
Abstract
Background:
Open and fluoroscopic techniques have been described for localization of the femoral attachment site in medial patellofemoral ligament (MPFL) reconstruction. No study to date has evaluated if one technique is superior to another in terms of complications.
Purpose:
To review the literature comparing clinical outcomes of MPFL reconstruction using the fluoroscopic versus open technique to localize the site of femoral graft placement.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A systematic literature review was performed via PubMed, Embase, and CINAHL to identify articles published between the inception of these databases and March 1, 2022, in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. This search yielded 4183 publications for initial review. Studies with at least a 2-year follow-up and complete reporting of patient-reported outcomes, range of motion, recurrent instability, and/or complications (ie, stiffness, infection, persistent pain) were included. We excluded studies of patients with collagen disorders; revision surgeries; surgeries with concomitant procedures; synthetic MPFL reconstruction; MPFL repairs; combined open and radiographic technique; and case series that included <10 patients. A proportional meta-analysis was performed by calculating the pooled estimate of incidence with 95% CIs using a fixed-effects model with double arcsine transformation (Freeman-Tukey) for each type of surgical technique (fluoroscopic or open).
Results:
A total of 29 studies met our inclusion criteria, of which 15 studies (566 patients) used the open technique and 14 studies (620 patients) used fluoroscopy. There were no significant differences between the open and fluoroscopic techniques in the incidence of postoperative apprehension (P = .4826), postoperative subjective instability (P = .1095), postoperative objective instability (P = .5583), reoperations (P = .7981), recurrent dislocation (P = .6690), or arthrofibrosis (P = .8118).
Conclusion:
Both open and radiographic localization of the femoral graft position in MPFL reconstruction offer similar outcomes and rates of complications.
Medial patellofemoral ligament (MPFL) reconstruction has gained popularity since the 1990s, and much evidence exists showing a low reoperation rate, a high rate of return to sport, and reduction of apprehension and instability recurrence. 9,37 Despite overall success with MPFL reconstruction, a complication rate of up to 26% has been reported. 29,40 Complications are in part associated with difficulty in consistently finding the appropriate femoral graft insertion point. Incorrect graft placement has been implicated in failure to correct patellar instability, 4,7,29,47,48 and an anteriorly placed graft has been identified as a risk factor for postoperative stiffness due to nonisometry. 29 Graft placement on the femoral side has been shown to be the most influential technical factor in creating an isometric graft. 46 The proximal-distal direction has the greatest sensitivity to changes in graft length, 43 with an anterior position causing the greatest graft length change at deeper flexion angles. 35 Thus, it has been suggested to avoid a graft position that is too far anterior and proximal. 17
The femoral attachment of the MPFL is located transversely in a bony groove between the medial epicondyle and the adductor tubercle. 26 Nomura et al found that the MPFL courses from the medial patellar margin to the posteromedial capsule, with deep fibers anchored on the femur just distal to the adductor tubercle. This is known as the “Nomura point” and is located 9.5 mm proximal and 5.0 mm posterior to the center of the medial epicondyle. 26
The femoral insertion of the MPFL may be located intraoperatively utilizing either open or radiographic techniques. Schöttle et al 38 described the widely used radiographic landmarks for anatomic femoral attachment. The Schöttle point can be localized on a true lateral radiograph 1 mm anterior to the tangent of the posterior femoral cortex, 2.5 mm distal to a perpendicular line through the proximal-most aspect of the femoral condyle, and proximal to a perpendicular line traced through the most posterior aspect of the Blumensaat line.
There are several challenges with radiographic and open approaches. It can be difficult to obtain a true lateral radiograph of the knee while instrumenting (utilizing procedural tools, inserting grafts or implants to perform the MPFL reconstruction procedure), and recently, the accuracy of the Schöttle point to the native MPFL femoral attachment has been challenged. 36,53 An open approach may theoretically provide visual or palpable confirmation of the location of the MPFL origin. However, an open approach generally requires a larger dissection, and appropriate landmarks may still be difficult to see or palpate. To our knowledge, a clinical comparison of outcomes between open and fluoroscopic techniques has not been performed.
The purpose of this systematic review was to compare clinical outcomes, particularly recurrent instability and stiffness, using a fluoroscopic versus open technique to localize the site of femoral graft attachment. We hypothesized that there would be no difference in clinical outcomes and complication rates for fluoroscopic versus open localization techniques.
