
Abstract
Background:
It has previously been speculated that baseball pitchers who display excessive forearm pronation at foot contact (FC) have a higher propensity toward ulnar collateral ligament injury and subsequent surgery.
Purpose:
To evaluate the association between degree of forearm pronation/supination at FC and throwing arm kinetics in high school and professional pitchers, at both the individual (intrapitcher) and the group (interpitcher) level.
Study Design:
Descriptive laboratory study.
Methods:
High school (n = 41) and professional (n = 196) pitchers threw 8 to 12 fastballs while being assessed with a 3-dimensional motion-capture system (480 Hz). Pitchers at each playing level were divided into a supination or pronation subgroup depending on degree of forearm pronation at FC. Regression models were built to observe the relationship between forearm pronation at FC and kinetic and kinematic parameters of interest.
Results:
At both the individual and the group level of high school and professional pitchers, there was no significant correlation between forearm pronation at FC and elbow varus torque (P min = .21). For every 10° increase in forearm pronation at FC in the individual high school pitcher, elbow flexion at FC decreased by 5°, whereas maximum elbow extension velocity was achieved 0.6% later in the pitch. In addition, elbow medial force increased by 4.1 N and elbow varus torque increased by 0.8 N·m for every 10° increase in forearm supination at FC. For every 10° increase in forearm supination in the individual professional pitcher, ball velocity increased by 0.5 m/s, shoulder external rotation at FC decreased by 11°, and elbow medial force decreased by 5.5 N.
Conclusion:
Supination- or pronation-predominant forearm motion during the pitch did not significantly differ between playing levels. Excessive forearm pronation at FC was not a significant risk factor for increased throwing arm kinetics for high school or professional pitchers. There was a weak positive association between forearm supination at FC and elbow varus torque in the individual high school pitcher. Ultimately, coaches and pitchers may be better served by redirecting their focus to other mechanical aspects of the pitch that may have stronger associations with injury risk implications as well as performance.
Injury rates have increased steadily over the past 20 years in professional baseball pitchers. 4,28 In Major League Baseball (MLB), pitchers bear a disproportionate percentage of these injuries, accounting for 62.4% of all days spent on the injured list. Approximately 26.3% of these injuries affect the throwing elbow, resulting in an average of 74 days of lost play per year in the MLB. 28 In 2015, Conte et al 5 observed that 25% of major league and 15% of minor league pitchers have undergone surgical ulnar collateral ligament (UCL) reconstruction (colloquially known as “Tommy John” surgery) each year. Partial UCL tears that can be managed conservatively still require 3 to 4 months of rehabilitation, whereas reconstruction rehabilitation can take between 12 and 18 months before return to play. 2 A return to presurgical level of performance is not guaranteed: studies estimate that 77% to 90% of MLB pitchers do return to play with 80% returning to a prior level of performance or better. 1,2,8,21,23,27 From 2004 to 2014, MLB pitchers who underwent UCL reconstruction missed an average of 180 days of the regular season, and cost of recovery amounted to more than US$2 million per pitcher. 21
Given the high incidence, complications, and costs of UCL tears, injury prevention is a high priority among players and coaches. Pre-established risk factors for professional pitchers include a high percentage of fastballs thrown (above 48%), high peak ball velocity (above 95.7 mph [154 kph]), and fewer days between outings. 2,3,12 Biomechanical researchers have sought to identify full-body kinematic and throwing arm kinetic parameters as surrogates for injury risk using advancements in motion-analysis technology to potentially identify risk factors. 4,11– 13
One factor that has been debated in coaching circles is the degree of forearm pronation at the time of foot contact (FC) during a pitch. Some coaching staff have suggested pitchers who display excessive forearm pronation may have a higher propensity toward increased load of the UCL and subsequent injury. 22 This speculation may originate from the fact that the common flexor origin of the elbow originates on the medial epicondyle. With excessive pronation fatiguing this muscle mass at the medial side of the elbow with repetitive use, pitchers and coaches may speculate that this is a risk factor for UCL injury. In addition, FC is at times referred to as the start of the “power position,” where pitchers are most receptive to implementation of changes in the pitching motion 11 with potential major implications for subsequent portions of the pitch. This extreme forearm pronation in effect causes the baseball to face second base, away from home plate, during the early cocking phase. For reference, a less pronated forearm would result in a baseball facing closer to short-stop for a right-handed pitcher, as is recommended by USA Baseball. 33
