
Abstract
Background:
Motion of the pelvis and trunk during baseball pitching is associated with increased upper extremity (UE) kinetics. Increased kinetics on the UE may lead to throwing-arm pain in youth pitchers. Limited biomechanical comparisons have been conducted on youth pitchers with and without throwing-arm pain to identify mechanical risk factors associated with pain.
Purpose:
To examine trunk and pelvic kinematics in youth baseball pitchers with and without UE pain.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A total of 26 male youth baseball pitchers (mean age, 12.7 ± 1.5 years; mean height, 162.2 ± 12.9 cm; mean weight, 52.6 ± 13.1 kg) were recruited to participate. An electromagnetic tracking system was used to obtain kinematic data during the fastball pitch. Data from a health history questionnaire was examined. Participants who answered “yes” to experiencing pain and who selected a region on their UE as the pain location were placed into the UE pain group. Participants who responded “no” to experiencing pain were placed into the pain-free group. We compared between-group differences in trunk rotation, flexion, and lateral flexion; pelvic rotation, anteroposterior tilt, and lateral tilt; and hip-shoulder separation from peak knee height to ball release of the baseball pitch using 1-dimensional statistical parametric mapping with an alpha level set at .05.
Results:
No statistically significant differences were observed between the UE pain and pain-free groups in the 7 trunk and pelvic kinematics analyzed from peak knee height to ball release (P > .05).
Conclusion:
Trunk and pelvic kinematics during the pitching motion did not differ between pain and pain-free groups of youth baseball pitchers.
Up to 50% of youth baseball pitchers experience upper extremity (UE) pain throughout their competitive season. 22,24,43,48 Furthermore, an alarming 46% of players were encouraged to continue playing despite the presence of arm pain. 24 In youth baseball pitchers, physical and developmental changes, 47 workload (ie, pitch volume, high effort throws, exceeding pitch counts), and limited rest days have been associated with UE pain and injury susceptibility. 9,10,12,23,51 To date, limited biomechanical comparisons have been conducted in this population to examine pitching mechanics associated with pain, despite the high prevalence of pain and injury among those completing this highly dynamic, repetitive, and explosive task.
During pitching, the relationship between kinematics and kinetics is influenced by the mechanism of dynamic coupling in which the position of segments affects joint torques. 58 A study by Hirashima et al 17 demonstrated that proximal joint segments were accelerated primarily by their own joint torques while distal segments were accelerated by velocity-dependent torques of proximal segments generated earlier in the pitch.
Work by Naito et al 31 demonstrated that maximal arm velocity during pitching was largely attributed to nonmuscular (passive-motion dependent) effects of increasing angular velocities of the chest, elbow, and wrist, accompanied by muscular torque effects of shoulder internal rotation. These findings corroborate that trunk and pelvic segments play a key role in creating and funneling kinetic energy into the throwing arm. 1,31
The trunk and pelvis rotate mostly about the vertical axis which elicits the lowest rotational inertial resistance. 8 Further, the trunk comprises approximately half of the body’s total mass. 1 These aspects enable the trunk to be a main contributor of momentum to the throwing arm. 1,2,44,54 In high school pitchers, improper trunk rotation sequences defined by peak pelvic rotation velocity occurring after peak upper torso rotation velocity increased proximal-end upper arm distraction forces. 37 Findings from a previous study suggest that high-school pitchers do not effectively use forces generated by the rotation of their trunk and pelvis compared with professional pitchers. 21 Compared with professional pitchers, high-school pitchers displayed less pelvic rotation at events of maximal knee height and hand separation as well as less trunk rotation across all pitch phases. When assessing the kinetics between these groups, normalized elbow valgus torque at maximal shoulder external rotation was greater in high school pitchers, and pitch velocity for high school pitchers was related to greater absolute elbow valgus torque. Conversely, in professional pitchers, absolute elbow valgus torque was not related to pitch velocity and inverse relationships were found between absolute elbow valgus torque and upper trunk and pelvic rotation. 21 As such, effective use of the trunk and pelvis in the transverse plane is an important component in pitching that can contribute to kinetics experienced on the throwing arm that may play a role in the presence of pain.
