
Abstract
Background:
The pattern of glenoid bone loss (GBL) in anterior glenohumeral instability is well described. It was recognized recently that posterior GBL after instability has a posteroinferior pattern.
Purpose/Hypothesis:
The purpose of this study was to compare GBL patterns in a matched cohort of patients with anterior versus posterior glenohumeral instability. The hypothesis was that the GBL pattern in posterior instability would be more inferior than the GBL pattern in anterior instability.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
In this multicenter retrospective study, 28 patients with posterior instability were matched with 28 patients with anterior instability by age, sex and number of instability events. GBL location was defined using a clockface model. Obliquity was defined as the angle between the long axis of the glenoid and a line tangent to the GBL. Superior and inferior GBL were measured as areas and defined relative to the equator. The primary outcome was the 2-dimensional characterization of posterior versus anterior GBL. The secondary outcome was a comparison of the posterior GBL patterns in traumatic and atraumatic instability mechanisms in an expanded cohort of 42 patients.
Results:
The mean age of the matched cohorts (n = 56) was 25.2 ± 9.87 years. The median obliquity of GBL was 27.53° (interquartile range [IQR], 18.83°-47.38°) in the posterior cohort and 9.28° (IQR, 6.68°-15.75°) in the anterior cohort (P < .001). The mean superior-to-inferior bone loss ratio was 0.48 ± 0.51 in the posterior cohort and 0.80 ± 0.55 (P = .032) in the anterior cohort. In the expanded posterior instability cohort (n = 42), patients with traumatic injury mechanism (n = 22), had a similar GBL obliquity compared to patients with an atraumatic injury mechanism (n = 20) (mean, 27.73° [95% CI, 20.26°-35.20°] vs 32.20° [95% CI, 21.27°-43.14°], respectively) (P = .49).
Conclusion:
Posterior GBL occurred more inferiorly and at an increased obliquity compared with anterior GBL. This pattern is consistent for traumatic and atraumatic posterior GBL. Bone loss along the equator may not be the most reliable predictor of posterior instability, and critical bone loss may be reached more rapidly than a model of loss along the equator may predict.
Keywords
Posterior glenohumeral instability is an increasingly recognized cause of shoulder pain and dysfunction 17,21,27,33 and may present with a nonspecific complaint of pain without an obvious history of dislocation or subluxation, which can pose a diagnostic challenge. 21 –23 The etiology of posterior instability is variable, with causes including repetitive microtrauma (especially with the shoulder in a flexed and internally rotated position), acute trauma, or ligamentous laxity. 11 Proposed risk factors for recurrent posterior instability include an age <40 years at the first instability event, dislocations related to seizures, large reverse Hill-Sachs lesions, increased glenoid retroversion, glenoid bone loss (GBL), and glenoid dysplasia. 6,8,20,23
While anterior instability has been studied extensively and well-accepted algorithms exist, literature on posterior instability continues to evolve. 4,9,18,25,26 Recent literature has attempted to establish the posterior GBL threshold beyond which capsulolabral repair alone is insufficient in the management of posterior instability. Arner et al 1 report a smaller glenoid width and a greater percentage of bone loss to be associated with failure of posterior labral repair. This study found a threshold of 11% bone loss to be associated with a 10.4 times greater risk of posterior labral repair failure, and a threshold of 15% was associated with a 24.4 times greater risk of failure. 1 Similarly, Bradley et al 5 found a smaller glenoid bone width to be a risk factor for revision following posterior labral repair. Another study reported GBL >13.5% to be associated with an increased failure rate following arthroscopic labral repair. 31 While Hines et al 16 did not find GBL to predict failure of posterior labral repair, those with >13.5% GBL were less likely to return to full military duty. Finally, a cadaveric model has suggested that bony augmentation is warranted with GBL >20%. 19
It has been suggested that differences exist between the GBL patterns of anterior and posterior instability, with posterior bone loss occurring more inferiorly relative to anterior bone loss. 19 However, posterior bone loss patterns have not been compared directly with bone loss patterns in a matched cohort of patients with anterior instability. As with anterior instability, a full understanding of GBL morphology in posterior glenohumeral instability is a critical step in surgical planning.