Methods
Literature Search and Study Selection
A systematic review of the literature focusing on fluoroscopic and open techniques for localizing the site of femoral fixation in patients undergoing MPFL reconstruction was conducted in accordance with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 24 A search was performed using PubMed, Embase, and CINAHL to identify articles published between the inception of these databases and March 1, 2022. The search terms included (“medial patellofemoral” OR “MPFL”) AND “reconstruction” OR (“patellar instability” AND “surgery”).
Inclusion criteria were a minimum 2-year follow-up as well as complete reporting of patient-reported outcomes, range of motion, stability, success/failure, and/or complications (ie, recurrent instability, stiffness, infection, persistent pain). We excluded studies of patients with Marfan, Ehlers-Danlos, or other collagen disorders; revision surgeries; surgeries with concomitant procedures; synthetic MPFL reconstruction; MPFL repairs; no description of surgical technique; combined open and radiographic technique; data not stratified by type of treatment; no femoral fixation; and <2 years of follow-up. We also excluded case series (<10 patients), review articles, abstracts, and articles not published in the English language. Two authors (K.H., C.C.) independently screened the results of the literature search to identify articles that met the inclusion criteria, which were then reviewed by the senior authors to resolve any disagreement.
Level of Evidence and Quality Assessment
We used the Oxford Centre for Evidence-Based Medicine criteria 27 to determine the level of evidence for each study. The same two authors independently evaluated the methodological quality and risk of bias for each study with the Downs and Black study quality assessment tool. 6 The maximum Downs and Black score, indicative of good methodological quality/low risk for bias, is 9 points for case series, 15 points for observational studies, and 32 points for randomized controlled trials.
Data Extraction
Two reviewers (K.H., C.C.) independently extracted the following data from each article into a standardized database: study design, sample size, sex, age at surgery, length of follow-up, surgical technique (fluoroscopic or open), graft fixation method, graft origin, type of graft (autograft or allograft), and concomitant procedures. Postoperative data included apprehension, subjective instability, objective instability, recurrent dislocation, arthrofibrosis, and reoperation. Subjective instability was defined as a patient-perceived instability of the patellofemoral joint without documented dislocation. Objective instability was defined as patellar hypermobility on surgeon-performed postoperative physical examination.
Statistical Analysis
Study characteristics were tabulated and described. Since the majority of the studies were only single-arm studies, a traditional comparative meta-analysis could not be performed. 5 Instead, a proportional meta-analysis was performed by calculating the pooled estimate of incidence with 95% CIs using a fixed-effects model with double arcsine transformation (Freeman-Tukey) for each type of surgical technique (fluoroscopic or open). To include studies with zero incidences, a continuity correction was performed by adding 0.5 to the numerator and denominator of incidence. 34 Forest plots were made, and the pooled estimate of incidence was compared between surgical techniques by seeing if their 95% CIs overlapped. Additionally, a P value was calculated using methods described in the Cochrane handbook, 16 which calculates the standard deviation from the confidence interval and uses a t test to compare means. Of note, this is an estimated P value since it was calculated using transformed values. Heterogeneity statistics (I 2) were calculated but are irrelevant to compare in proportional meta-analyses, as all studies were single-arm studies. 23 A P value <.05 was considered statistically significant, and all analyses were performed using JBI System for the Unified Management, Assessment and Review of Information. 31
Results
The literature search identified 4183 unique articles. Of these, 240 articles were screened for eligibility and 29 met inclusion criteria (Figure 1).
