
Abstract
Background:
Isolated soft tissue injuries of the posterior capsulolabral complex can be addressed arthroscopically, with various anchor systems available for repair.
Purpose:
To evaluate clinical and patient-reported outcomes after arthroscopic capsulolabral repair in patients with posterior shoulder instability (PSI) and to compare differences in outcomes between patients treated with a suture-first technique (PushLock anchor) and an anchor-first technique (FiberTak all-suture anchor).
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Included were 32 patients with dynamic structural PSI (type B2 according to the ABC classification) treated with an arthroscopic posterior capsulolabral repair. After a mean follow-up time of 4.8 ± 3.4 years (range, 2-11) patients were evaluated clinically, and standardized outcome scores were obtained for the Subjective Shoulder Value (SSV), the Western Ontario Shoulder Instability Index (WOSI), Rowe, Kerlan-Jobe Orthopaedic Clinic (KJOC), patient satisfaction (0-5 [best]), and pain on a visual analog scale (VAS; 0-10 [worst]).
Results:
The overall satisfaction level with the outcome of the surgery was 4.6 ± 0.5 (range, 4-5). No patient suffered from instability events. The mean VAS level for pain was 0.4 ± 0.9 (range, 0-4) at rest and 1.9 ± 2.0 (range, 0-6) during motion. The mean SSV was 80 ± 17 (range, 30-100), the mean postoperative WOSI score 75% ± 19% (range, 18-98), the mean Rowe score 78 ± 20 (range, 10-100), and the mean KJOC score was 81 ± 18 (range, 40-100) for the entire cohort. There was no significant difference between the techniques with regard to range of motion, strength, or clinical outcome scores.
Conclusion:
Arthroscopic posterior capsulolabral repair was a satisfactory method to treat structural PSI type B2 with regard to stability, pain relief, and functional restoration. The majority of patients had good outcomes. No differences in outcomes were observed between the anchor-first and suture-first techniques.
Keywords
Posterior shoulder instability (PSI) is more common than expected. A recent study suggests that up to 24% of young, highly active patients with shoulder instability problems suffer from PSI. 41 Diagnosis of PSI can be challenging, as clinical symptoms vary. 14,26,34,37 Only about one-fourth of patients report a traumatic dislocation as onset of their symptoms. 