The objective of this study was 2-fold: (1) to characterize the pattern of GBL in shoulders with posterior instability in comparison to a matched cohort of anterior instability patients and (2) to determine if the posterior GBL pattern varied according to traumatic or atraumatic mechanisms. We hypothesized that posterior GBL would be located more inferiorly compared with anterior GBL. We also hypothesized that the bone loss patterns of chronic posterior subluxation would be more inferior than those of traumatic posterior instability.
Methods
Patient Selection
This study was determined to be exempt from institutional review board approval. A multicenter, retrospective matched cohort study was performed to identify the GBL patterns of posterior glenohumeral instability in comparison to the bone loss patterns seen in primary anterior glenohumeral instability. Patients with isolated anterior and isolated posterior glenohumeral instability at 2 academic medical centers were identified from 2008 to 2018 via review of patient records and International Classification of Diseases, Ninth/Tenth Revision (ICD-9/ICD-10) diagnosis codes (ICD-9: 831.00-02; ICD-10: S43.011-2, S43.014-5, S43.021-2, S43.024-5) and were confirmed by chart review. Inclusion criteria were as follows: age <65 years; history of isolated anterior or posterior instability (eg, documented unidirectional subluxation or dislocation); examination findings consistent with anterior or posterior glenohumeral instability (eg, apprehension for anterior instability, Kim test for posterior instability); anterior or posterior labral tear on imaging in conjunction with another positive finding (eg, pain, dislocation/subluxation, or exam findings of instability); available preoperative magnetic resonance imaging (MRI) or computed tomography (CT) of the affected shoulder with an en face view of the glenoid; and GBL as described below. Exclusion criteria were a history of previous glenohumeral stabilization procedures before imaging, incomplete imaging availability, or a lack of GBL.
Matched Anterior Instability Cohort
Patients with posterior instability who met inclusion and exclusion criteria were matched 1:1 to patients with anterior instability. Patients were matched by age at first instability event (within 3 years), sex, number of instability events (single vs multiple), and characterization of symptoms (pain, apprehension, or both) (Figure 1). Patients who did not have an exact match based on these criteria were excluded from comparative evaluations. Overall, 28 patients with posterior instability were matched to 28 patients with anterior instability. The advanced imaging modality in the anterior cohort was an MRI scan in 20 patients and CT scan in 8 cases. The advanced imaging modality in the matched posterior instability cohort was an MRI scan in 27 cases and a CT scan in 1 case.
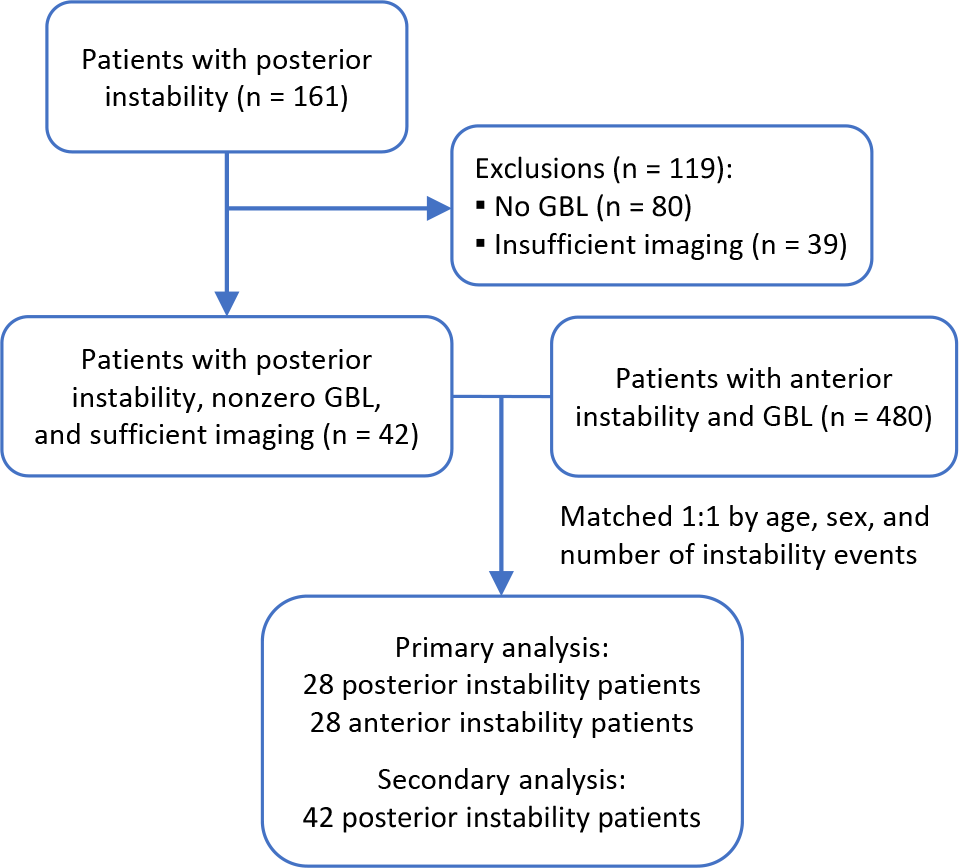
Flow diagram demonstrating patient selection. GBL, glenoid bone loss.
Glenoid Version and Morphology
