
Abstract
Background:
Single-step all-arthroscopic techniques have gained popularity recently in the treatment of osteochondral lesions of the talus (OLT). Concomitant subchondral bone defects led surgeons to add autologous bone grafting to the surgical procedures. Collagen scaffolds have been used widely for stabilization of the reconstruction and regeneration of the articular surface.
Purpose:
To compare single-step all-arthroscopic treatment of OLT consisting of debridement, microfracture, autologous bone grafting, and application of fibrin sealant in 2 patient groups: with versus without collagen scaffold.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Included were 94 patients who underwent single-step all-arthroscopic treatment for OLT. Autologous bone grafting was applied to 48 patients (BG group), while autologous bone grafting plus collagen scaffold was applied to 46 patients (BG+S group). A fibrin sealant was applied to both groups. Clinical outcomes were assessed with the American Orthopaedic Foot & Ankle Society (AOFAS) score and the visual analog scale (VAS) for pain. Radiological outcomes were evaluated with the magnetic resonance observation of cartilage repair tissue score. The mean follow-up time was 69.3 ± 20.7 months.
Results:
Patients in both groups showed statistically significant improvement in pre- to postoperative AOFAS and VAS scores (P < .001 for all), with no difference between groups in AOFAS and VAS score improvement. Complete healing with or without hypertrophy was achieved in 42 patients in the BG group (87.5%) and 38 patients in the BG+S group (82.6%).
Conclusion:
The treatment of bone lesions in OLT may be the ultimate goal to obtain successful outcomes, in which case using a collagen scaffold besides grafting may not affect clinical and radiological outcomes.
Osteochondral lesions of the talus (OLT) are challenging injuries for all orthopaedic surgeons because of both the poor regenerative capacity of the cartilage tissue and the insufficient vascular supply of the talar dome. 8,29 They are most commonly associated with a history of trauma to the ankle region such as sprains or fractures, and without being appropriately treated, these lesions may be the precursors of avascular necrosis. 32,45 Whereas nonoperative treatment has long been the mainstay modality for nondisplaced OLT, there has been an increasing trend toward surgical treatment in the past few decades, especially for large lesions and patients with failed conservative treatment. 39
The goal of surgical treatment in OLT is a pain-free joint, preserving function and preventing osteoarthritic changes. For this purpose, there are alternatives that work on either repairing, regenerating, or replacing talar cartilage. 32 Although various surgical techniques have been defined in the literature according to the lesion characteristics, there is still a lack of consensus to determine whether 1 intervention is superior to others in the treatment of large OLTs. 7 In addition to different advantages, variable failure rates have been reported for each procedure in the literature for long-term follow-up. Recently, the autologous matrix-induced chondrogenesis (AMIC) technique has been described for large defects of the ankle joint to overcome the existing disadvantages of previously reported surgical methods. 47 AMIC is a combined technique in which the debridement, bone marrow stimulation with microfracturing, and stabilizing of the bone marrow with a scaffold are all applied in the same, single-step, surgery. Although promising, few studies have reported long-term results of the AMIC technique for the ankle joint. 17,25 Lately, there have been a few studies in which these techniques are combined with autologous bone grafting, especially for concomitant subchondral cysts. 22,40,43 These combined techniques aim to debride the necrotic subchondral bone and apply autologous bone grafting simultaneously to maintain local revascularization and reconstruction of the talar subchondral area. 22
The purpose of the present study was to compare the results of arthroscopic reconstruction of OLT with autologous bone grafting with versus without scaffold application. Our hypothesis was that autologous bone grafting alone will have similar results in terms of clinical and radiological outcomes when compared with autologous bone grafting and collagen scaffold application.
Methods
Upon approval from our institution’s ethics committee, we retrospectively evaluated patients who were admitted to the orthopaedic department of our hospital with chronic ankle pain (>6 months), diagnosed with OLT, and underwent arthroscopic reconstruction surgery by our senior foot and ankle surgeon (B.K.) between 2010 and 2018. The indication for surgery was failure of conservative treatment for ≥6 months.
Patients with a history of previous ankle surgery; patients with concomitant kissing lesions in the ankle joint or fractures or deformities in the affected lower limbs; and patients with metabolic diseases, infection, or severe osteoarthritis were excluded from the study. Patients who had OLT smaller than 15 mm2, and who were treated with conservative methods, were also excluded. In addition, 18 patients were lost to follow-up. All included patients provided informed consent.