13,36 PSI often presents with subluxations that often are not recognized as instability events but rather present as pain during movement, discomfort, or functional deficits. 38,44 The detection of structural defects causing PSI can be a challenge. 16,19 The Kim test (Kim et al 25 ) and jerk test are established methods to suspect posterior capsulolabral defects; nevertheless, magnetic resonance imaging (MRI) is essential to detect soft tissue lesions. As PSI often results from microtraumatic origin in the sense of a “roll-over mechanism,” radiologic outcomes commonly will not be as impressive as in anterior instability. 1,33 When MRI results are ambiguous, the intra-articular application of contrast medium can be helpful (Figure 1). 43,48
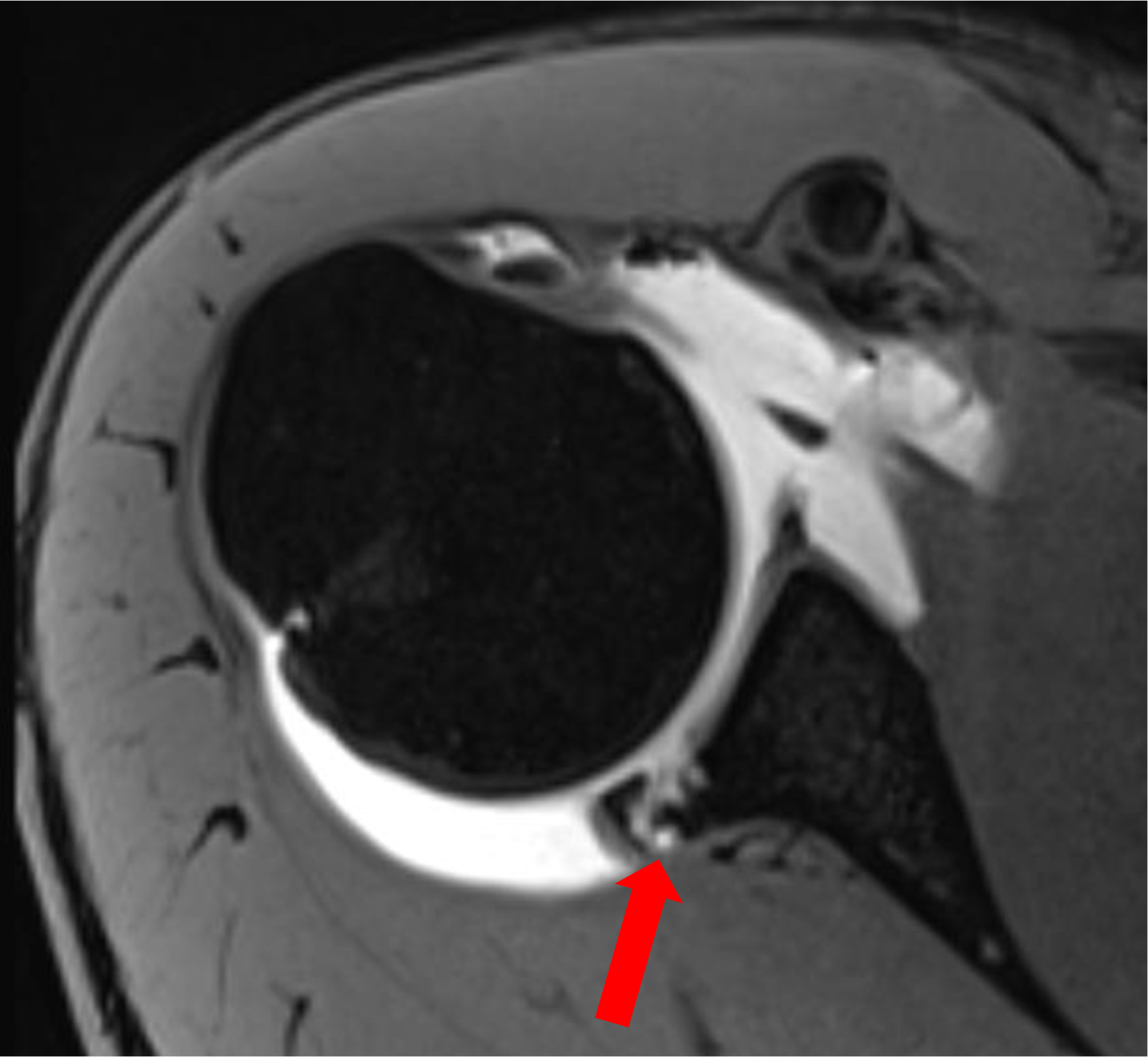
Axial magnetic resonance arthrography image of a patient with B2 posterior shoulder instability with posterior labral damage (arrow).
The ABC classification was established by Moroder et al 32 to facilitate the diagnosis of PSI and offer a treatment guideline to physicians (Figure 2). Group A stands for persons with an acute first-time event that either suffered from a posterior subluxation (type A1) or a dislocation (type A2). Group B classifies patients with recurrent dynamic PSI. While type B1 stands for a functional instability with pathologic muscle patterning, 31 type B2 describes instability caused by structural damage due to a single trauma or recurrent microtrauma. Group C describes a chronic static PSI, which might be either of constitutional (type C1) or acquired (type C2) origin.

ABC classification of posterior shoulder instability.
In the case of a painful and functionally impairing B2 PSI, surgical treatment is recommended. 22,32,42 Isolated soft tissue injuries of the posterior capsulolabral complex can be addressed arthroscopically. 7 –9,23,24,39 Various anchor systems are available for shoulder instability repair. 2,18,30,40,45
The aim of this study was to evaluate the clinical outcomes after arthroscopic posterior capsulolabral repair in patients with B2 dynamic structural PSI at midterm follow-up. 32 Specifically, we aimed to determine whether there was a difference in clinical outcome scores between patients treated with a suture-first technique (PushLock anchor; Arthrex) compared with an anchor-first technique (FiberTak all-suture anchor; Arthrex). We hypothesized that arthroscopic posterior capsulolabral repair will result in good clinical outcomes regardless of the anchor system used.