Glenoid version was measured on the axial MRI or CT slices at the midglenoid point using the Friedman technique. 12,13 A straight line bisected the glenoid fossa and extended to the most medial edge of the scapula. A second line was drawn perpendicular to this line (line A). Next, a line was drawn across the face of the glenoid from the anterior to posterior glenoid rim (line B). Glenoid version was calculated as the angle formed between lines A and B. Retroversion was expressed as a positive number and anteversion as a negative value. Axial cuts of the glenoid were also assessed for glenoid dysplasia, which was described qualitatively as pointed, delta, or lazy-J. 10,30
GBL Measurements
The perfect-circle technique was used to measure GBL, as previously described. 15,28 A sagittal image with the glenoid en face was exported to PowerPoint (Microsoft) and a best-fit perfect circle with equal height and width was applied to the inferior two-thirds of the glenoid. The image was then opened with ImageJ software (National Institutes of Health) and the percentage of total area GBL was calculated using the freehand trace function (Figure 2A). Linear bone loss at the glenoid equator (percentage of the diameter of perfect circle) and linear bone loss along the axis of greatest bone loss (percentage of the diameter of perfect circle) (Figure 2B) were determined using the line function. The area of bone loss below and above the equator were measured separately and divided to determine the ratio of superior-to-inferior GBL. The location of GBL, including the axis of greatest GBL and the borders of the defect, were described relative to the clockface convention with the 12-o’clock position at the bony landmark of the supraglenoid tubercle (Figure 2C). Left shoulders were transposed to a right-shoulder configuration such that the 9-o’clock position corresponded to the posterior glenoid in all cases. The superior border of the defect was termed the “start point” of the defect and was assigned a clockface designation. The obliquity of GBL from the long axis of the glenoid was measured as previously described (Figure 2D). 7 All measurements were completed by 2 pairs of senior orthopaedic residents (M.G.L and M.P.K.; M.D.B and A.E.L.). Measurement techniques were discussed and standardized before initiation of the study in attempt to maximize accuracy.

Glenoid measurements. (A) GBL area (red). (B) Linear bone loss along the axis of greatest loss. (C) Range of bone loss using a clockface model. (D) Obliquity of GBL measured as an angle between the long axis of the glenoid and a line tangent to the GBL. GBL, glenoid bone loss
Study Outcomes
The primary outcome of this study was the 2-dimensional characterization of GBL in posterior instability patients (n = 28) and their matched anterior instability cohort (n = 28) with the following measurements: ratio of superior-to-inferior GBL, clockface location of GBL, and obliquity of GBL (in degrees). A secondary analysis was performed on an expanded cohort of posterior instability patients (n = 42) to assess the influence of additional variables such as traumatic or atraumatic mechanism of injury on GBL area and pattern. Patients with atraumatic posterior shoulder instability had a history and examination consistent with posterior instability but did not recall an event of frank dislocation. The advanced imaging modality in the expanded posterior instability cohort was an MRI in 38 cases and a CT scan in 4 cases.