Previous studies have reported that excessive contralateral trunk lean during pitching resulted in greater elbow proximal force and varus moments (external valgus) as well as shoulder proximal force and internal rotation moments. 36,45 Another study reported lateral flexion velocities were associated with peak shoulder-compressive forces and peak internal rotation net joint moments in youth pitchers. 13 Furthermore, increased forward trunk lean at ball release (BR) was shown to increase elbow varus moments (external valgus) and shoulder abduction net joint moments. 13,28,44 In youth pitchers, increased forward trunk flexion velocities before BR were related to shoulder abduction net joint moments and compressive forces. 13 Therefore, a comparison study between pain and pain-free groups of pitchers using time-series data may be useful in detecting mechanical differences and for examining kinematic patterns that may be associated with pain. 6,15,25,28
Although research has identified pitching-related injury risk factors in youth baseball players, 12,22,23,29,30,35 the factors associated with these injuries, specifically trunk and pelvic kinematics when throwing with pain, are not well understood. 14,18,42 An improved understanding of trunk and pelvic mechanics during the pitching motion associated with UE pain in youth baseball pitchers would be beneficial in determining modifiable-risk factors in youth pitchers. Improper motion of these segments may lead to increased kinetics on the UE and result in various soft tissue injuries. 40
The aims of this study were to compare trunk and pelvic kinematics between groups of youth baseball pitchers with and without UE pain using timeseries data. We hypothesized that pitchers reporting self-perceived UE pain would display 1 or more of the following kinematics: decreased trunk rotation toward home plate early in the pitching motion, decreased levels of hip-shoulder separation, increased trunk lateral flexion away from the pitching arm, and increased trunk flexion near BR.
Methods
Participants
A total of 26 male youth baseball pitchers (mean age, 12.7 ± 1.5 years; mean height, 162.2 ± 12.9 cm; mean weight, 52.6 ± 13.1 kg) between the ages of 10 and 15 years were selected from an internal database for this retrospective study. Inclusion criterion required participants to be competing actively on a team roster as a pitcher during the time of data collection. In addition, they had to be surgery- and injury-free for 6 months before participation. Injury was defined as being diagnosed by a physician or athletic trainer resulting in any time loss from practice or competition. The institutional review board of Auburn University approved all testing protocols, and written informed parental consent and assent from the participant were obtained before study participation.
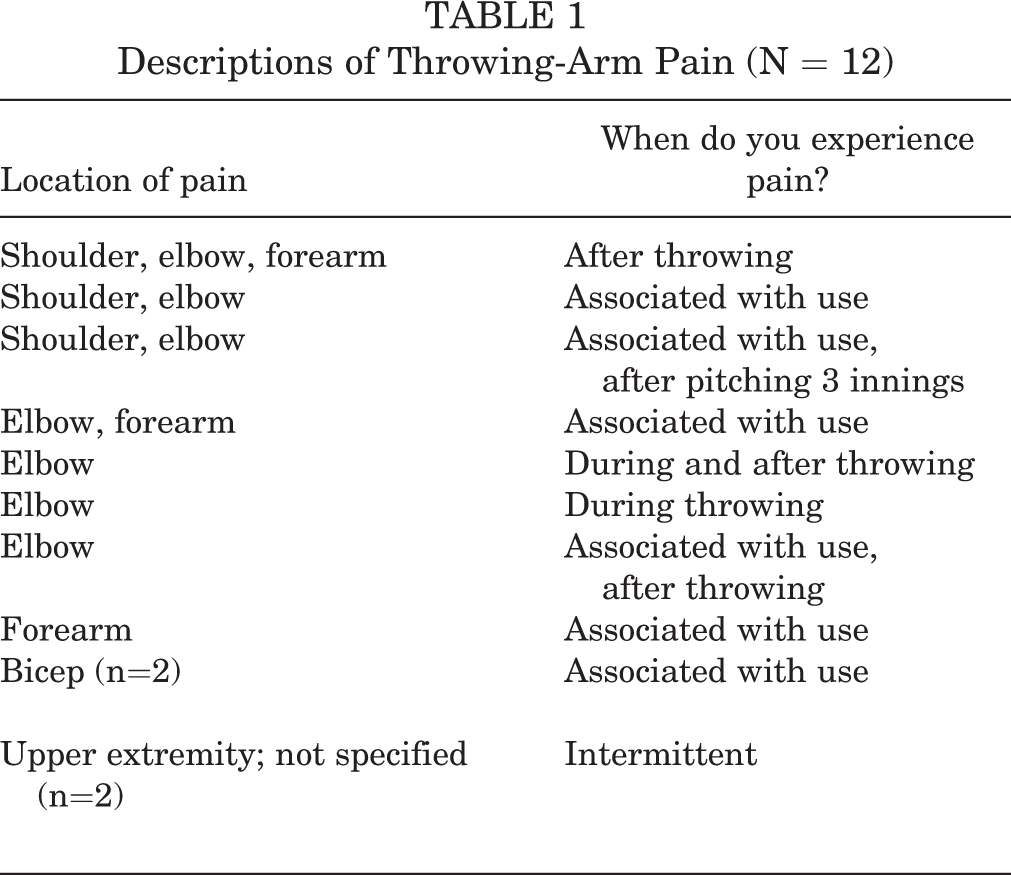
A questionnaire was used to determine the occurrence of pain in pitchers. Participants were asked, “Do you currently experience any pain/discomfort in your upper extremity, specifically your throwing side?” Participants were placed into 2 groups based on the yes/no response: those currently experiencing UE pain and those who were not. Currently experiencing pain included reported pain before, during, and/or after pitching. Those who answered “yes” were then asked to select the body area where they were currently experiencing pain. All participants who answered “yes” and