A total of 94 patients were included (45 female and 49 male patients; mean age, 32 years; age range, 16-52 years). The single-step arthroscopic procedure was applied with bone grafting only (without application of collagen scaffold due to lack of availability of the product on the market) to 48 patients (group BG), and bone grafting with scaffold application (which was our initial surgical technique when the product was available) was applied to 46 patients (group BG+S). The duration of symptoms before surgery was 11.6 ± 4.6 months for group BG and 9.9 ± 3.6 months for group BG+S. The average follow-up time for all subjects in the study was 69.3 ± 20.7 months (63.5 ± 22.1 months for group BG and 75.5 ± 17.5 months for group BG+S). Patient demographics and lesion characteristics were described in Table 1. Ligament reconstruction was applied to 8 patients in group BG and 12 patients in group BG+S, which was statistically nonsignificant.
Demographics of the Patients and Characteristics of the Lesions a

a BG, bone grafting; BG+S, bone grafting plus collagen scaffold.
Clinical outcomes were documented with the American Orthopaedic Foot & Ankle Society (AOFAS) ankle score and level of pain was evaluated on a visual analog scale (VAS) at both the preoperative period and the final follow-up. Radiological evaluation was performed with preoperative standard weightbearing anteroposterior and lateral ankle radiographs as well as ankle magnetic resonance imaging (MRI). In the postoperative period, MRI examination was performed on the last follow-up (Magnetom Aera, 1.5-T; Siemens) and evaluated in Digital Imaging and Communications in Medicine Viewer (Numaris/4, Version: Syngo MR E11; Siemens). Reconstructions were formed in axial, sagittal, and coronal sections with T1, T2, and turbo inversion recovery magnitude weighting. Lesion volume was calculated preoperatively with the axial, sagittal, and coronal sections of MRI modality using the volume formulas of the software and expressed as cubic millimeters. Patient MOCART (magnetic resonance observation of cartilage repair tissue) scores were determined postoperatively by a senior radiologist with >10 years of experience in sports trauma and musculoskeletal imaging and who was blinded to patient clinical data and study design. 30
Surgical Technique
All of the patients in both groups underwent single-step arthroscopic surgery performed by the same surgeon (Figure 1). Under general or spinal anesthesia, all patients were placed in the supine position and pneumatic tourniquets were used. All patients received 1 gram of prophylactic intravenous cefazolin half an hour before the tourniquet was inflated. Routine diagnostic ankle arthroscopy was performed with standard anteromedial and anterolateral arthroscopic portals. Following the verification of OLT, the osteochondral fragment was removed. Debridement of the bone defect was performed until the native healthy bone (identified by the hardening sense of the bone through manual probe examination after the complete removal of the soft bone) was seen. Microfracture at the floor of the bone defect was applied with the help of an awl. The defect was then filled completely with cancellous bone graft, which was harvested from the ipsilateral iliac crest through a mini-incision.