Methods
Study Population
In this retrospective study, we reviewed the records of 48 consecutive patients who suffered from B2 dynamic structural PSI who underwent arthroscopic capsulolabral repair between 2010 and 2019. Exclusion criteria were multidirectional instability, glenoid retroversion greater than 15°, Samilson-Prieto radiographic osteoarthritis grade of 2 or above, or previous surgical treatment of the affected shoulder.
A total of 41 patients who met the inclusion and exclusion criteria were identified. All patients had preoperative MRI. Patients with questionable glenoid retroversion had additional computed tomography imaging. All patients were invited for follow-up examination at our hospital; 8 patients were lost to follow-up and 1 refused to participate, leading to a follow-up rate of 78% (N = 32 patients). Ten patients could only be contacted via telephone and email/post due to relocation, and the remaining 22 patients returned for a clinical examination (flowchart displayed in Figure 3). Local ethics committee approval was obtained for this study, and written informed consent was obtained from all patients available for follow-up.

Flow diagram of patient enrollment ( a contact via telephone and email after anchor-first, 5 patients; after suture-first, 5 patients). OA, osteoarthritis.
For arthroscopic capsulolabral repair of the shoulder, the patient was positioned in the lateral decubitus position. First, a diagnostic arthroscopy was performed, including documentation of accompanying pathologies such as cartilage damage or lesions of the rotator cuff or biceps tendon. The condition of the posterior labrum and capsule was checked with a tactile hook. Afterward, the posterior capsulolabral complex was mobilized (Figure 4A) and the glenoid rim freshened with a rasp or shaver.

Capsulolabral repair with the suture-first technique. (A) After mobilizing the posterior capsulolabral complex, (B) a looped FiberWire was passed through the posterior capsulolabral complex with the help of a SutureLasso, and (C) the free ends were then pulled through the looped end to create a cinch stitch. (D) The cinch stitch was then fixed to the posterior glenoid rim using a PushLock anchor. The steps were repeated with as many anchors as needed for complete refixation.
In our clinic, the PushLock anchor system was used until 2016. For this knotless suture-first technique, a SutureLasso (Arthrex) was passed through the capsulolabral tissue. A nitinol wire loop was advanced through the SutureLasso and retrieved through the anterior portal. A looped suture was loaded through the nitinol wire loop and retracted with the SutureLasso shuttling the looped suture through the tissue (Figure 4B) and out the posterolateral portal. A grasping device was passed through the looped end of the suture and used to retrieve the open ends of the suture also via the posterolateral portal, thus forming a cinch-stitch (Figure 4C). Afterward, a drill guide was inserted through the posterolateral portal and placed onto the glenoid rim at a 45° angle. After drilling, the PushLock was advanced into the joint and the suture tensioned to approximate the labral tissue to the eyelet. The anchor was then hammered in the drill hole (Figure 4D) and the ends of the suture were cut. The steps were repeated with as many anchors as needed for complete refixation.
The change from suture-first to anchor-first technique with all-suture anchors occurred gradually starting in 2015. The posterior capsulolabral complex was mobilized in the same manner as described before (Figure 5A). The FiberTak all-suture anchor was then placed into a drillhole at the prepared glenoid bone bed at a 45° angle through a posterolateral portal (Figure 5B). By pulling the suture, the anchor was firmly set into the bone. Both ends of the suture were shuttled through the posterior capsulolabral complex using a suture lasso (Figure 5C), and both ends were tied to form a mattress stitch reattaching the labrum to the posterior glenoid (Figure 5D). The steps were repeated with as many anchors as needed for complete refixation.

Capsulolabral repair with the anchor-first technique. (A) Mobilization of posterior capsulolabral complex. (B) FiberTak all-suture anchor at the bony edge of the posterior glenoid rim. (C) Suture lasso used to pass both suture ends through the capsulolabral complex. (D) Knot tied to create a mattress stitch to reattach the labrum.