One piece of evidence that supports the theory comes from the relationship between fastball kinematics and UCL reconstruction. Pitchers throwing a fastball have more forearm pronation during the cocking phase than those throwing a curveball. 11 –13 In addition, pitchers with increased fastball count have a higher incidence of UCL injury, which potentially could stem from this increased forearm pronation or from twisting motion. Solomito et al 33 found that at FC, the forearm was pronated 16° on average during a fastball, compared with a 2° supination of the forearm during a curveball. They also observed that torque about the elbow was significantly higher for fastballs compared with curveballs (75.2 vs 70.4 N·m, respectively). Still to date, no group has evaluated forearm pronation at FC as a potential correlate with throwing arm kinetics. Although Solomito et al observed an association between forearm pronation torque at maximum elbow extension and elbow varus torque in a cohort of collegiate pitchers, this analysis did not consider the time of FC, which has traditionally been the moment of question for excessive forearm pronation. This evaluation in a distinctly collegiate cohort confined the applicability of its findings to other playing levels, while also limiting its analysis to “between pitchers” rather than analyzing how an individual pitcher’s change in forearm pronation angle affects throwing arm kinetics. Last, this study only evaluated 1 elbow kinetic–-elbow varus torque–-not considering other directional forces of strain about the elbow.
Considering the lack of available data, the purpose of the current study was to compare forearm motion throughout the pitching motion between high school and professional pitchers and characterize kinematic and kinetic parameters for subgroups of pitchers delineated by degree of forearm pronation or supination at FC. We also sought to evaluate the association between the degree of forearm pronation or supination at FC with throwing arm kinetics, including elbow varus torque, both at the individual level (intrapitcher) and between pitchers (interpitcher). We hypothesized no difference in forearm motion throughout the pitching motion would be observed between high school and professional pitchers. We also hypothesized no significant association between elbow varus torque and forearm pronation at FC would be observed.
Methods
High school and professional baseball pitchers were included in this study. The data sets of professional baseball pitchers who had previously undergone a biomechanical pitching assessment were provided by Motus Global. Motus Global deidentified all data before distribution, qualifying this study for exemption from institutional review board approval under federal guidelines.
Inclusion criteria were professional pitchers who were on a major league or minor league (low A, high A, AA, and AAA) roster without record of serious injury (requiring >2 weeks of rest or rehabilitation) in the previous 6 months as well as high school pitchers who were actively on a high school or club baseball team at the time of testing, who were without record of severe injury (requiring >2 weeks of rest or rehabilitation) within the past 6 months, and who had been cleared by a medical professional to participate in baseball activities. Before participation, high school and professional pitchers were administered a privacy waiver and provided written informed consent. For underage pitchers, the parent or guardian signed the waiver and pitchers gave assent.
Demographic data were provided by the pitcher and including age, preferred throwing arm, experience level, and injury history. Research staff measured and recorded each pitcher’s height and mass. The pitcher was given unlimited time to warm up with his preferred routine for pitching at full effort (eg, arm bands, stretching, plyometric care, and long toss). Once the pitcher indicated he was ready, 46 reflective markers were positioned on anatomical landmarks as defined previously. 15 Positional coordinate data of the reflective markers were collected using an 8-camera Raptor-E motion-analysis system (Motion Analysis Corp) at 480 Hz. Prior to recording the pitches, a single static calibration was performed to align the pitcher with the laboratory coordinate system and to define the local coordinate systems. The global coordinate system was established based on International Society of Biomechanics standards 34 : Y was vertically upward, X was perpendicular to Y (positive toward home plate from the pitcher’s mound), and Z was the cross-product of X and Y.
Pitchers were directed to pitch between 8 and 12 fastballs with gamelike effort from a regulation dirt mound to a catcher behind home plate at a regulation distance (18.4 m). Pitchers were allowed to pitch at their own set pace. Ball velocity was collected with a radar gun behind the pitcher (Stalker Sports Radar).