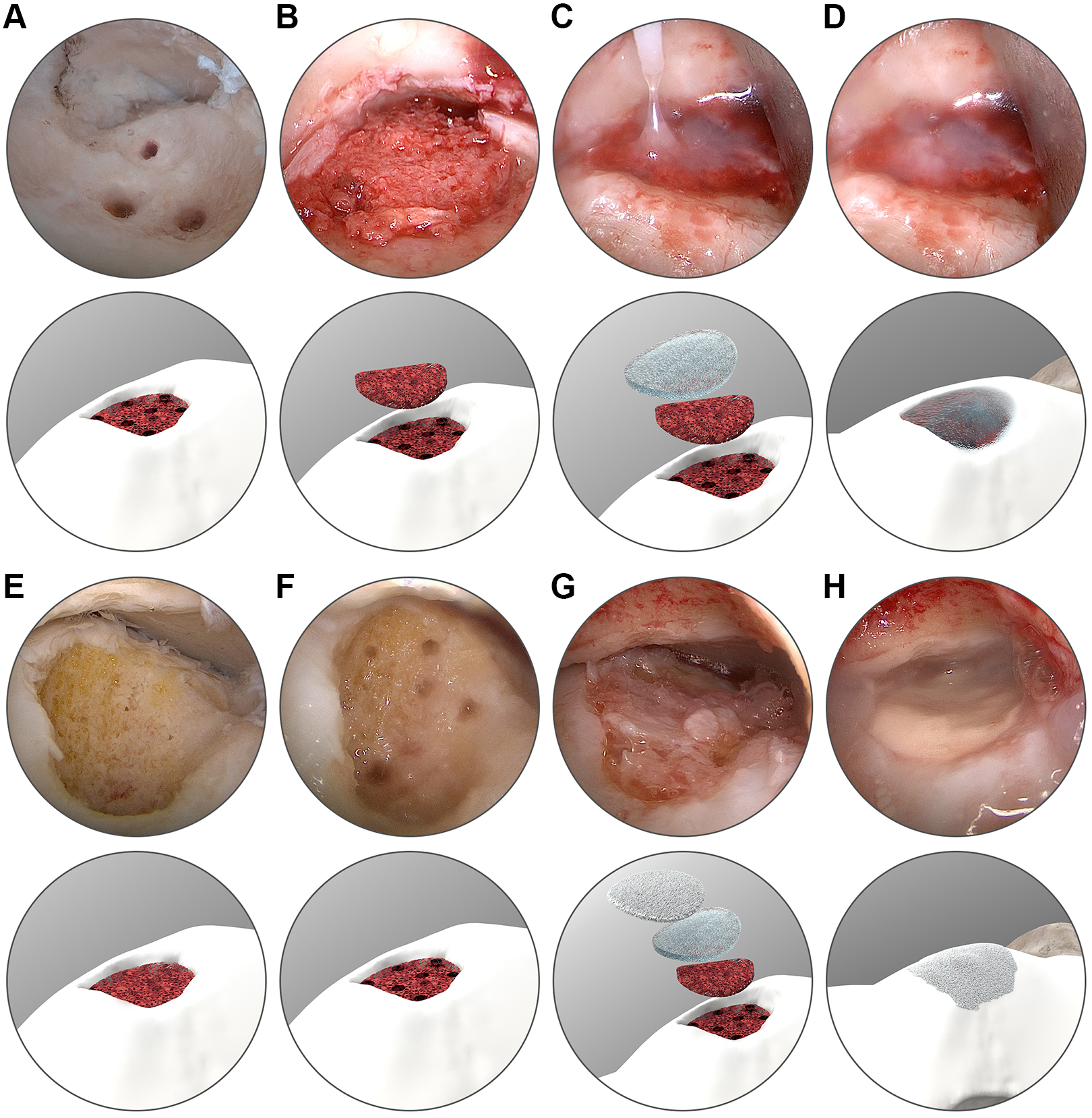
Steps of the surgical technique in the (A-D) bone grafting group and (E-H) bone grafting plus collagen scaffold group.
The procedure up to this stage was standard in both groups. In addition, for patients in group BG+S, a porcine collagen type I/III scaffold (Chondro-gide; Geistlich Pharma), which was prepared with an aluminum template according to the lesion size and shape, was placed onto the grafted region in a dry fashion through a suitable arthroscopic portal while the foot was held in maximum plantarflexion. If needed, osteoplasty was performed with a burr for the osteophytes in the anterior tibia to have a proper angle for the scaffold application. A fibrin-based sealant (Tisseel; Baxter International) was used as a fixation material for both groups to stabilize the bone grafts. It was placed on top of the bone graft in group BG and placed between the bone graft and scaffold in group BG+S. Neither group underwent calcaneal or malleolar osteotomy during the surgeries.
Postoperative Management
In the postoperative period, all patients in both groups were nonweightbearing with below-knee casts applied in a neutral ankle position for 4 weeks. Partial weightbearing with a range of motion walker (Aircast Walker, DJO Global, Vista, California) and physical therapy with passive range of motion exercises were allowed following cast removal. At 8 weeks postoperatively, patients were free to perform active range of motion exercises and full weightbearing. Return to intensive sport activities were allowed after at least 6 months postoperatively in all patients.
