reported outcomes based on the IKDC, Tegner, and KOOS scores and the RTS rate were not significantly different between the ACLR and ACLR+ALA groups (IKDC: P = .32; Tegner: P = .24; KOOS: P = .13; RTS: P = .32).
Based on subgroup analysis, a significant improvement in the SSD in anterior laxity was seen with ALLR versus LEAT (ALLR: SMD, –1.10 [95% CI, –1.74 to –0.46]; P < .01) (LEAT: SMD, –0.11 [95% CI, –0.31 to 0.09]; P = .29). However, ALLR was also attributed to worse Tegner scores (ALLR: MD, 0.03 [95% CI, –0.22 to 0.29]; P = .79) (LEAT: MD, 0.56 [95% CI, –0.47 to 1.59]; P = .01). Double-bundle ACLR showed advantages in knee stability (pivot shift: RR, 1.02 [95% CI, 0.95 to 1.09]; P = .53) (anterior laxity: SMD, –0.11 [95% CI, –0.37 to 0.15]; P = .40) compared with single-bundle ACLR (pivot shift: RR, 1.07 [95% CI, 1.03 to 1.12]; P < .01) (anterior laxity: SMD, –0.76 [95% CI, –1.35 to –0.18]; P = .01).
The clinical assessment of graft laxity included measurements with a KT-1000/KT-2000/Rolimeter arthrometer, the pivot-shift test, and the Lachman test. Higher postoperative knee laxity is correlated with a higher risk of meniscal tears, cartilage lesions, and graft failure, which would ultimately result in progressively irreversible osteoarthritis and worse subjective long-term outcomes. 39,50 In this study, a significant decrease in the SSD was found in the ACLR+ALA group compared to the isolated ACLR group, contrary to the study of Lee et al 24 in which no significant differences in anterior laxity were found. The lack of a significant difference in graft laxity between the 2 groups may have been caused by patient selection bias for revision ACLR. A recent cadaveric study showed that the ALL contributes to the restraint of anterior tibial translation in ACL-injured knees, indicating that a small increase in anterior tibial translation may be clinically relevant. 12 Improvements in the satisfaction and knee function of patients have been shown to have direct associations with knee rotational stability; therefore, rotational stability has received increased attention after ACLR. Studies have revealed better pivot-shift test findings in patients who underwent ACLR+ALA, 56,60 which was in agreement with our study. Previous researchers have also revealed that the pivot-shift test is multifactorial and may be influenced by performance methodology, applied torque, and variability between different examiners. 54 Moreover, a multicenter cohort study showed that a greater preoperative pivot shift under anesthesia and knee hyperextension were risk factors for a residual pivot shift after ACLR. 15 As a residual pivot shift is associated with clinical outcomes, satisfaction, functional scores, and activity levels as well as cartilage lesions, meniscal tears, and osteoarthritis, 3,49 it should be considered of increased importance. This study also found that the Lachman test results favored the ACLR+ALA group, indicating that ACLR+ALA also affected anteroposterior stability. This is not difficult to understand because the ALL acts as a secondary stabilization structure contributing to better Lachman test results.
Graft failure is an unacceptable and feared complication for patients, especially young athletes who expect to return to competition. In this study, patients who underwent isolated intra-articular ACLR had a higher risk of graft failure than those who underwent combined ACLR and extra-articular ALA. A recent study found that ACLR+ALA was related to lower rates of graft failure than isolated ACLR. 42 Additionally, in a recent clinical study focusing on a young population that participated in sports involving pivoting, graft failure rates were higher in both groups than in our meta-analysis, with a rate of 11% in the isolated ACLR group, which was much higher than the rate in the ACLR+ALA group. 46 The advantages of ALA have been clearly demonstrated for active young patients who have a high risk of graft ruptures. However, our graft failure results were inconsistent with a previous study that indicated no difference between the 2 groups. 40 Undoubtedly, research conducted during recent years has added some weight to this evidence and has changed the overall findings. Although the graft rerupture rates were not high in the 2 groups, the observed difference in this study should not be underestimated, and clinicians should weigh and consider this new finding, especially for patients who participate in sports involving pivoting.
Overconstraint of the knee is a major concern regarding ACLR+ALA, which could cause some problems, even the development of osteoarthritis in the knee, in the long run. Only 2 of the included studies assessed knee osteoarthritis conditions based on radiological results. Zaffagnini et al 60 evaluated degenerative joint disease on radiographs, and no difference was found between ACLR and that combined with LEAT. However, Castoldi et al 6 evaluated tibiofemoral osteoarthritis on weightbearing radiographs and found that the addition of LEAT was associated with a significantly increased risk of lateral tibiofemoral osteoarthritis. It should be noted that lateral meniscal lesions, a proven risk factor of osteoarthritis, were significantly more frequent in the LEAT group. Based on the postoperative KOOS Sport/Recreation subscores in 3 studies, 13,36,44 no statistical difference was found between isolated ACLR and ACLR+ALA. In a recent biomechanical study comparing the impact of different anterolateral procedures on knee kinematics, additional LEAT was proven to overconstrain internal rotation, leading to nonphysiological kinematics, while ALLR did not have such a risk. Unfortunately, with only 1 study 44 reporting KOOS subscores after ALLR, subgroup analysis in the present study by ALA technique was not available.