All data processing was performed using custom MATLAB scripts (MathWorks) as described previously. 6,15 Data from the markers were filtered by a low-pass filter (fourth-order, zero-lag Butterworth filter, 13.4-Hz cutoff frequency). 14 FC was identified as the first frame when the lead toe or heel in the Z-axis reached the minimum height. Ball release was calculated as the instant 0.01 seconds after the wrist joint center passed the elbow joint center in the positive X direction. 9 Stride length was defined as the distance from the stance leg medial malleolus at the time of maximum knee height to the lead leg medial malleolus at the time of FC, normalized as a percentage of body height. Shoulder abduction was defined as the angle between the distal direction of the upper arm and the line between the two shoulder markers with respect to the frontal plane. Shoulder horizontal abduction was defined as the angle between the upper throwing arm and the upper trunk in the transverse plane. The angle between the distal directions of the upper arm and forearm of the throwing arm was used to define elbow flexion. Forearm pronation was measured as the degree of supination about the elbow, where the palm facing toward the torso was considered 0° of pronation and a palm facing directly downward was considered 90° of pronation (Figure 1). Pitch time was defined as a percentage that started at FC, 0%, and ended at ball release, 100%. The pitching motion was divided into 7 time points: 14 maximum knee height, hand separation, elbow extension, FC, maximum shoulder external rotation, ball release, and maximum shoulder internal rotation.

Forearm pronation measurement defined.
Statistical Analysis
Analyses were performed separately for the 2 populations (professional and high school pitchers) to avoid confounding based on playing levels. Within each population, all pitches with forearm pronation at >0° were assigned to the pronation group, whereas all pitches with forearm pronation at <0° were assigned to the supination group. Pitches with outlier values (≥3 or ≤3 SD away from the mean) for forearm pronation and ball velocity were removed. In addition, in each group, pitchers with <3 pitches or those with a range of forearm pronation <10° across pitches were removed to maintain an adequate range for intrapitch analyses. 20,31 A flowchart demonstrating the pitches and pitchers used in these analyses is included in Figure 2.

Flowchart demonstrating the number of pitches/pitchers utilized in analyses for the (A) high school and (B) professional pitcher cohorts. FC, foot contact. *The following parameters were evaluated for outliers: forearm pronation at FC, ball speed.
Two-sample t tests were used to compare demographic variables between the 2 groups. The interpitcher effect of forearm pronation on variables of interest were assessed with a simple linear regression model between the average value of the variable of interest and the average forearm pronation at FC per pitcher. The intrapitcher effect of forearm pronation on variables of interest were assessed using a mixed-linear effect model between the variable of interest and forearm pronation at FC for each pitch with random intercepts. In addition, 2-way mixed-effect analysis of variance (ANOVA) tests were used to account for repeated measures (more specifically, variables collected at multiple time points). The average values by pitcher in each group were used in the ANOVA tests to avoid over-representation because the number of pitches varied per pitcher. The parameters B (coefficient of regression), β (normalized coefficient of regression), P, and R 2 (coefficient of determination) were calculated for each regression model. Alpha was set at .05 for all analyses. Statistical analysis was performed using MATLAB 2021a (Mathworks).
Results
A total of 41 high school and 196 professional baseball pitchers were included in the evaluation (Table 1). There were 29 high school pitchers in the pronation subgroup and 12 in the supination subgroup. There were 181 professional pitchers in the pronation subgroup and 15 in the supination subgroup. At both playing levels, there were no differences in pronation and supination groups regarding age, height, weight, or mass (P min = .064).
Reported Demographics for Supinated and Pronated Forearm Cohorts Delineated by Playing Level a

a Values are reported as mean ± SD or n (%).
A comparison of the supinated and pronated high school and professional forearm rotational motions throughout the pitch is included in Figure 3. For all high school pitchers combined, pitchers began at a point of increased pronation (43° ± 30°) at maximum knee height that reached a peak value at hand separation (44 ± 31°). High school pitchers proceeded to supinate the arm throughout elbow extension (36 ± 42°) and FC (43 ± 30°), achieving a neutral degree of supination at maximum external rotation (1 ± 24°) and ball release (-1 ± 26°). When following through at maximum internal shoulder rotation, pitchers returned to a position of pronation (20 ± 31°). For all professional pitchers, a similar trend of forearm motions at distinct time points were reported. However, professional pitchers were shown to have increased forearm pronation from elbow extension (P = .023) to maximum shoulder external rotation (P = .022) compared with high school pitchers. Furthermore, professional pitchers achieved a neutral position at ball release distinctly (3 ± 17°), rather than from maximum shoulder external rotation to ball release as reported for high school pitchers. Finally, professional pitchers finished at maximum shoulder internal rotation with increased pronation compared with high school pitchers (29 ± 20 vs 20 ± 31°, respectively; P = .019). When comparing specific pronation/supination subgroups, there was no significant difference at any time points between the high school and professional pronation/supination subgroups (P min = .10).