Statistical Analysis
The statistical analysis was performed with R Software (Version 4.1.2; The R Project for Statistical Computing) using the Rcmdr, Rallfun-v40, and car packages. Comparison of AOFAS and VAS among groups with respect to improvement in preoperative and postoperative scores was analyzed with robust methods for between-by-within design. 49 Group comparison for MOCART was performed with robust technique for comparing 2 independent groups. 48 0.2 Trimming and 1000-bootstrap replicates were preferred for robust estimation of means and confidence intervals (as per recommendations of the authors 48,49 ). The Cohen d was used to calculate effect sizes (0.2 = small; 0.5 = medium; 0.8 = large effect size). Correlation between MOCART, AOFAS and VAS were analyzed with robust measures of correlation (“type O” correlation). 50 The categorical variables between groups were compared by using the Pearson chi-square test. Values of P < .05 were considered to indicate statistical significance.
Results
There was no statistically significant difference between groups in demographic characteristics of the patients (age, sex), duration of symptoms, lesion characteristics (volume, side, location), or preoperative AOFAS and VAS scores. Both groups saw statistically significant pre- to postoperative improvement in AOFAS and VAS scores (P < .001 for all). However, the improvement in AOFAS and VAS scores was not statistically significantly different between groups (Table 2).
Preoperative and Postoperative AOFAS and VAS Scores a
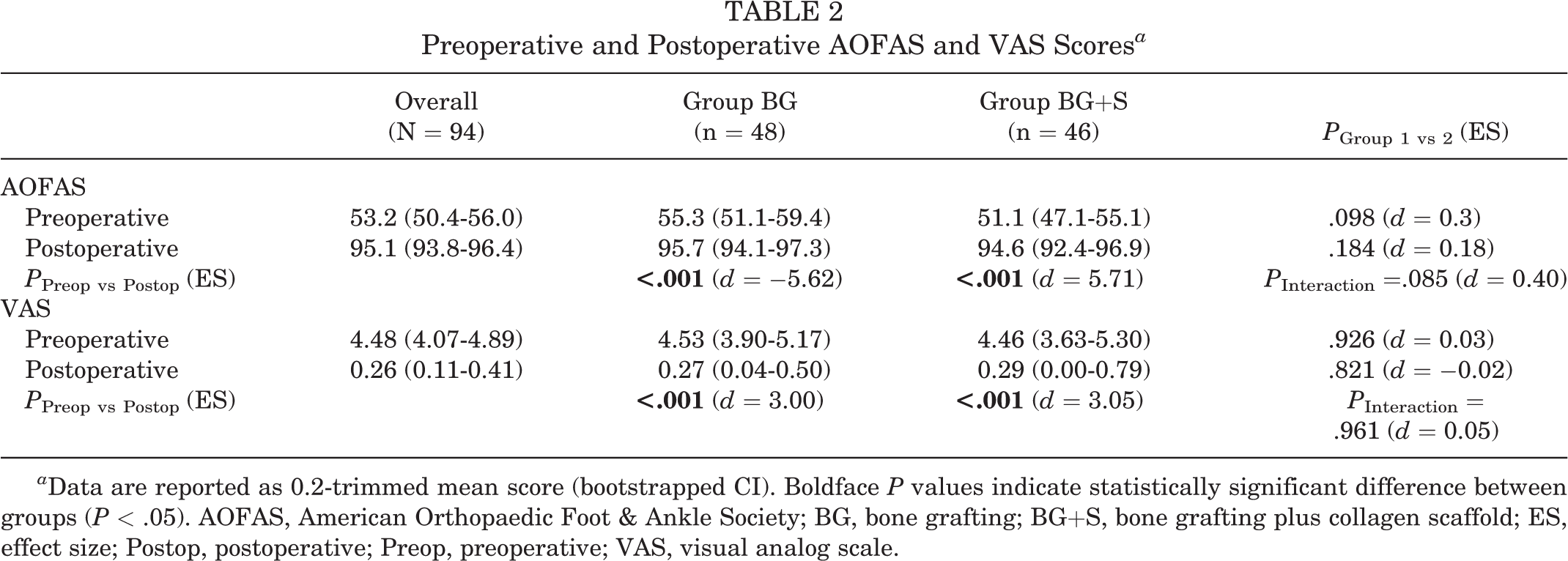
a Data are reported as 0.2-trimmed mean score (bootstrapped CI). Boldface P values indicate statistically significant difference between groups (P < .05). AOFAS, American Orthopaedic Foot & Ankle Society; BG, bone grafting; BG+S, bone grafting plus collagen scaffold; ES, effect size; Postop, postoperative; Preop, preoperative; VAS, visual analog scale.