Statistical Analysis
Continuous variables were calculated and expressed as the mean and standard deviation or 95% CI. The D’Agostino-Pearson test was used to determine normality. In the case of nonparametric data, the median and interquartile range (IQR) were reported. Frequencies and proportions were calculated for categorical variables. Independent t tests or Mann-Whitney U tests were used to compare continuous data based on normality. Reliability was measured by the intraclass correlation coefficient (ICC) using a 2-way random-effects model, based on the measurements of 2 raters and assessing absolute agreement. ICC was reported for several measurements that were representative of the techniques employed for all other measurements. Significance was set at P < .05. Calculations were performed using MedCalc Statistical Software Version 19.6 (MedCalc Software Ltd).
Results
Patient Demographics
Fifty-six patients (28 anterior GBL, 28 posterior GBL) were included in the matched cohort analysis. The average age was 25.2 ± 9.87 years (range, 14-47 years) with 54 (96.4%) male patients. Of the 42 patients in the expanded posterior instability cohort, 36 (85.7%) were male, and the mean age was 28.4 ± 11.73 years (range, 14-53 years). In the expanded posterior instability cohort, the initial instability event was traumatic and resulted in frank dislocation in 22 (52.4%) patients; of these events, the mechanism was related to sports (n = 12), motor vehicle collision (n = 2), seizure (n = 2), or unspecified trauma (n = 6). A total of 20 posterior instability patients reported chronic subluxation without a known dislocation event.
Comparison of Posterior and Anterior Bone Loss
The bone loss patterns in the posterior and anterior instability groups were compared (Table 1). Bone loss obliquity was significantly greater in the posterior GBL group (median, 27.53°; IQR, 18.83°-47.38°) compared with the anterior GBL group (median, 9.28°; IQR, 6.68°-15.75°; P < .001) (Figures 3 and 4). The mean axis of greatest loss in the matched posterior cohort was 117.74° from the supraglenoid tubercle (95% CI, 107.31°-128.18°) compared with 99.83° (95% CI, 91.03°-108.63°) in the anterior cohort (P = .009).
Comparison of Matched Posterior and Anterior Instability Groups a

a Data are presented as median (interquartile range) or mean ± SD. Boldface P values indicate statistically significant difference between groups (P < .05). GBL, glenoid bone loss.
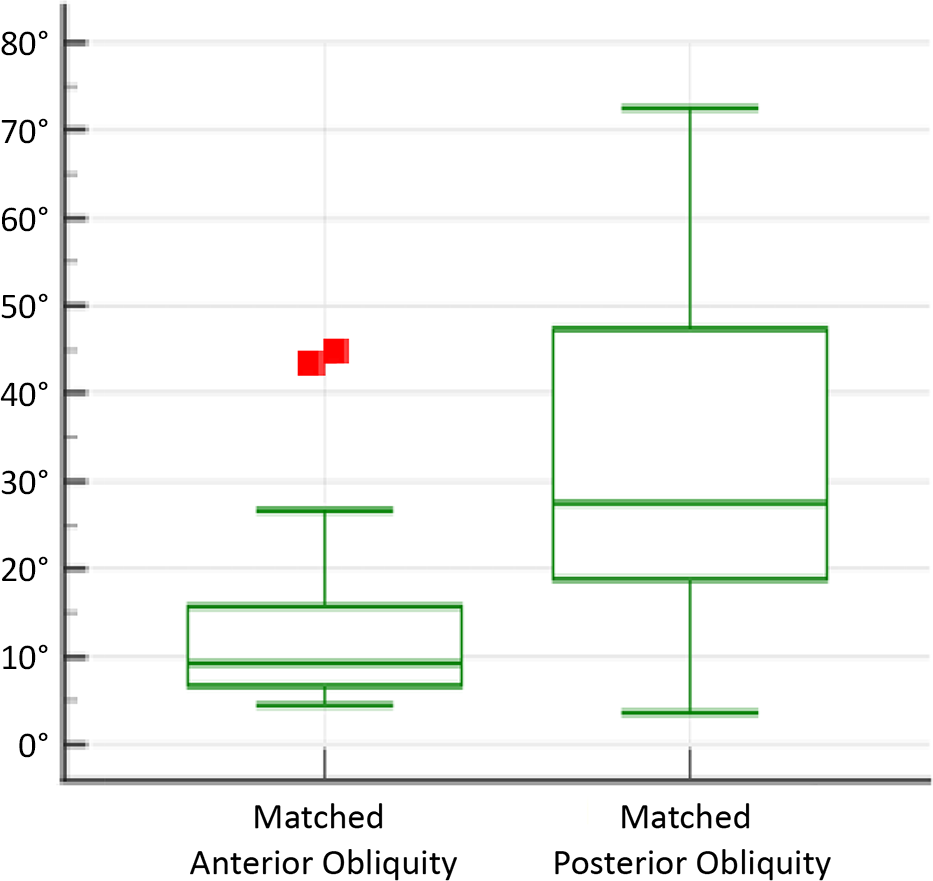