Forearm pronation throughout distinct time points of the pitch according to (A) high school (HS) and professional (Pro) pitchers and (B) forearm-pronated and forearm-supinated HS and Pro pitchers. BR, ball release; EE, elbow extension; FC, foot contact; HS, hand separation; MER, maximum shoulder external rotation; MIR, maximum shoulder internal rotation; MKH, maximum knee height.
Variability in forearm pronation was also compared between the 2 playing levels. Compared with professional pitchers, high school pitchers’ forearm pronation variability (as measured by standard deviation) was lower at maximum knee height (12.5 vs 22.5; P < .001); not statistically different at hand separation (19.1 vs 23.3; P = .204); significantly higher at elbow extension (51.6 vs 19.6; P < .001); not statistically different at FC (19.3 vs 17.3; P = .393); not statistically different at maximum shoulder external rotation (12.4 vs 11.5; P = .566); not statistically different at ball release (13.5 vs 13.2; P = .808); and significant higher at maximum shoulder internal rotation (17.7 vs 13.4; P = .032).
Throwing arm kinematic and kinetic parameters are reported in Table 2 for high school and professional forearm pronation and supination cohorts. The high school pronation group had an average ball velocity of 31.4 ± 3.4 m/s, elbow flexion 99 ± 17°, forearm pronation 30 ± 19°, and elbow varus torque 54 ± 16 N·m. The high school supination group had an average ball velocity of 30.7 ± 2.3 m/s, elbow flexion 93 ± 24°, forearm pronation -14 ± 9°, and elbow varus torque of 49 ± 14 N·m. A mixed-factorial ANOVA for parameters evaluated is included in Table 3.
Kinematic and Kinetic Parameters in High School and Professional Pitchers According to Forearm Pronation and Supination Subgroups a

a BH, body height.
P Values for Mixed-Factorial ANOVA at Multiple Time Points (Foot Contact to Maximum Shoulder Internal Rotation) a

a Boldface P values indicate statistical significance (P < .05). ANOVA, analysis of variance.
Regression results between forearm pronation and supination at FC with kinematic and throwing arm kinetic parameters are listed in Table 4 for high school pitchers and Table 5 for professional pitchers. For every 10° increase in forearm pronation at FC for the individual high school pitcher, ball velocity decreased by 0.2 m/s (B = -0.02; β = -0.10; P = .017) and elbow distractive forces decreased by 7.3 N (B = -0.73; β = -0.09; P = .006). Elbow anterior force approached significance for the individual high school pitcher and noted a negative association with increased forearm pronation (B = -0.16; β = -0.04; P = .056). For every 10° increase in forearm pronation at FC for the individual high school pitcher, elbow flexion at FC decreased by 5° (B = -0.46; β = -0.47; P < .001), whereas maximum elbow extension velocity was achieved 0.6% later in the pitch (B = -1.53; β = -0.10; P = .011). Elbow medial force increased by 4.1 N (B = 0.41; β = 0.07; P = .020) and elbow varus torque increased by 0.8 N·m (B = 0.08; β = 0.06; P = .016) for every 10° increase in forearm supination at FC for the individual high school pitcher.