The 0.2-trimmed mean MOCART score was 66.0 for group BG (bootstrapped CI, 63.9-68.0) and 61.4 for group BG+S (bootstrapped CI, 57.4-65.4). The difference was significant (P = .040), but the effect size was small (Cohen d = 0.47). Complete healing with or without hypertrophy was achieved in 42 (87.5%) patients in group BG and 38 (82.6%) patients in group BG+S. Complete healing with graft hypertrophy was achieved in 24 (50%) patients in group BG and 22 (47.8%) patients in group BG+S; this difference was not statistically significant. Details of MOCART items are described in Table 3.
MOCART Properties of the Study Groups a

a Data are reported as n (%). BG, bone grafting; BG+S, bone grafting plus collagen scaffold; MOCART, magnetic resonance observation of cartilage repair tissue.
There was a statistically significant positive correlation between MOCART and AOFAS scores (r = 68.7; P < .001) and a significant negative correlation between MOCART and VAS scores (r = −49.2; P < .001) (Figure 2).

Correlation of MOCART (magnetic resonance observation of cartilage repair tissue) scores with (A) American Orthopaedic Foot & Ankle Society (AOFAS) and (B) visual analog scale (VAS) pain scores.
There was no statistically significant difference in postoperative complications between the study groups. In group BG, 1 patient had a superficial skin infection at arthroscopic portals; the infection resolved with oral antibiotic therapy. One patient from the same group had developed synovial fistula at 1 of the arthroscopy portals and was treated with deep soft tissue reconstruction. In group BG+S, 2 patients had a superficial skin infection of an arthroscopic portal; the infection resolved with oral antibiotic therapy.
Discussion
The most important finding of the present study is that an all-arthroscopic surgical treatment of OLT, including debridement, microfracture, autologous bone graft application, and stabilization of the graft with fibrin glue, achieved similar outcomes compared with covering the bone graft with an additional collagen membrane, as there were no statistically significant difference in terms of clinical and radiological outcomes postoperatively between the BG and BG+S groups.
Several operative techniques have been described for the treatment of OLT in the literature, the main indication being failed conservative treatment. 8,29,32 Stimulating the bone marrow with microfracture was among the first techniques associated with reliable clinical outcomes in terms of pain and function; however, this technique turned out to have questionable results in OLT larger than 1.5 cm2. 5,27,52 Autologous chondrocyte implantation and matrix-induced autologous chondrocyte implantation procedures were then described to overcome such defects, although these have their own disadvantages, being 2-stage procedures. 32 Osteochondral autograft transfer (OAT) is another surgical technique described for the treatment of large defects; in OAT, grafts carrying type II collagen are harvested from the ankle or the knee and transferred to the defective area of the talus. However, OAT causes high rates of donor-site morbidity. 35,42 Osteochondral allograft transplantations have also been used in the surgical treatment of OLT; however, both are expensive and carry the risk of host-graft rejection. 10
In searching for a solution without these disadvantages, Benthien and Behrens 3 developed a single-step procedure called AMIC, described initially for the knee joint, which combined debridement, microfracture, and stabilization with collagen membrane scaffold. Wiewiorski et al 47 later applied this technique with an additional autologous bone grafting to a large focal osteochondral lesion of the talus for the first time via arthrotomy in a 21-year-old man and achieved excellent results at 1-year follow-up. Since then, various studies indicating the benefits of AMIC as a single-stage procedure with reduced donor-site morbidity have been published, especially in the treatment of patients with large (15 mm2) OLT. 1,2,46 However, there is still no consensus in the literature about which surgical procedure is superior to another in the treatment of these defects. 7,17 Furthermore, the original AMIC technique had its own disadvantages of being an open procedure, with most cases requiring an arthrotomy to have good exposure and successful restoration of the lesion. 40
Recently, Valderrabano et al 43 described an iliac crest cancellous graft–aided AMIC procedure for osteochondral lesions of the ankle joint with a minimum follow-up of 24 months. The rationale behind their novel modified AMIC technique was the talar lesions’ typically having concomitant large cystic osseous lesions; therefore, increasing the necessity of adding autologous cancellous bone grafts with rich mesenchymal stem cell ingredients to the existing AMIC procedure. In their study, both AOFAS and VAS scores had improved significantly in the postoperative period and they achieved full coverage of the lesion on postoperative MRI in 85% of patients, which was similar to our results. Although no complications were seen postoperatively, malleolar osteotomy had also been performed in 22 of their 26 cases. Because malleolar osteotomies have a morbidity of open surgical naturea and a probability of having malunion and nonunion; all-arthroscopic treatments have recently become popular. 40