The postoperative protocol was the same for every patient and consisted of 6 weeks of immobilization in an abduction bandage with passive movement and range of motion restriction; in particular, internal rotation (IR) was forbidden for the first 6 weeks.
Follow-up Examination and Patient-Reported Outcomes
At follow-up, all patients were evaluated by a single investigator (K.K.) who was not involved in the surgical procedure. The questionnaire-based follow-up examination included questions about general sociodemographic data (sex, age, dexterity, height, weight) as well as postoperative complications or revision surgery concerning the affected shoulder. The clinical evaluation started with a standardized physical examination of both shoulders, including the measurement of active range of motion (forward flexion, abduction, external rotation [ER] and IR at 0° and 90° of abduction) with the use of a goniometer and isometric muscle strength captured with a dynamometer placed at the wrist for abduction (Jobe position) and ER and IR at 0° of abduction. Patients who were not capable of attending the examination in person were asked to evaluate their shoulder range of motion according to pictures they were shown. A total of 22 patients who attended the follow-up examination in person performed strength measurements.
The patients were asked about their satisfaction with surgery (0 = not satisfied at all, 5 = very satisfied) and pain level during rest and movement captured with a visual analog scale (VAS) (0 = no pain, 10 = worst pain). This was followed by 3 pathology-specific questionnaires. The first was the Western Ontario Shoulder Instability Index (WOSI), whose primary aim was to evaluate the outcome after shoulder instability treatment. 27 After conversion to a 0% to 100% scale, a higher percentage stood for a good shoulder function. This was followed by the Rowe score. In addition, the patients’ ability in performing sports with focus on overhead activities was queried using the Kerlan-Jobe Orthopaedic Clinic Shoulder and Elbow Score (KJOC) with a maximum of 100 points achievable. 3 Furthermore, the Subjective Shoulder Value (SSV) was captured. It reflects the patient’s assessment of the operated shoulder as a percentage of a healthy shoulder, which would score 100%. 17 The patients were supported by a clinical research assistant to complete the questionnaires.
Statistical Analysis
Statistical analysis was performed using SPSS software (Version 27; IBM). Descriptive statistics were calculated including means, standard deviation, minimum values, and maximum values. The Kolmogorov-Smirnoff test was used to test all data for normal distribution. To evaluate the range of motion and strength between the affected and the healthy shoulder, the Wilcoxon signed-rank test was calculated. The differences in clinical results between treatment groups were evaluated with the Mann-Whitney test. A P value of <.05 was considered significant.
Results
Patient Demographics
The sociodemographic data of the patient cohort can be seen in Table 1. There was a significant difference between the anchor-first and suture-first groups with regard to the follow-up period (P < .001). There were no significant differences between the groups in age, sex, body mass index, dexterity, or number of anchors used.
Patients Characteristics and Number of Anchors Used for Stabilization a

a Data are reported as mean ± SD (range) unless otherwise indicated. Boldface P value indicates statistically significant difference between anchor-first and suture-first groups (P < .05).
Postoperative Clinical Results and Subgroup Analysis
With regard to range of motion, there was a small but significant loss of IR between the operated and the healthy shoulder at 0° of abduction (86° ± 9° vs 88° ± 4°; P = .023) and 90° of abduction (69 ± 13° vs 72 ± 9°; P = .039) (Table 2). There was no significant difference in postoperative range of motion between the 2 technique groups (Table 2).