Results of Intrapitcher and Interpitcher Regression Analysis of Forearm Pronation/Supination at FC Among High School Pitchers (Independent Variable) with Kinematic and Kinetic Parameters that Achieved Significance (Dependent Variable) a
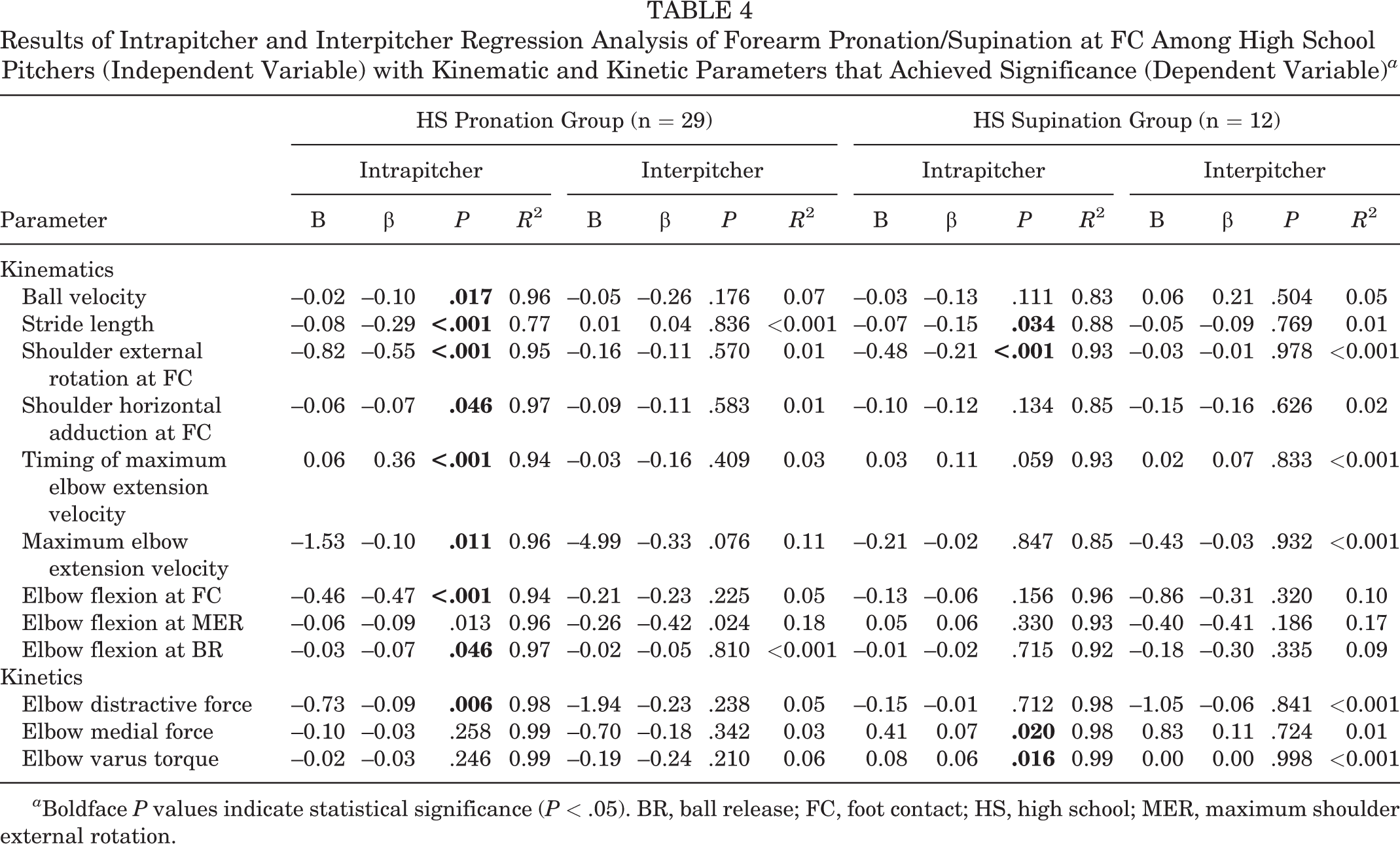
a Boldface P values indicate statistical significance (P < .05). BR, ball release; FC, foot contact; HS, high school; MER, maximum shoulder external rotation.
Results of Intrapitcher and Interpitcher Regression Analysis of Forearm Pronation/Supination at FC Among Professional Pitchers (Independent Variable) with Kinematic and Kinetic Parameters that Achieved Significance (Dependent Variable) a

a Boldface P values indicate statistical significance (P < .05). BR, ball release; FC, foot contact; MER, maximum shoulder external rotation.
For every 10° increase in forearm pronation at FC for the individual professional pitcher, ball velocity increased by 0.1 m/s (B = 0.01; β = 0.08; P = .007), shoulder external rotation at FC decreased by 9° (B = -0.90; β = -0.69; P < .001), and shoulder abduction at FC decreased by 6° (B = -0.06; β = -0.09; P < .001). Elbow anterior force decreased by 2.3 N (B = -0.23; β = -0.06; P = .002) and elbow distractive force decreased by 10.4 N (B = -1.41; β = -0.08; P = .017) for every 10° increase in forearm pronation at FC for the individual professional pitcher. For every 10° increase in forearm supination for the individual professional pitcher, ball velocity increased by 0.5 m/s (B = 0.05; β = 0.15; P = .031) and shoulder external rotation at FC decreased by 11° (B = -1.06; β = -0.23; P < .001). Elbow medial force decreased by 5.5 N (B = -0.55; β = -0.05; P = .009) for every 10° increase in forearm supination at FC for the individual professional pitcher.