selected any area of their arm, elbow, or shoulder were assigned to the pain group. Therefore, the UE pain group included pitchers with various locations of pain along the UE. Chalmers et al 6 observed a significantly higher percentage of pitchers with current pitching-related discomfort in those with a history of pitching-related shoulder or elbow injury compared with uninjured pitchers. Table 1 displays the locations and types of experienced pain that were reported. Those who answered “no” were deemed pain-free. The pain group was then matched to a group of pitchers of similar demographics who were pain-free.
Descriptions of Throwing-Arm Pain (N = 12)
Procedures
Kinematic data were collected using an electromagnetic tracking system (trakSTAR; Ascension Technologies, Inc) synced with biomechanics analysis software (The MotionMonitor; Innovative Sports Training). These data for 18 of the included participants from the database were collected at 100 Hz (2013-2017) and for 8 participants were collected at 240 Hz (2017-2019). The inclusion of participants whose data were captured using the higher frequency was to balance group size, as all 8 participants with data collected at 240 Hz were in the pain-free group.
For motion capture, sensors were attached to the following locations: (1) posterior aspect of the trunk at the first thoracic vertebra spinous process; (2) posterior aspect of the pelvis at the first sacral vertebra; (3-4) bilaterally, on the flat, broad portion of the acromion on the scapula; (5-6) lateral aspect of the bilateral upper arm at the deltoid tuberosity; (7-8) posterior aspect of the bilateral distal forearm; (9) dorsal aspect of the throwing hand, centered on the third metacarpal; (10-11) lateral aspect of the bilateral upper leg, centered between the greater trochanter and the lateral condyle of the knee; (12-13) lateral aspect of bilateral lower leg, centered between the head of the fibula and lateral malleolus; and (14) dorsal aspect of the foot contralateral to pitching arm centered on the second metatarsal. 19,53 A 15th movable sensor attached to a plastic stylus was used for the digitization of bony landmarks. 33,34,56,57
Using a digitization method, a link segment model was developed. Joint centers were determined by digitizing a joint’s medial and lateral aspects then calculating the midpoint between those 2 points. 33,34,56,57 A rotation method was used to estimate the joint centers of the shoulder and hips. 16,50 Raw data regarding sensor position and orientation were transformed to a locally based coordinate system. For the world axis, the y-axis represented the vertical direction. Anterior to the y-axis in the direction of movement was the positive x-axis; orthogonal and to the right of the xy-axes was the positive z-axis. Position and orientation of the body segments were obtained using Euler angle sequences that were consistent with the International Society of Biomechanics standards and joint conventions. 56,57 Specifically, the zx′y″ sequence described trunk and pelvic motion relative to the world axis. All raw data were independently filtered along each global axis using a fourth-order Butterworth filter with a cutoff frequency of 13.4 Hz. 33,34,55 All data were time-stamped through The MotionMonitor(Innovative Sports Training) and passively synchronized using a data acquisition board. Pitch speed was measured using a calibrated radar gun (StalkerPro II; Stalker Radar).