Comparison of Range of Motion Between Operated and Healthy Shoulders and Between Technique Groups a
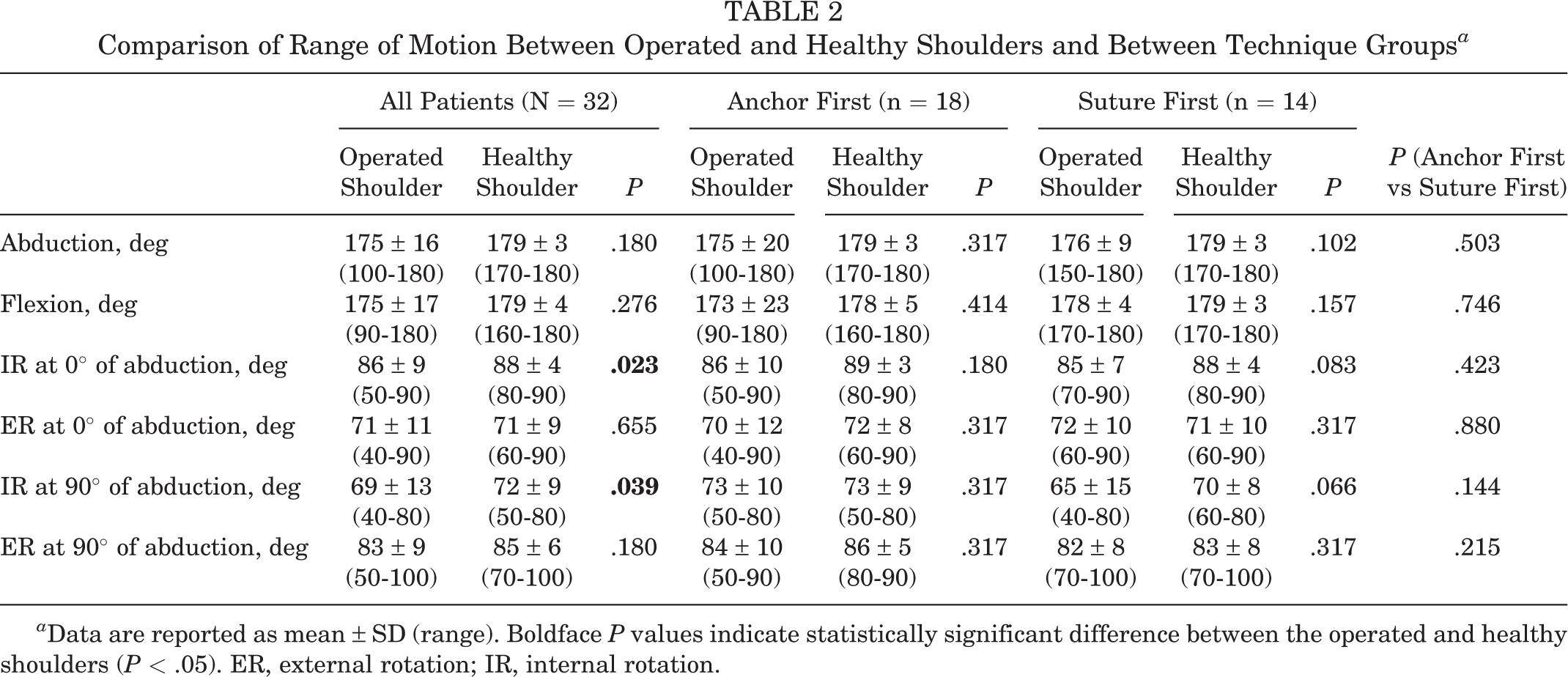
a Data are reported as mean ± SD (range). Boldface P values indicate statistically significant difference between the operated and healthy shoulders (P < .05). ER, external rotation; IR, internal rotation.
The mean values reached for abduction, IR and ER strength can be seen in Table 3. There was no significant difference in achieved strength when comparing the 2 technique groups.