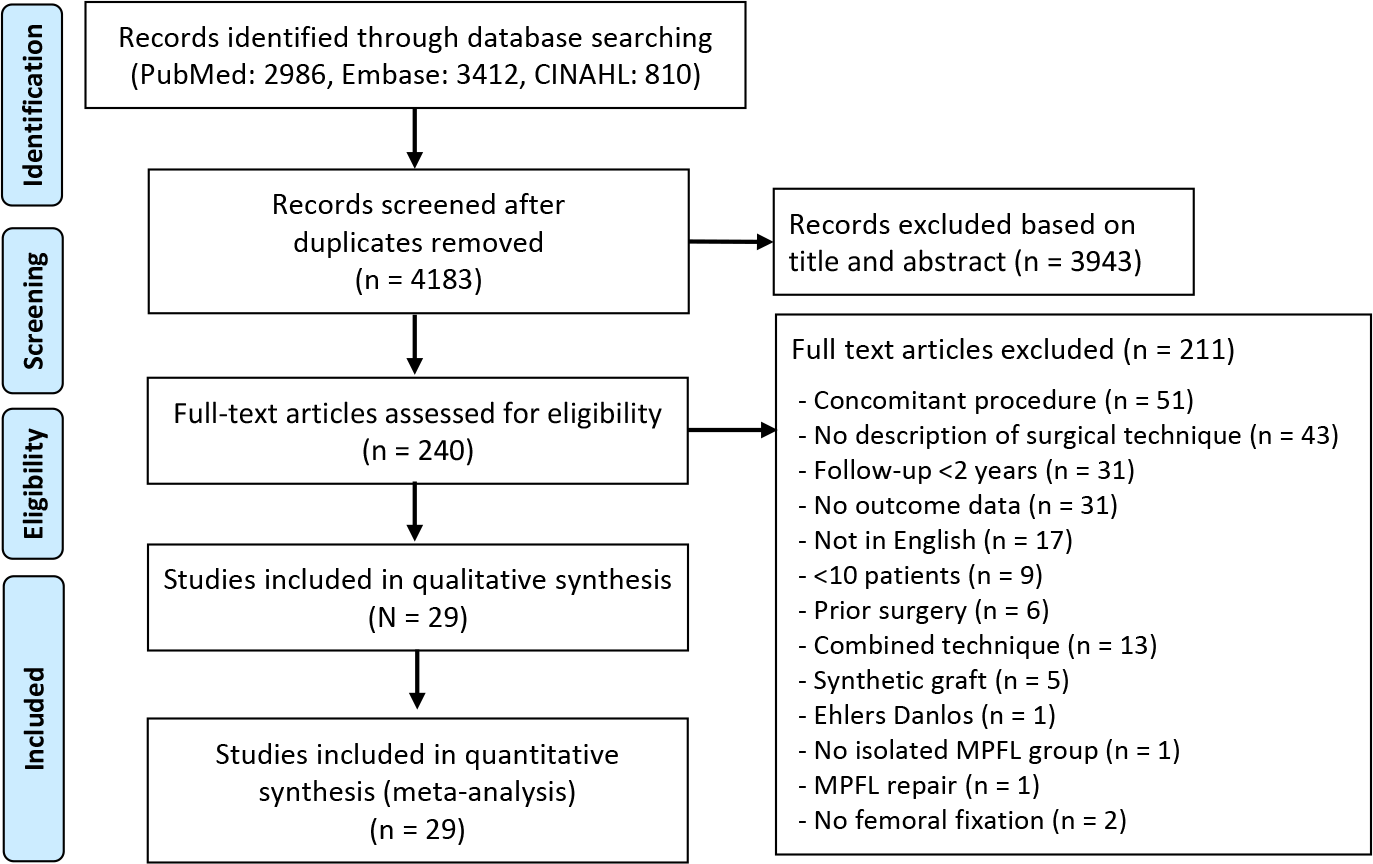
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart for study inclusion. MPFL, medial patellofemoral ligament.
Study Characteristics
The characteristics of the included studies are shown in Table 1. Fifteen studies § (566 patients) used the open technique and 14 studies ∥ (620 patients) used fluoroscopy. There were 23 studies ¶ with level 4 evidence, 3 studies 18,32,41 with level 3 evidence, 2 studies 2,52 with level 2 evidence, and 1 study 8 with level 1 evidence. Overall, the study quality was good, and most studies had a low risk for bias based on the total Downs and Black scores (Table 1). The minimum score indicative of good methodological quality/low risk of bias was 6 and higher for case series, 11 and higher for observational/cohorts, and 20 and higher for RCTs.
Study Characteristics Stratified by Surgical Technique a

a F, female; LOE, level of evidence; M, male; MPFL, medial patellofemoral ligament; NR, not reported; PF, patellofemoral; RCT, randomized controlled trial.
b The maximum possible Downs and Black score, indicative of good methodological quality/low risk for bias, is 9 points for case series, 15 points for observational studies, and 32 points for randomized controlled trials.
Suture anchor or transosseous suture # were most commonly used for graft fixation to the patella, and an interference screw was most commonly used for femoral fixation. ** Most studies used semitendinosus or gracilis hamstring autograft for MPFL reconstruction (Table 2).
Surgical Details Stratified by Surgical Technique a

a Quad, quadriceps tendon; ST, semitendinosus; TA, tibialis anterior.