In the search for a minimally invasive technique, Usuelli et al 40,41 recently developed an all-arthroscopic AMIC procedure for the surgical treatment of OLT to overcome the disadvantages of the existing open AMIC technique and having arthroscopic advantages of smaller incisions and quicker patient recovery. We had performed a similar technique for years, but we had difficulty finding an available collagen scaffold on the market due to health insurance–based issues. Therefore, we eventually began to perform the procedure by applying the autologous bone graft and stabilizing it with fibrin glue only, without an additional scaffold applied to the bone graft. The theory was that the fibrin glue would act as a scaffold with its organic fibrin-based nature. With the help of autologous cancellous bone grafts with rich mesenchymal stem cell ingredients, a healthy cartilage was created over the graft. We did not observe any major difference in this group when compared with lesions treated with an additional scaffold for stabilization, and this constituted the hypothesis of the current study. In addition, we preferred ipsilateral iliac crest as the source of cancellous bone, rather than calcaneal grafts as described in Usuelli et al 40,41 . Although it has a low morbidity of donor site, iliac crest has been considered to be the gold standard for harvesting autogenous bone grafts. 43
Several studies have been published about autogenous bone grafting for the treatment of OLT with different indications and surgical techniques. § Some of the authors preferred preserving the existing articular cartilage after grafting if it was healthy, 9,37 whereas others did not if it was degenerated or damaged. 14,26,43,46 According to a systematic review by Zengerink et al, 53 each technique has been reported with different success rates, varying from 41% to 93%. The main principle of the “grafting” concept remains intact, that is, to restore and provide the weightbearing profile of the talus. Therefore, the indication is generally based on the “depth” of the lesion, which points out the subchondral bone compromise. There have been different opinions in the literature about the amount of depth, indicating the need for bone grafting; 11,15 Giannini et al 36 created a classification system for OLT and underlined this concept clearly by giving a threshold size deeper than 5 mm as the minimum defect depth where grafting is needed. Kolker et al 22 reported that using autologous bone grafting alone without cartilage repair led to poor results in their series. They therefore did not recommend it as a primary treatment for OLT but instead stated that it could be used in combination with the other procedures. 22 The consensus statements on “Scaffold-Based Therapies,” developed at the 2017 International Consensus Meeting on Cartilage Repair of the Ankle, also agreed on this idea, as the use of bone grafting alone yields fibro-like instead of hyaline-like tissue. 36 This idea was the rationale behind the concept of using scaffolds to overlie and stabilize the bone graft in these procedures. But it is a well-known fact that native hyaline-like tissue could be expected only with autologous chondrocyte implantation. Collagen matrix over the bone graft could act only as a scaffold to achieve a better fibrocartilage. In the light of this, Kubosch et al 25 achieved satisfactory results in their study consisting of 17 patients who underwent an arthroscopy-assisted open procedure for OLT in the medial talus. The surgical procedure included debridement, microfracture, autologous cancellous bone grafting, application of porcine collagen I/III membrane, and stabilization with fibrin glue, which is similar to the technique used in our BG+S group.
As collagen is the natural component of skeletal tissues, collagen-based scaffolds are thought to allow both stimulation of matrix formation for cartilage repair and reduction of graft failure by improving the graft stabilization. 16,31 In addition, with the evolving bioengineering industry, 3-dimensional scaffolds have been developed to limit the complications of autologous chondrocyte implantation and AMIC techniques, such as graft hypertrophy. 6,23,24,44 Although there have been encouraging results on the use of scaffold-based treatments, there is still a lack of data and low level of evidence, which brings the need for further prospective studies to confirm the long-term benefits of these products. 18,38,44,51 In our study, we found no statistically significant difference between the BG and BG+S groups in terms of degree of defect repair and filling of the defect, according to the MOCART scores (the rates of hypertrophic repair were similar).