Distribution of obliquity in the anterior versus posterior instability groups. The center line represents the median, the top and bottom of the box represent the interquartile range, and the whiskers indicate the maximum and minimum values. The red squares represent outliers.

Sketch of mean (A) posterior and (B) anterior glenoid bone loss location and obliquity (yellow shading). (C) Example of posterior bone loss on T1 magnetic resonance imaging. (D) Example of anterior bone loss on computed tomography 3-dimensional reconstruction.
The start point of posterior GBL was significantly more inferior than that of anterior GBL. The posterior median value was 64.85° (IQR, 58.30°-82.36°) compared with the anterior median value of 53.54° (IQR, 39.62°-67.62°) (P = .007). While the mean total arc of bone loss was less in the posterior group (83.28° ± 24.62°) compared with the anterior group (93.22° ± 29.77°), this did not reach statistical significance (P = .18).
The ratio of superior-to-inferior GBL was significantly greater in the anterior instability group (0.80 ± 0.55) compared with the posterior instability group (0.48 ± 0.51) (P = .032).
Anterior Bone Loss
For the 28 shoulders in the anterior bone loss cohort, the mean ratio of superior-to-inferior loss was 0.80 (95% CI, 0.58-1.01). Bone loss ranged from the 1:54 to 4:55 clockface positions. The mean arc of bone loss was 93.22° (95% CI, 81.68°-104.76°). The axis of greatest loss occurred at 3:20. The linear loss along this axis was 4.67% (95% CI, 3.08-6.25). The linear loss alone the equator was 3.47% (95% CI, 1.84%-5.11%). The median obliquity from the long axis of the glenoid was 9.28° (IQR, 6.68°-15.75°).
Posterior Bone Loss
For the 42 shoulders in the expanded posterior instability cohort, the mean total area of the posterior GBL (relative to the surface area of the best-fit circle on the face of the inferior glenoid) was 7.77% (95% CI, 6.03%-9.50%). The ratio of superior to inferior bone loss was 0.50 (95% CI, 0.36-0.65). Using the clockface convention with the supraglenoid tubercle at 12-o’clock, the bone loss range extended from 9:43 to 6:48. The mean arc of bone loss was 87.81° (95% CI, 80.76-94.86°). The axis of greatest loss occurred at 8:11. The linear bone loss along this axis was 12.50% (95% CI, 10.08%-14.92%) and was significantly greater than the linear posterior loss at the equator, 5.95% (95% CI, 4.23%-7.67%) (P < .001). The mean obliquity from the long axis of the glenoid was 29.89° (95% CI, 23.62°-36.15°).