After sensor placement and digitization, participants were allotted unlimited time to complete their pregame warm-up and become familiar with all testing procedures. For testing, each participant threw 3 fastballs for a strike to a catcher at regulation distance. The fastest pitch thrown for a strike was analyzed. A biomechanical comparison was performed on the pitching motion from peak knee height (PKH) to BR. This includes the push-off, arm cocking, and acceleration phases (Figure 1), encompassing the events of PKH, stride foot contact, maximal shoulder external rotation (MER), and BR. PKH was defined as the maximum vertical displacement of the stride-leg knee in the vertical direction. Stride foot contact was measured by the first change in ground reaction force greater than 20 N using a nonconductive force plate embedded into the pitching platform (Bertec 4060 NC sampled at 1200 Hz; Bertec Corp). BR was measured as the quantified time point halfway between MER and maximal shoulder internal rotation. 4,5,52 MER and maximal shoulder internal rotation were determined based on the rotation of the upper arm segment about the long axis defined relative to the thorax using a yx′y" Euler rotation sequence. 54,57 Data were time-normalized to 100% of the time between PKH and BR and analyzed using 1-dimensional statistical parametric mapping (SPM) in the open-source software package SPM1d. 20,38,39 Hip-shoulder separation was determined by subtracting trunk rotation from pelvic rotation in the transverse plane. The kinematic variables analyzed are illustrated in Figure 2.

Pitching motion analyzed peak knee height (PKH) to ball release (BR). FC, foot contact; MER, maximal shoulder external rotation.

Trunk and pelvic variables: (A) pelvic and trunk rotation, (B) trunk lateral flexion, (C) trunk flexion/extension, (D) hip-shoulder separation, (E) pelvic lateral tilt, and (F) pelvic anteroposterior tilt.
Statistical Analysis
A Shapiro-Wilk test of normality was used to assess normality of demographics. Subsequently,a Mann-Whitney U test was performed to evaluate differences in age, height, weight, and pitch speed between pain and pain-free groups. Statistical parametric mapping was used to assess trunk and pelvic kinematic differences from PKH to BR during the pitch. Seven independent-samples SPM(t) tests were performed to contrast trunk rotation, flexion, and lateral flexion; pelvic rotation, anteroposterior tilt, and lateral tilt; and hip-shoulder separation between groups using an alpha level set at .05. Descriptive statistics were processed using SPSS (Version 27.0 [released 2019]; IBM SPSS Statistics for Windows), and SPM analyses and all kinematic data were processed using a customized MATLAB script (MATLAB R2021A; MathWorks).
Due to participant data’s being pulled from a database, we were unable to perform an a priori power analysis, which is a method preferred over post hoc. 32 We chose to calculate for transparency but encourage the reader to interpret the analysis with caution. This is a limitation to this study; however, achieving a large sample size of pitchers pitching with pain is difficult, and we determined the data should still be reported similar to a previous study analyzing history of injury with kinematic outcomes. 7 Based on our sample of 12 participants in the pain group, power was calculated at β (pelvic rotation), 0.60; β (trunk rotation), 0.54; β (trunk flexion), 0.95; β (trunk lateral flexion), 0.33; β (hip-shoulder separation), 0.93; β (pelvic lateral tilt), 0.74; and β (pelvic anteroposterior tilt), 0.22.
Results
A total of 12 participants satisfied the inclusion criteria and were included in the pain group; 14 participants were included in the pain-free group. Descriptive statistics for demographic variables are presented in Table 2. All demographic data were distributed normally apart from height of the no-pain group (W = .863; P = .034). Based on this outcome, a nonparametric Mann-Whitney U test was used to determine differences in demographics. There were no significant differences between the pain and pain-free groups in age (U = 60.50; n 1 = 14; n 2 = 12; P = .217), height (U = 70.00; n 1 = 14; n 2 = 12; P = .471), or weight (U = 72.00; n 1 = 14; n 2 = 12; P = .537). In addition, pitch speeds did not differ between groups (U = 60.50; n 1 = 14; n 2 = 12; P = .643).
Participant Demographics a

a Data are reported as mean ± SD.