For the individual or cohort of high school and professional pitchers, there were no significant correlations found between forearm pronation at FC and elbow varus torque (P min = .21).
Discussion
In the present study, we have examined excessive forearm pronation/supination at FC as a source of potential increased elbow varus torque and, consequently, as a surrogate for potential injury risk. The major findings of this study were that (1) there was no significant correlation found between forearm pronation at FC and elbow varus torque for the individual or cohort of high school and professional pitchers (P min= .21), with additional throwing arm kinetics, such as elbow anterior force and distractive force, only showing negative associations with forearm pronation for the individual pitcher at both levels; (2) forearm pronation at FC was significantly associated with several kinematic parameters including the timing of maximum elbow extension velocity as well as shoulder external rotation and elbow flexion at FC for both cohorts at the individual level; (3) forearm supination was significantly positively associated with elbow varus torque for the individual high school pitcher; and (4) ball velocity had mixed relationships with forearm pronation/supination dependent on both the playing cohort evaluated and when delineating between the individual pitcher versus cohort.
Our results lend support to the theory that increased forearm pronation may not be a significant risk factor for increased elbow varus torque and by extension UCL injury in high school and professional pitchers. Even more, our study noted additional throwing arm kinetics such as elbow anterior force and distractive forces showed weakly negative associations with forearm pronation for the individual pitcher, in both high school and professional players, suggesting that increasing pronation for any given pitcher likely carries little risk of increased kinetic forces/torques about the elbow joint. To the best of the authors’ knowledge, only 1 other group has evaluated the role of forearm kinematics with elbow kinetic outcomes. Solomito et al 32 investigated collegiate pitchers and observed that at terminal extension of the forearm for the fastball, there was a negative association between pronation and elbow varus torque (P = .013). Though some cadaveric studies have demonstrated elbow varus laxity was greater when the forearm was pronated compared with supinated and, thus may carry risk of UCL injury with excessive pronation, 25,26 these are inappropriately applicable to an in vivo pitching sequence for numerous reasons. First, the degree of pronation in these cadaveric studies is beyond the range of motion (ROM) of that observed in vivo (cadaveric studies, 40-80°; normal patient ROM, 70-85°). 35 Multiple cadaveric studies utilized specimens with cut UCLs, allowing movement at ranges well outside the typical ROM. 25,29 These studies were able to derive greater elbow varus torque values when straining the forearm beyond its normal limits with very little in vivo applicability to forces experienced by pitchers. In addition, there was no muscle contraction present for cadavers, which may be protective in the clinical setting. Furthermore, simply because a muscle may have a primary role of pronating the arm and a secondary role in stabilization against varus instability, this does not mean that performing the primary activity always leads to the secondary role.
In this study, it was observed that forearm pronation at FC was significantly associated with several other kinematic parameters. In particular, professional and high school pitchers with increased forearm pronation at the individual level had decreased elbow flexion and shoulder external rotation at FC, while achieving maximum elbow extension velocity later in the pitch. These are important findings given that increased elbow flexion, 16 shoulder external rotation, 18 and improper timing of maximum segmental joint velocities 17,19,24,30 have all been studied previously and implicated in increased throwing arm kinetics or injury risk. Though these parameters were evaluated during later portions of the pitch (ie, maximum shoulder external rotation, ball release), the means by which one kinematic may influence subsequent portions of the pitching motion is important in elucidating combinatory sequences that may pose the highest injury risk to pitchers and warrants further investigation. Although there was a positive relationship found between forearm pronation at FC and other full-body kinematics, the directionality of these relationships is unknown.
Although forearm pronation had no significant kinetic relationships, forearm supination at FC did show a positive association with elbow varus torque for the individual high school pitcher. Solomito et al 33 additionally observed that for every 1-N·m increase in the supination moment at maximum elbow extension, there was a 1-N·m increase in elbow varus torque. Therefore, the potential for forearm supination as a source of elevated elbow varus torque during early (current study) and late (Solomito et al 33 ) portions of the pitching sequence remains plausible. Coaches may consider instructing pitchers to avoid extreme supination motions of the forearm throughout the pitch.