Glenoid Version and Morphology
Glenoid version was compared between the matched cohorts. The mean glenoid retroversion in the posterior instability cohort was significantly greater than that of the anterior cohort (8.69° [95% CI, 6.05° to 11.33°] vs 5.37° [95% CI, 3.50° to 7.24°], respectively; P = .037). There was a positive correlation between glenoid retroversion and total area of posterior GBL (r = 0.580; 95% CI, 0.264 to 0.783; P = .0012). The glenoid morphology in the setting of posterior instability was characterized as delta in 25 (59.5%), lazy-J in 10 (23.8%), and pointed in 7 (16.7%) cases. In the anterior instability cohort, the glenoid morphology was characterized as delta in 5 (17.9%), lazy-J in 8 (38.6%), and pointed in 15 (53.6%) cases.
Mechanism of Injury in Posterior Bone Loss
The mechanism of injury was not found to influence the location or extent of GBL in shoulders with posterior instability. The mean total posterior GBL after traumatic injury (n = 22; 8.67% ± 6.50%) was not significantly different from the GBL observed in atraumatic instability (n = 20; 6.78% ± 4.30%) (P = .28). Regarding the location of GBL, the axis of greatest GBL after traumatic instability was 116.55° ± 25.08° compared with 112.69° ± 27.39° in patients with atraumatic instability (P = .69). In patients with traumatic shoulder instability, the mean obliquity was 27.73° (95% CI, 20.26-35.20°), compared with 32.20° (95% CI, 21.27-43.14) in patients with atraumatic instability (P = .49).
Reliability of Measurements
The ICCs for interobserver reliability were 0.98 (95% CI, 0.91-0.99) for the total area loss measurements and 0.96 (95% CI, 0.84-0.99) for obliquity measurements, indicating excellent agreement.
Discussion
The present study demonstrates that, in matched shoulders with unidirectional instability, posterior GBL is more inferior than anterior GBL. In addition, the bone loss patterns in traumatic and atraumatic posterior instability are similar. As the prevalence of posterior instability is becoming increasingly recognized, 20,27,33 understanding the GBL location and extent in posterior instability is vital to guide repair or reconstruction. While anterior instability has been studied widely and evidence-based guidelines have been established to guide management in the setting of bone loss, 3,9,25 such evidence is developing for posterior instability. Previous studies have characterized the morphology and location of posterior GBL, 2,7 but the present study uniquely compares anterior and posterior GBL patterns in a matched cohort and describes posterior bone loss according to traumatic or atraumatic onset.
Previous studies have evaluated the morphology of posterior GBL, but comparisons with anterior GBL patterns have been limited to historical data. 2,7 Beaulieu-Jones et al 2 studied the posterior GBL patterns in 40 young, active patients. The authors found posterior GBL to be associated with increased glenoid retroversion, but retroversion was not associated with the size of the defect. The present study demonstrated a moderate correlation between glenoid retroversion and the total area of GBL. Beaulieu-Jones et al also demonstrated that posterior GBL has a more anterior to posterior slope, whereas anterior GBL is typically 90° to the glenoid face. 2 Dekker et al 7 further described the posterior GBL location with the methods utilized in the present study. The authors showed posterior GBL occurs from 6:44 to 9:28, which is similar to the findings in the present study from 6:48 to 9:43. Similarly, the average obliquity of 29.89° in the present study nearly matches the previously reported 30.7°, demonstrating consistency between cohorts and reviewers. Indeed, we demonstrated excellent reliability between reviewers in the present study.
The present study is the first to directly compare the location of GBL between anterior and posterior instability cohorts. Our findings suggest that the obliquity of posterior GBL is significantly more oblique than that in anterior instability. In the matched cohorts in the present study, the median posterior obliquity was 27.53° compared with 9.28° in the anterior cohort (P < .001). Bone loss patterns in anterior instability are relatively parallel to the long axis of the glenoid. The obliquity of nearly 10° in the present study differs from previous the findings of Saito et al, 24 who described the anterior GBL obliquity to be 0.5° from parallel to the long axis of the glenoid. This discrepancy may be due to the different technique used to measure obliquity in the former study. To further emphasize the proportion of inferior bone loss in posterior instability, the ratio of superior-to-inferior GBL was 0.48 in the posterior instability cohort compared with 0.80 in the anterior instability cohort. While former studies have relied on historical comparisons of GBL between anterior and posterior instability, 2,7 these results further quantify the differences in a matched cohort.