The SPM analysis revealed no statistically significant differences in trunk rotation, flexion, and lateral flexion between the pain and pain-free groups from the time-normalized comparisons of PKH to BR. Furthermore, no statistically significant differences were found in pelvic rotation, lateral tilt, and anteroposterior tilt, and hip-shoulder separation between the pain and no-pain groups. Time-normalized kinematic comparisons from PKH to BR, in addition to the SPM of each test, are presented in Figures 3 and 4 on the left- and right-hand sides of the figures, respectively. The thick black lines on the SPM visualization (right) in Figures 3 and 4 indicate a t statistic continuum for the duration of the pitch; the red hashed line indicates the alpha-based critical threshold of the t statistic. A test is considered significant when the t-statistic crosses the alpha threshold line. The x coordinate of where significance occurs corresponds to the normalized time point where differences occurred.

Trunk-related time-normalized comparisons between groups (left) and statistical parametric mapping (SPM) visualizations (right). (A) Trunk rotation: (-) toward third base, (+) toward first base; (B) trunk lateral flexion: (+) toward throwing-arm side, (-) away from throwing-arm side; and (C) trunk: (-) flexion, (+) extension. BR, ball release; PKH, peak knee height. t*: significant t value. Red hashed line: significant t statistic thresholds 0-100% of pitch.

Pelvis-related time-normalized comparisons between groups (left); (A) pelvic rotation: (-) toward third base, (+) toward first base; (B) pelvic lateral tilt: (+) toward stance leg, (-) toward stride leg; (C) pelvic anteroposterior (AP) tilt: (-) anterior pelvic tilt, (+) posterior pelvic tilt; and (D) hip-shoulder separation: pelvic rotation minus trunk rotation. Statistical parametric mapping visualizations (right). BR, ball release; PKH, peak knee height. t*: significant t value. Red hashed line: significant t statistic thresholds 0-100% of pitch. Thick black lines: t statistic for kinematic data 0-100% of pitch.
Discussion
This study found no significant differences in trunk and pelvic kinematics in youth pitchers with and without UE pain. Therefore, we rejected our hypothesis, which suspected trunk and pelvic mechanics to differ between groups. Considering the role trunk positioning plays on UE forces and how increased forces can contribute to arm pain, this was an unexpected result. Lack of significant differences in trunk and pelvic biomechanics between UE pain and pain-free groups suggests that other influences may affect the prevalence of UE pain within youth baseball pitchers.
When comparing healthy pitchers with those with a history of injury/surgery, Fleisig et al 13 reported no differences in trunk kinematics in high school and college pitchers shortly after ulnar collateral ligament repair (n = 33) compared with healthy controls (n = 33), though differences in elbow extension, elbow extension velocity, and shoulder internal rotation velocity were observed between groups. Further, in a study comparing noninjured pitchers with pitchers who previously had a type of core injury, no differences in pelvic or trunk kinematics were observed, though increased elbow flexion at BR and normalized elbow forces were found in those with a previous core injury type. 28 The authors concluded that compensations up the chain at the throwing arm may be occurring. Manzi et al 28 also reported that pitchers with increased elbow flexion at BR were more likely to have a history of elbow injury. Accordingly, distal segment biomechanics may influence the presence of arm pain to a greater extent than proximal segment biomechanics. 3 It is noted, however, that history of injury/surgery and the presence of arm pain may not be correlated.