Ball velocity had mixed associations with forearm pronation/supination dependent on the playing cohort evaluated, as well as, when delineating between the individual pitcher versus cohort. In particular, for the individual high school pitcher, ball velocity decreased with increased forearm pronation, whereas for the individual professional pitcher, ball velocity increased with greater pronation, as well as supination. Ultimately, it would be difficult to draw any final conclusion based on these results, but it is plausible that professional pitchers may be able to achieve faster ball velocity at more extreme degrees of pronation and/or supination. Though statistically significant, these associations were weak and likely may not have significant performance benefit implications. Additional investigations are needed to fully explore these ball velocity associations with forearm kinematic motions.
Strengths and Limitations
A strength of this study is its evaluation of high school and professional baseball pitching groups separately. Although other studies involving collegiate pitching populations may be related, they are not identical, with unique outcomes having been found between collegiate and professional baseball players in prior studies. 7,10 Some noted sources of differentiation include power, speed, and agility, as well kinematic and kinetic measures such as maximum pelvic velocity, elbow flexion torque, and elbow varus torque during the pitch. Therefore, isolating and reporting on these unique subsets is beneficial for adequate characterization of an important subset. Reporting all elbow kinetic parameters, conducting an intrapitcher and interpitcher analysis, as well as the large sample size evaluated for the professional cohort are additional strengths unique to this study.
A limitation of this study is the inability to assess if forearm pronation is an acquired trait, inherent, or influenced by musculoskeletal capacity or by coaching direction, given that pitchers were tested at a single point in time with little understanding of a pitcher’s longitudinal progress or changes in pitching kinematics over time. It is possible that due to instruction when learning to pitch, pitchers are taught different degrees of pronation and retain that degree of pronation throughout the pitching sequence. Future studies are needed to track pitchers over time to better understand how changes in kinematics may influence loads experienced on both the shoulder and the elbow. In addition, although a positive association was noted between forearm pronation at FC and other full-body kinematics, the directionality of these relationships is unclear. The current study evaluated a specific point in the kinematic sequence. There may be several variables that play a role in the subsequent kinematic sequence that can increase loads on the medial elbow.
Furthermore, wrist injury has been observed as the third most common musculoskeletal injury in professional pitchers after elbow and shoulder. 13 Preliminary data have found an association between forearm pronation and increased forces on the ulnar portion of the wrist. 33 Our study did not assess kinetics about the wrist and is warranted in additional studies to see if this kinematic may have important consequences at the more distal joint. In addition, musculoskeletal parameters (ie, passive and active range of motion, muscular strength) were not included in this study, which may have better supplemented our study findings and may be warranted in future evaluations. This study did not include an evaluation of shoulder kinetics, and thus the potential deleterious effects of forearm motion on the shoulder cannot be commented on. The skin-marker interaction may not adequately represent reflective marker placement at the anatomic surface intended. Finally, though injury risk can be implied through the use of throwing arm kinetics as a surrogate for ligament and soft tissue loading, we did not report actual injury incidence in these pitchers and the direct influence of injury risk should not be presumed, limiting this study’s clinical applicability.
Conclusion
Pitchers often utilize a supination- or pronation-predominant forearm motion throughout the pitching motion; however, the sequence chosen does not appear to significantly differ between playing levels when comparing high school with professional pitchers. Our results also lend support to the theory that excessive forearm pronation at FC may not be a significant risk factor for increased throwing arm kinetics and, by extension, injury. Although forearm pronation had no significant kinetic relationships, forearm supination at FC did have a positive, weak association with elbow varus torque for the individual high school pitcher. Ultimately, coaches and pitchers may be better served by redirecting their focus onto other mechanical aspects of the pitch that may have stronger associations with injury risk implications as well as performance.
Footnotes
Final revision submitted September 6, 2022; accepted September 26, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.B.C. has received education payments from Arthrex and hospitality payments from Smith & Nephew. L.V.G. has received consulting fees from DePuy Synthes, Exactech, and Responsive Arthroscopy and royalties from Exactech and Zimmer Biomet. J.S.D. has received education payments from Gotham Surgical; consulting fees from Arthrex, Merck Sharp & Dohme, and Trice Medical; speaking fees from Arthrex; and royalties from Linvatec and Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by the Hospital for Special Surgery.