Recent studies have estimated the “critical” posterior GBL to range from 11% to 20%. 1,19,31 While the determination of the extent of posterior GBL is important, it is also important to recognize the location of the bone loss. Early attempts to define the critical GBL in posterior instability were modeled according to anterior GBL patterns, 19 which is relatively vertical and parallel to the long axis of the glenoid. 24 Nacca et al 19 showed that reverse Bankart repair is insufficient for posterior GBL >20% in a cadaveric model. The authors utilized vertical osteotomies parallel to the long axis of the glenoid, as was performed in an analogous cadaveric study for the critical anterior GBL by Yamamoto et al. 32 Clinical studies have reported critical posterior GBL to be much lower than that predicted by the cadaveric model, where 11% posterior GBL was associated with a 10-fold greater failure rate with arthroscopic capsulolabral repair. 1 This difference between cadaveric and clinical studies may be related to the findings in the present and former studies, where posterior GBL has a more oblique orientation and is more inferior than anterior GBL. 2,7 Therefore, future cadaveric studies for posterior GBL should utilize these findings to create models that more closely align with in vivo bone loss patterns.
A novel finding of this study was the similar posterior GBL locations in patients with traumatic and atraumatic posterior instability. There was no significant difference in the obliquity of GBL between patients with traumatic posterior shoulder dislocations (mean, 27.73°) and in those who experienced chronic subluxation without a frank dislocation event (mean, 32.20°). It is interesting to consider that, whereas posterior bone loss approached the scapular spine in our cohort, it rarely extended superior to the spine (see Figure 3). We hypothesize that the scapular spine and the acromion may play a role in the posteroinferior direction of posterior instability, which should be further explored in future studies. This theory may account for the consistency in bone loss location in traumatic and atraumatic posterior GBL patterns. These findings suggest that surgeons can generally expect to find a consistent location of posterior GBL that will guide reconstruction, regardless of the injury mechanism.
Posteroinferior GBL, which does not run parallel to the long axis of the glenoid, has implications for proper reconstruction of these defects. While the present study did not investigate bony augmentation procedures, it does highlight the difference in bone loss patterns between anterior and posterior instability. If the goal of bone block procedures is to replace the bone that has been lost, then it follows that the positioning of anterior and posterior bone blocks should not be symmetric. To reconstruct GBL more accurately in cases of increased obliquity from the long axis of the glenoid, a bone block would match this angle, with a more cephalad screw trajectory than its anterior counterpart.
Limitations
This study has some limitations. First, the study was limited by the retrospective study design. Second, this was a radiographic study, preventing an analysis of the influence of bone loss location on clinical and patient-reported outcomes. Third, measurements were performed by orthopaedic residents who had practice performing these measurement techniques before initiation of the study. While excellent interobserver ICC values were found, this reliability may not be generalizable. Fourth, we used both MRI and CT scans in the analysis. While CT scans are the gold standard for assessing bone loss, MRI has been shown to be accurate and reliable for the measurement of GBL. 14,29 In addition, MRI studies have been used recently to define posterior critical bone loss. 1 Given that the present study relied on proportions of bone loss, rather than absolute bone loss, the use of both imaging modalities is not likely to influence the results of the study.
Conclusion
In the current study, posterior GBL occurred more inferiorly and at an increased obliquity compared with anterior bone loss. Traumatic and atraumatic posterior shoulder instability generated similar posterior GBL patterns. Recognition of posterior GBL patterns is important when considering reconstruction and future cadaveric studies on posterior GBL.
Footnotes
Acknowledgment
The authors thank Anna Rose Hughes for her artistic sketch of the glenoid.
Final revision submitted September 3, 2022; accepted October 11, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.D.B. has received education payments from Supreme Orthopedic Systems. S.A.H. has received education payments from Arthrex. M.N.G. has received education payments from Supreme Orthopedic Systems and speaking fees from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by the University of Maryland, Baltimore (ref. No. HP-00092361).