Research has shown that youth baseball pitchers may struggle to optimally sequence their trunk and pelvis compared with elite pitchers. 1,21 It has also been reported that less elite and younger pitchers typically demonstrate greater variability in pitching mechanics. 11 Previous studies have reported greater variation in other kinematic variables not used in the current study outside of forward trunk tilt at BR, 9,11 and variation in kinematics has also been reported with relation to pitch speed. 46 In the present study, pitch speeds were not significantly different between groups (Table 2). Proposed aspects of pitch variance in youth pitchers present some challenges in determining group differences. The influence of pitch and/or group variance combined with the limited sample size, in addition to dependence on distal kinetic chain components, might have contributed to the present null findings among this sample, despite the importance of trunk and pelvic positioning on pitching kinetics and performance. The current study used only the fastest pitched fastball from each participant. The fastball is often the first pitch youth pitchers acquire and therefore have more experience throwing. In addition, participants had unlimited time to warm up and familiarize themselves with the laboratory environment, and pitches analyzed were thrown for strikes. Still, with these aspects in mind, strategies for assessing mechanical differences in relation to injury prevention should consider unique kinematic profiles associated with the level of play. 41
A benefit of using SPM analysis to compare groups is that it provides temporal specificity of when differences in kinematics occur, which can be visualized from the time-series plots. This can offer insight into pitch timing, which is the time spent between peak angular velocities achieved by segments across the kinetic chain. 26,49 It has been reported that pitchers with decreased time in the early phases of the pitching motion (ie, foot contact to peak pelvic angular velocity) had increased shoulder joint forces. 2,26,49 In contrast, increased time spent in the late phases correlated with decreased shoulder forces. 1 One study observed that elite-level pitchers rotated their trunks later in the pitching cycle compared with lower-skilled pitchers. 1 Aguinaldo and Escamilla 2 reported that the timing of trunk motion and flow of mechanical energy from the trunk to the upper arm was found to predict maximum elbow valgus torque. Another study suggested not only the importance of timing but the rate of trunk rotation played a significant role in throwing shoulder kinematics, 34 a potential basis for the onset of pain. Chalmers et al 7 reported that peak trunk rotation was reached later in the pitch for those who underwent superior labrum anterior to posterior repair compared with control and biceps tendinosis repair groups in collegiate-level pitchers or above. Another study reported less trunk rotation at foot contact in professional pitchers who underwent a superior labrum anterior to posterior tear, but no other kinematic differences were observed. 27 Although pain is linked to, or may precede, injury, one should use caution when comparing self-reported pain with diagnosed injury. The current study observed no significant differences in trunk or pelvic kinematics between pain and pain-free groups. When youth are developing pitching mechanics, pelvic and trunk mechanics should be emphasized; although when arm pain is reported, then assessing distal segment kinematics and kinetics, pitching workloads, and continuous monitoring of arm health may be appropriate action steps in determining causative mechanisms and for reducing the prevalence of arm pain.
Previous studies have reported that increased lateral trunk lean away from the pitching arm resulted in higher forces on the UE, although it also resulted in higher pitch speeds. 36,45 In the current study, pitch speeds were not significantly different between groups (pain, 55.9 ± 9.48 mph; pain-free, 54.8 ± 8.32 mph), which may justify the lack of frontal plane differences in trunk mechanics. Likewise, the lack of sagittal plane differences observed in this study may also be related to similar pitching ability among the pain and pain-free groups as indicated by similar pitch speeds. 25 Therefore, differences in pelvic and trunk mechanics may be linked more to performance/velocity than the result of arm pain. Future biomechanical research comparing pain and pain-free groups of pitchers should include subgrouping locations of pain, longitudinally collected data such as changes in player demographics, pitching workloads, pitch types, variance in kinematics, and mechanical variables of the throwing arm in addition to the variables used in this study. 6 Furthermore, questionnaires assessing throwing-arm function and the extent of pain may help compare mechanics across various levels of pain or arm function capacities.
Limitations
The limitations of this study include a small sample size of youth baseball pitchers reporting pain. The lack of significant differences in these comparisons may be due to a lack of sufficient statistical power. Therefore, findings may need to be interpreted with some caution. With relatively smaller sample sizes due to the availability of pain data, the present study used group comparisons across the pitching motion (0%-100%), which was an approach chosen to make detailed comparisons of each segment’s pattern of motion. Moreover, this study only examined a pitcher’s fastest recorded fastball during data collection and did not assess within-pitcher variance. Other potential limitations include the age range of participants in this study. Future research should examine pitching biomechanics within more homogeneous groups using more discrete age ranges. Furthermore, pain was self-reported and measured only as a binary variable (currently experiencing or not experiencing throwing-arm pain) and included a wide range of UE pain locations. When assessing kinematics, this study used trials collected at a sampling rate of 100 Hz. However, this study focused on relatively slower motions of the pelvis and trunk, therefore we feel sufficient data were obtained for this analysis. Future analyses should assess throwing-arm kinematics and kinetics, specific locations of reported pain, and use of different pitch types.
Conclusion
The findings of this study indicate that youth pitchers may not be at risk of reporting throwing-arm pain based solely on motions of the trunk and pelvis during pitching. Although motions of the trunk and pelvis may be associated with increased forces on the throwing arm that can lead to injury, when throwing-arm pain is reported, additional mechanics such as those of the UE should also be considered alongside workload and nonmodifiable risk factors.
Footnotes
Final revision submitted September 9, 2022; accepted September 26, 2022.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Auburn University (protocol No. 18-121 EP 1803).