Strengths and Limitations
The strengths of our meta-analysis are the pre-established protocol for identifying clinical outcomes after isolated ACLR and ACLR+ALA, including pivot-shift test findings, Lachman test results, instrumented laxity, IKDC scores, Tegner scores, KOOS subscores, and RTS rates. Although the patient-reported outcomes for the IKDC score, Tegner score, and KOOS were not significantly different between the isolated ACLR and ACLR+ALA groups, our meta-analysis found that knee stability based on the pivot-shift test, Lachman test, and SSD in anterior laxity was better in patients who underwent ACLR+ALA. However, it is still unclear whether this additional procedure is worth performing in each patient. Moreover, the surgical technique, optimal graft type, isometric location of ALA and individual reconstruction, most appropriate knee flexion angle during ALL graft fixation, and optimal fixation tension for ALA remain to be further determined. Because of the small sample sizes and short-term duration of follow-up in some of the included studies, these conclusions should be further validated by more high-quality RCTs to determine the characteristics of patients who would be suitable and benefit from ACLR+ALA as well as the optimal surgical techniques for ALA.
The present study has several limitations. First of all, inconsistent findings and sparse data made it difficult to pool and analyze all data across the included studies and thus weakened the strength of our results. For example, some studies reported the grade classification of the Lysholm score, whereas other studies reported MDs of the results. Considerable variability in techniques regarding the assessment of isolated ACLR and ACLR+ALA in the included studies was another concern, as heterogeneity was increased by this variability. However, most results revealed low heterogeneity, allowing the corresponding conclusions to be derived. Moreover, subgroup analyses were also performed and revealed the clinical effects of different follow-up times and types of ALA and ACLR.
Furthermore, variability was observed in the included studies with regard to additional extra-articular procedures, as abundant techniques are available for ALA. As further study of the anatomy and biomechanical function of the ALL increases, more anatomic extra-articular ALA techniques for specific structures may be developed, which may improve clinical outcomes in the knee. 23,34 Therefore, we divided the ALA procedure into 2 categories and then carried out subgroup analysis based on the use of LEAT and ALLR, which showed that better results on the SSD in anterior laxity was reported in the ALLR group.
Postoperative radiological outcomes are another aspect of the clinical evaluation of ACLR. Unfortunately, data on validated patient-oriented imaging outcomes were unavailable for comparison.
Finally, the follow-up of some included studies was relatively short term, and therefore, it was not possible to evaluate the overall long-term clinical effects of the 2 procedures. However, our subgroup with >24 months of follow-up showed better pivot-shift test findings in the ACLR+ALA group. Known aspects of ACLR techniques, such as graft choice, fixation method, osseous tunnel location, and rehabilitation program, possibly influence final outcomes and should be considered before performing combined extra-articular surgery. 27,60 Similar patient-reported outcomes (IKDC and Tegner scores) were reported in the 2 treatment groups, suggesting that additional ALA did not influence the final functional outcomes.
Conclusion
The addition of ALA can be considered as a reinforcement of ACLR to improve anteroposterior and anterolateral rotational stability of the knee. Both isolated ACLR and ACLR+ALA provided improved knee function at short-term to midterm follow-up.
Footnotes
Notes
Final revision submitted September 28, 2022; accepted October 21, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: Support for this study was received from the National Natural Science Foundation of China (grants 81972123 and 82172508) and the 135 Project for Disciplines of Excellence of West China Hospital, Sichuan University (grants ZYJC21030 and ZYGD21005). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.
Search Strategy of Part 1 of the Study

| Database | Search Strategy |
|---|---|
| PubMed |
“ACL” [MeSH Terms] OR “ACL” [All Fields] OR “anterior cruciate ligament” [MeSH Terms] OR “anterior cruciate ligament” [All Fields] “extraarticular” [MeSH Terms] OR “extraarticular” [All Fields] OR “anterolateral ligament” [MeSH Terms] OR “anterolateral ligament” [All Fields] systematic[sb] OR Meta Analysis[ptyp] #1 and #2 and #3 |
| Embase |
‘ACL’/exp OR ‘ACL’ ‘anterior cruciate ligament’/exp OR ‘anterior cruciate ligament’ ‘extraarticular’/exp OR ‘extraarticular’ ‘anterolateral ligament’/exp OR ‘anterolateral ligament’ [cochrane review]/lim OR [systematic review]/lim OR [meta analysis]/lim #1 or #2 #3 or #4 #5 and #6 and #7 |
| Cochrane Library |
ACL: ti, ab, kw (Word variations have been searched) anterior cruciate ligament: ti, ab, kw (Word variations have been searched) extraarticular: ti, ab, kw (Word variations have been searched) anterolateral ligament: ti, ab, kw (Word variations have been searched) #1 or #2 #3 or #4 #5 and #6 (restricted as Cochrane reviews or other reviews) |