Results of Meta-analysis
The incidence rates of postoperative apprehension after fluoroscopic (3.1% [95% CI, 0.0%-9.1%]) and open (5.4% [95% CI, 2.6%-8.8%]) techniques were not significantly different (P = .4826) (Figure 2). In addition, there was no significant difference in the incidence of postoperative subjective instability for fluoroscopic (3.1% [95% CI, 1.3%-5.6%]) versus open (6.1% [95% CI, 3.3%-9.5%]) techniques (P = .1095) (Figure 3). The incidence of reoperation for the fluoroscopic (3.2% [95% CI, 1.3%-5.7%]) compared with the open (3.6% [95% CI, 1.8%-6.0%]) technique was not significantly different (P = .7981) (Figure 4).
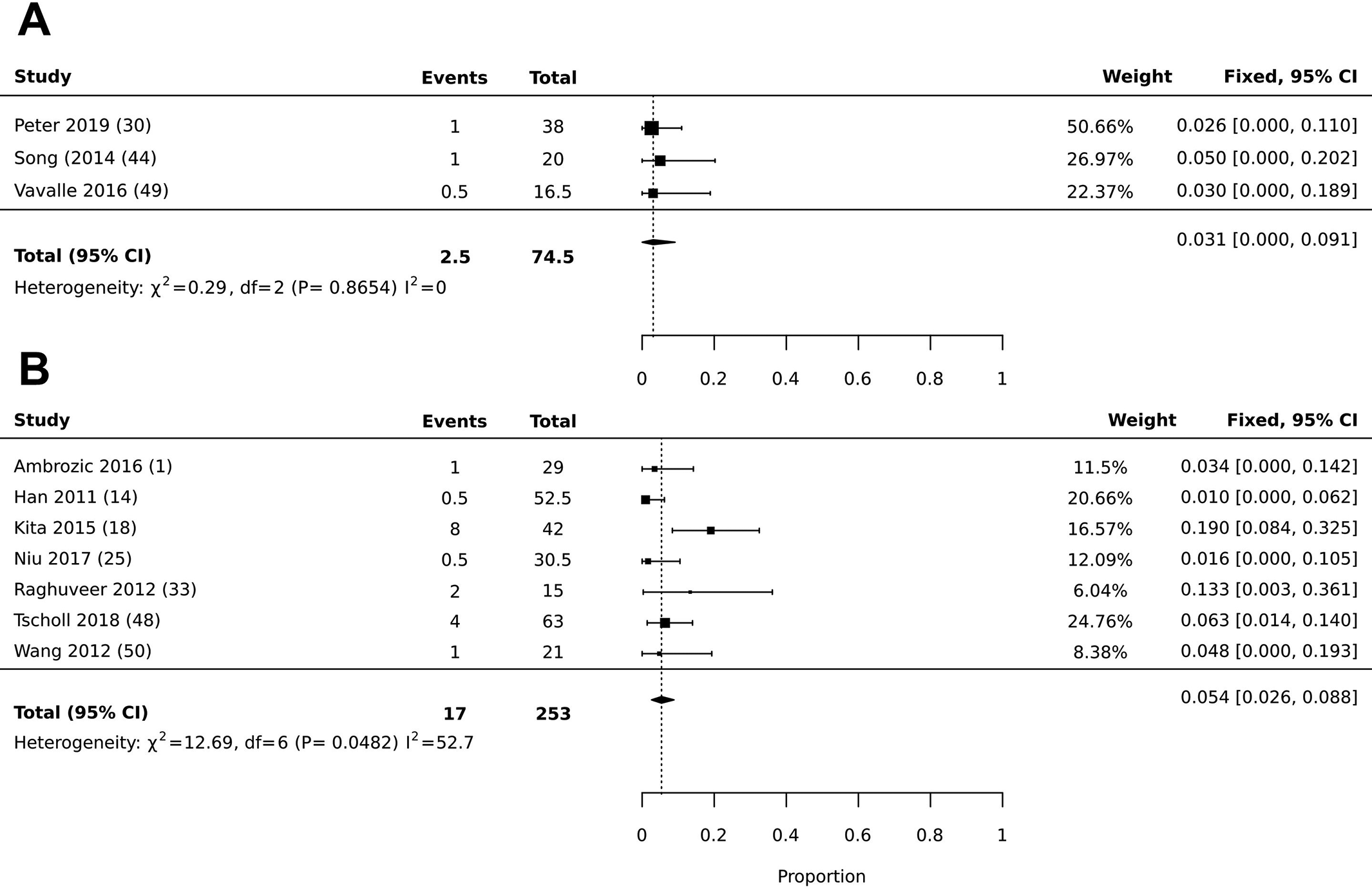
Forest plot illustrating the prevalence of postoperative apprehension for (A) intraoperative fluoroscopy versus (B) open surgery.