On the other hand, fibrin sealants have been used widely for decades as an adhesive for stabilizing perichondral grafts and promoting chondrocyte proliferation. 19,21 We are aware that using fibrin sealants in combination with other collagen-based scaffolds is preferred in the literature because of the low mechanical resistance and rapid biodegradability of fibrin, thus limiting its application as a tissue-engineering scaffold alone. 33,34 Although there are studies in the literature stating that it is unsuitable for the use as a scaffold in treating osteochondral defects, recent studies have given promising results, by focusing on the effects of fibrin sealants on chondrocyte behaviors in detail. 4,20 In an ex vivo study by Filardo et al, 12 fibrin glue was found to significantly improve the stability and integrity of the scaffolds, irrespective of the lesion location or scaffold type. Furthermore, it was discussed that the fibrin glue may favor implant integration not only mechanically, but also biologically, by representing a scaffold itself to host cells and promote tissue formation. While the efficacy and outcomes of using these products alone as a scaffold or in combination with other tissue-engineering products is still a matter of controversy, there is increasing evidence regarding fibrin sealants themselves inducing a chemoattractive response in chondrocytes and aggravating chondrogenesis. 12,19,20,34 In the light of this know-how, we speculated that the use of fibrin sealant alone as a scaffold, applied directly onto a source of mesenchymal stem cells, should be investigated in further in vitro and in vivo studies.
Limitations
There are several limitations to this study. First of all, the retrospective design precluded evaluation of some of the properties of both patients and lesions. As lesion “depth” is an important parameter indicating “grafting,” it would be ideal if, in addition to determining the total volume of the lesion, the depth of the defect was addressed separately perioperatively after debridement of damaged tissue. However, it can be assumed to be at least 5 mm (the threshold value for the indication of autologous bone grafting). Some demographic properties of the patients, such as body mass index or smoking habits, could not be identified from the registry data either, and there is debate surrounding whether these properties affect the healing of talar articular cartilage significantly or not. Cases with cystic components, which are thought to be the ideal indication for bone grafting, were also not investigated in detail in this study. The main reason behind this omission was that we believe that bone grafting may not be indicated only in lesions with cystic components. The real problem in OLT may not be only a cartilage issue but also a bony problem due to circulation damage to the bone and subsequent necrosis. Therefore, bone grafting could also be considered in these lesions, even if not accompanied by a significant cystic component. Although there was no statistically significant difference in terms of the number of cystic lesions in both groups that may interfere with the clinical results, it would have been ideal if all properties of these lesions, including depth and volume, were added to the study and compared between groups to decrease possible biases. Further prospectively designed clinical trials or multicenter research studies would enlighten these properties and the precise necessity of using scaffolds in such lesions in more detail.
Last, the average follow-up time was significantly longer in group BG+S. Although we do not believe that this difference would have affected the outcomes at all (as the mean follow-up time was long enough [69.3 ± 20.7 months] for all study patients), it may theoretically have a negative effect on MRI scans and clinical outcomes of group BG+S. Second-look arthroscopies or biopsies would emphasize the outcomes for both groups more clearly; however, we were unable to undertake second invasive interventions in our study, which may be a further study design in the future.
Conclusion
All-arthroscopic surgical treatment of OLT, including debridement, microfracture, autologous bone graft application, and stabilization of the graft with fibrin glue, achieved similar clinical and radiological postoperative outcomes compared with covering the bone graft with an additional collagen membrane. Using autologous bone graft for stimulation and restoration of osteochondral lesion without any need for an additional collagen membrane is the advantage of this novel technique. This study highlights once again that OLT is primarily a bone lesion and that cartilage lesion is a concomitant problem. Treatment of the bone lesion of the talus might be the ultimate goal to obtain successful outcomes, in which case using a collagen scaffold besides grafting may not affect clinical and radiological outcomes.
Footnotes
Notes
Final revision submitted October 13, 2022; accepted October 21, 2022.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Acibadem University (ref No. 2022-07/06).