Comparison of Strength Between Operated and Healthy Shoulders and Between Technique Groups a
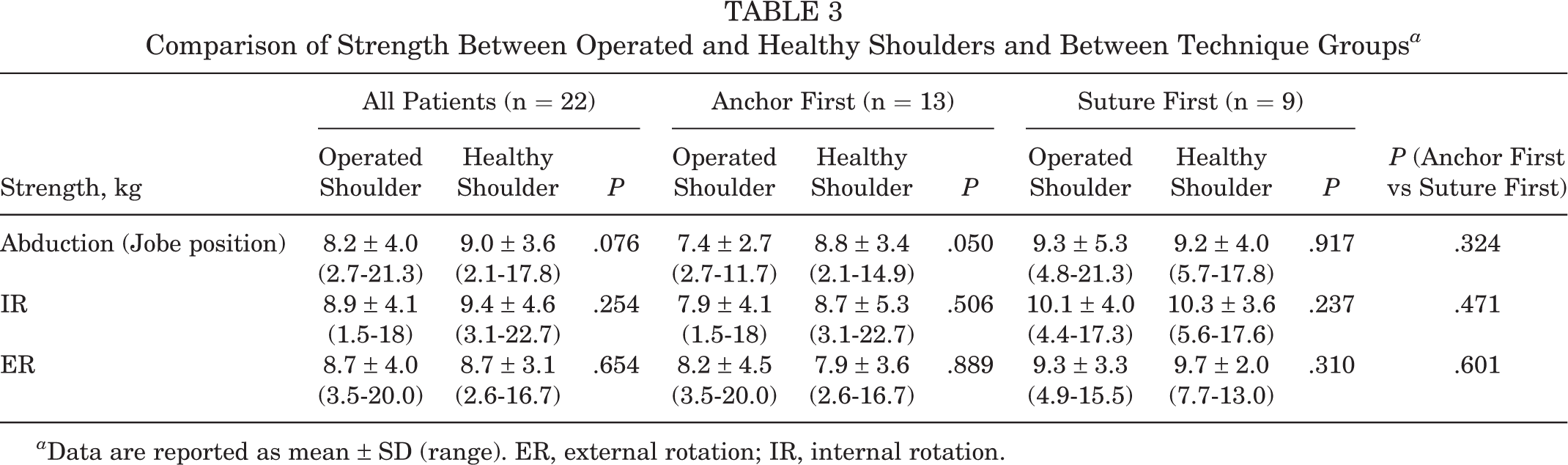
a Data are reported as mean ± SD (range). ER, external rotation; IR, internal rotation.
No patients reported any instability events, and no patients required reoperation. The mean VAS level for pain was 0.4 ± 0.9 (range, 0-4) at rest and 1.9 ± 2.0 (range, 0-6) during motion. The mean SSV was 80 ± 17 (30-100), the mean postoperative WOSI score was 75% ± 19% (18%-98%), the mean Rowe score 78 ± 20 (10-100), and the mean KJOC score was 81 ± 18 (40-100) for the entire cohort. The results of the achieved scores and subgroup distinction can be seen in Table 4. There was no significant difference between both groups for satisfaction, VAS, WOSI, Rowe, SSV, or KJOC score.
Comparison of Patient-Reported Outcomes Between Technique Groups a

a Data are reported as mean ± SD (range). KJOC, Kerlan-Jobe Orthopaedic Clinic; SSV, Subjective Shoulder Value; VAS, visual analog scale; WOSI, Western Ontario Shoulder Instability Index.
Discussion
In this retrospective study, most patients who suffered from structural dynamic PSI type B2 who were treated with arthroscopic capsulolabral repair showed good clinical results in terms of functional outcomes, stability, pain, and satisfaction at midterm follow-up, independent of the used arthroscopic anchor technique. In addition, range of motion and strength were comparable with those of the contralateral healthy shoulder.
The nonsignificant reduction in abduction strength of patients in the anchor-first group compared with the contralateral healthy shoulder and with patients in the suture-first group might be explained by the significantly shorter follow-up period of patients in anchor-first group, as the periscapular muscles, and especially deltoid muscle, may need time to fully regenerate after surgery. Furthermore, there was a small but significant difference for IR at 0° as well as 90° abduction when comparing the operated and the healthy shoulder. The reduced postoperative IR is most likely due to posterior capsulolabral gathering. This phenomenon is described in the same manner for ER when examining patients after anterior shoulder stabilization. 11,29,45 The reduced shoulder rotation underlines once more that it is important not to tighten the capsule too much and find the right balance between avoiding instability and allowing the patient a free range of motion. 21 Nevertheless, measuring error should be taken into account, as in clinical practice it is barely possible to reliably measure a range of motion of <10°. Furthermore a lack of range of motion <10° will probably not be clinically relevant for the patient.