Forest plot illustrating the prevalence of postoperative subjective instability for (A) intraoperative fluoroscopy versus (B) open surgery.
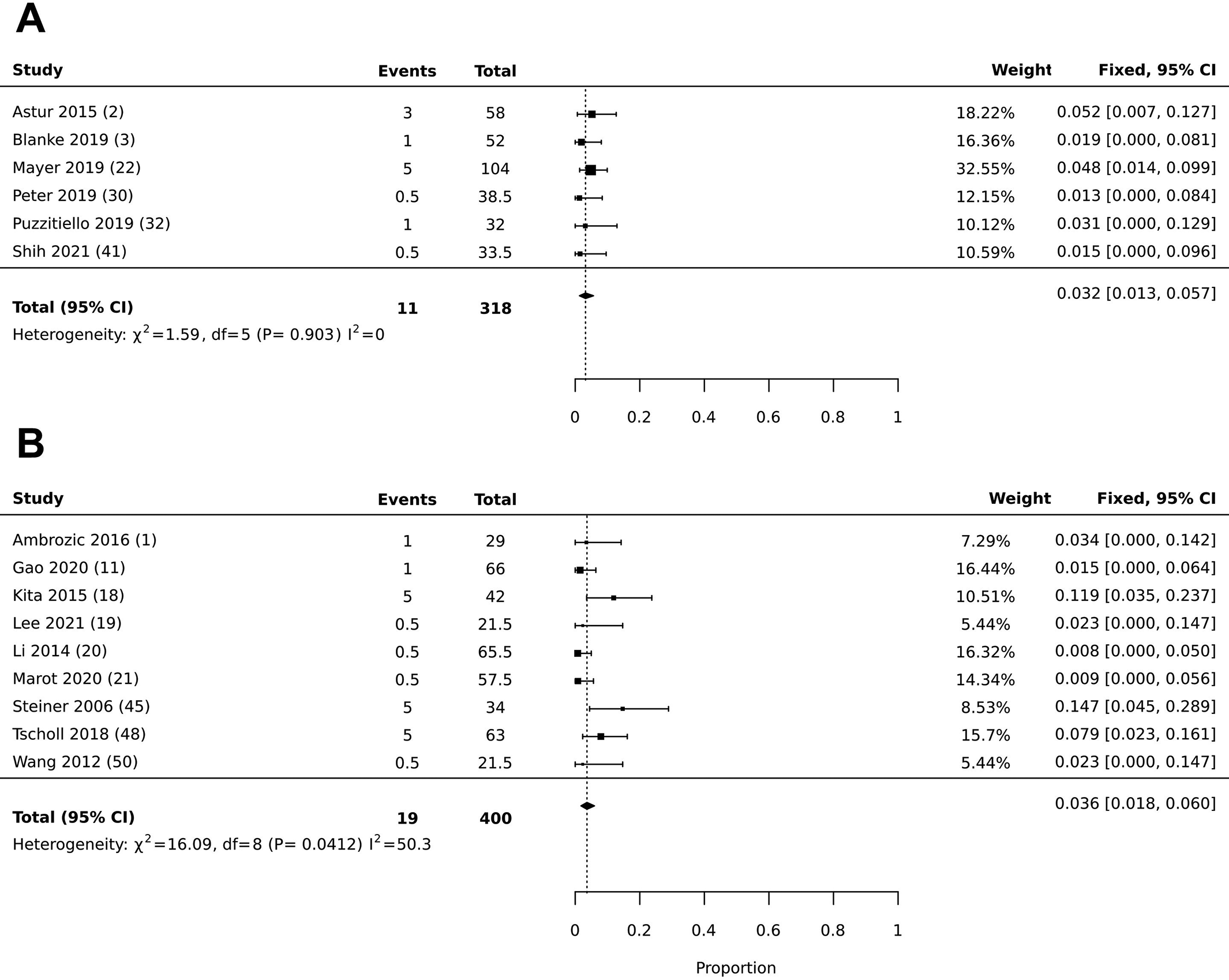
Forest plot illustrating the prevalence of reoperation for (A) intraoperative fluoroscopy versus (B) open surgery.