Although most patients had good-to-excellent outcome scores, 1 patient had poor clinical outcome scores. Nevertheless, the satisfaction level was high, which presumably means that this patient’s shoulder function was even worse before surgery or worsened again over time. The follow-up period for this patient was 6 years, so it can also be assumed that the patient might have developed osteoarthritis, resulting in an impaired shoulder function. 28,46 No radiograph or other imaging was performed to confirm the diagnosis within the follow-up examination.
No overall group differences with regard to postoperative scores could be detected. In this case, a prospective study with a bigger cohort and preoperative patient-reported outcome scores seems to be desirable. Still, this study underscores that midterm results are in line with other studies. 5
While several clinical outcome studies have been published on arthroscopic soft tissue repair in patients with anterior shoulder instability, 11,18,20,29,45 results after PSI are less commonly reported. 4,38 It is necessary to prove the reliability of the same stabilizing methods in patients with PSI, as the pathology is different in its biomechanical characteristics and the symptoms caused. 7,32,38 Arthroscopic posterior capsulolabral repair proved itself to provide significant improvements in terms of stability, pain, and function. 6,8 As technical methods have improved, repair with suture anchors has resulted in significantly better clinical outcomes compared with anchorless capsulolabral plications. 8,12,15 Kim et al 24 reported 96% of good and excellent results after arthroscopic labrum refixation and capsular shift in 26 cases with post-traumatic posterior subluxation using a 2.7/8-mm suture anchor. This is in line with our results, as well as the detected postoperative loss in IR. Also, Williams et al 47 examined 27 shoulders 5 years after arthroscopic repair in patients with traumatic PSI. They reported no deficit in range of motion postoperatively, muscle weakness (4/5) during ER in 2 patients, and 2 patients (8%) suffering from recurrent instability requiring additional surgery. 47 Examining a large case series of 183 athletes, Bradley et al 8 showed that 90% of all patients were able to resume their previous sport after arthroscopic posterior capsulolabral reconstruction. They stated an improved American Shoulder and Elbow Surgeons score from 45 to 86 at 3 years postoperation, which is similar to the results of the present study. 8 Our study presented a good postoperative KJOC score, indicating a satisfying return to sport rate in patients. A meta-analysis conducted by De Long et al 12 confirmed these good results, showing arthroscopic procedure to be an effective and reliable treatment option for PSI with regard to outcome scores, patient satisfaction, and return to play, although throwing athletes are less likely to return to their preinjury level compared with other athletic sports. 12,35
Limitations
The study has some limitations; the cohort size examined in this study seems to be rather small, 22% of participants were lost to follow-up, and 31% of examined patients lacked strength measurements postoperatively as they could only be contacted via telephone or mail (Figure 3). However, the cohort is quite large in comparison with studies on similar pathologies in the literature. The strength of the study is the homogeneous cohort, with diagnosis made on the basis of the ABC classification and clear inclusion and exclusion criteria. Another limitation of the study concerning sports and return to play is the lack of recording of the amount of activity or level of competition of the patients preoperatively. We evaluated the subjective restrictions of the patient with regard to resuming the sport the patient practiced before the operation. In addition, it would have been desirable to have Patient Acceptable Symptom State scores with regard to outcome measurements. 10 Furthermore, a follow-up imaging would be desirable. Nevertheless, as we do not treat images but patients, the clinical results seem to be more meaningful in clinical practice. A further strength of the study is the rather long follow-up period. Subgroup comparability was given for all parameters except the length of the follow-up period, which is explained by the fact that, in recent years, only all-suture anchors were used in our clinic. Therefore, a longer follow-up for the anchor-first technique is warranted. Preoperative scoring would have been desirable to evaluate the improvement of shoulder function postoperatively.
Conclusion
The results of our study indicated generally good outcomes after arthroscopic posterior capsulolabral repair to treat structural PSI type B2 with regard to stability, pain relief, and functional restoration. No differences in outcome were observed between the anchor-first and suture-first techniques.
Footnotes
Final revision submitted September 7, 2022; accepted September 26, 2022.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Charité Universitätsmedizin Berlin (ref No. EA2/149/21).