There was no significant difference in the incidence of postoperative objective instability after the fluoroscopic (1.4% [95% CI, 0.1%-3.7%]) versus the open (2.5% [95% CI, 0.1%-7.1%]) technique (P = .5583) (Figure 5). The incidence rates of recurrent dislocation after fluoroscopic (1.4% [95% CI, 0.4%-2.8%]) and open (1.8% [95% CI, 0.6%-3.4%]) techniques were not significantly different (P = .6690) (Figure 6). Last, there was no significant difference in the incidence of arthrofibrosis for the fluoroscopic (1.7% [95% CI, 0.1%-4.6%]) compared with the open (1.3% [95% CI, 0.0%-4.7%]) technique (P = .8118) (Figure 7).

Forest plot illustrating the prevalence of postoperative objective instability for (A) intraoperative fluoroscopy versus (B) open surgery. F-T.

Forest plot illustrating the prevalence of recurrent dislocation for (A) intraoperative fluoroscopy versus (B) open surgery.

Forest plot illustrating the prevalence of arthrofibrosis for (A) intraoperative fluoroscopy versus (B) open surgery.
Discussion
Our proportional meta-analysis comparing the pooled incidence of complications revealed no significant differences in postoperative outcomes when comparing open and radiographic techniques to localize femoral tunnel position during MPFL reconstruction. The incidence rates of postoperative apprehension (fluoroscopic, 3.1%; open, 5.4%), subjective instability (fluoroscopic, 3.1%; open, 6.1%), reoperation (fluoroscopic, 3.2%; open, 3.6%), objective instability (fluoroscopic, 1.4%; open, 2.5%), recurrent dislocation (fluoroscopic, 1.4%; open 1.8%), and arthrofibrosis (fluoroscopic, 1.7%; open, 1.3%) were not statistically different. Reoperations were reported for 11 of 317 patients in the fluoroscopy group and 19 of 400 in the open technique group. Reoperations were required for removal of symptomatic hardware, arthrofibrosis, redislocation, graft failure, patellar fracture, postoperative hematoma, and suture granuloma. ††
Complications after MPFL reconstruction may be due to several different anatomical or surgical factors. One potential source of complications may be poor femoral tunnel placement. 4,29,40 Some studies have evaluated how accurate surgeons are at determining the location of femoral fixation. 48,54 Additionally, the accuracy of the radiographic technique utilizing the Schöttle point has recently been called into question. Sanchis-Alfonso et al 35 showed that the native attachment of the MPFL may be up to 4.1 mm from the radiographic point as identified. Furthermore, the margin of error for localizing the Schöttle point on a lateral radiograph is quite small. Five degrees of rotational error corresponds to malpositions of 7.5, 9.2, and 8.1 mm in the anteroposterior, posteroanterior, and cephalad orientations, respectively. 54 By comparison, the open technique has demonstrated a broad range of accuracy, from 65% to 92.3%. 15,39 Despite these findings, our data suggest that the outcomes and complication profile are similar for both techniques.
Limitations
Our study has several limitations inherent to being a proportional meta-analysis, including the lack of comparative arms within studies, publication bias, small study effect, and the quality and heterogeneity of the studies included. Most of the studies included had a low level of evidence. Variabilities in patient number, sex ratio, age at time of surgery, and length of follow-up can also be seen. Another limitation in this study is the variation in technique and implant choice. However, we did find that most studies used suture anchor or transosseous suture for patellar fixation, and more than two-thirds used interference screw femoral fixation (24/29 studies). It also should be noted that failure of fixation is a rare complication and was not reported in any of the included studies, making it unlikely that implant differences were an important factor. Finally, the largest limitation may be that the primary purpose of the included studies was to report results rather than complications, which could have caused underreporting of stiffness, in particular.
Conclusion
The study findings suggest that both open and radiographic localization of femoral graft position in MPFL reconstruction offer similar outcomes. We found no significant differences in the rates of postoperative apprehension, postoperative subjective instability, postoperative objective instability, reoperations, recurrent dislocation, or arthrofibrosis when comparing open and fluoroscopic techniques. Surgeons can choose either technique and expect similar results.
Footnotes
Notes
Final revision submitted September 30, 2022; accepted October 21, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: K.H. has received grant support from Arthrex; education payments from Arthrex, Smith & Nephew, and Rock Med; and hospitality payments from Zimmer Biomet. C.C. has received grant support from Arthrex and education payments from Arthrex and Smith & Nephew. B.J.L. has received education payments from Prodigy Surgical. L.B. has received royalties from Zimmer Biomet and hospitality payments from Arthrex and Prodigy Surgical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.