
Abstract
Background:
Routine hip magnetic resonance imaging (MRI) before arthroscopy for patients with femoroacetabular impingement syndrome (FAIS) offers questionable clinical benefit, delays surgery, and wastes resources.
Purpose:
To assess the clinical utility of preoperative hip MRI for patients aged ≤40 years who were undergoing primary hip arthroscopy and who had a history, physical examination findings, and radiographs concordant with FAIS.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Included were 1391 patients (mean age, 25.8 years; 63% female; mean body mass index, 25.6) who underwent hip arthroscopy between August 2015 and December 2021 by 1 of 4 fellowship-trained hip surgeons from 4 referral centers. Inclusion criteria were FAIS, primary surgery, and age ≤40 years. Exclusion criteria were MRI contraindication, reattempt of nonoperative management, and concomitant periacetabular osteotomy. Patients were stratified into those who were evaluated with preoperative MRI versus those without MRI. Those without MRI received an MRI before surgery without deviation from the established surgical plan. All preoperative MRI scans were compared with the office evaluation and intraoperative findings to assess agreement. Time from office to arthroscopy and/or MRI was recorded. MRI costs were calculated.
Results:
Of the study patients, 322 were not evaluated with MRI and 1069 were. MRI did not alter surgical or interoperative plans. Both groups had MRI findings demonstrating anterosuperior labral tears treated intraoperatively (99.8% repair, 0.2% debridement, and 0% reconstruction). Compared with patients who were evaluated with MRI and waited 63.0 ± 34.6 days, patients who were not evaluated with MRI underwent surgery 6.5 ± 18.7 days after preoperative MRI. MRI delayed surgery by 24.0 ± 5.3 days and cost a mean $2262 per patient.
Conclusion:
Preoperative MRI did not alter indications for primary hip arthroscopy in patients aged ≤40 years with a history, physical examination findings, and radiographs concordant with FAIS. Rather, MRI delayed surgery and wasted resources. Routine hip MRI acquisition for the younger population with primary FAIS with a typical presentation should be challenged.
Femoroacetabular impingement syndrome (FAIS) is an increasingly recognized cause of hip pain in young adults. FAIS is defined by symptoms, physical examination findings, and abnormal femoral and/or acetabulum morphology on radiographs. 8,10,31 The abnormal morphology of the femur and/or acetabulum results in incongruous contact between the acetabular rim and the proximal femur, leading to hip pain, acetabular labral injury, and hip osteoarthritis. 9
While nonoperative modalities can improve symptoms, arthroscopy improves symptoms better than nonoperative options. 11,18,27,32 Unsurprisingly, hip arthroscopy for FAIS has increased over the past 15 years. 4,5,24,35 Recent data suggest that hip arthroscopy within 6 months of symptom onset yields better outcomes than delayed surgical intervention, suggesting time to hip arthroscopy may be a critical factor. 18
Hip magnetic resonance imaging (MRI) is an advanced imaging modality often ordered to aid in the evaluation of FAIS. 2,26 While limited, some data suggest that routine use of MRI is not cost-effective in the diagnosis and treatment of FAIS. 7 Recently, Ramkumar et al 28 challenged the clinical utility of preoperative hip MRI in young patients with FAIS with concordant history, physical examination findings, and plain radiographs at a single institution.
The purpose of the study was to assess the clinical utility of the preoperative hip MRI for patients aged ≤40 years who were undergoing primary hip arthroscopy and who had a history, physical examination findings, and radiographs concordant with FAIS. Clinical utility included changes in the decision to operate, surgical plan, time to surgery, and cost based on the preoperative MRI. We hypothesized that preoperative hip MRI would add little clinical utility in this patient population.
Methods
Patient Selection
After obtaining institutional review board approval for this study, we retrospectively identified patients undergoing hip arthroscopic surgery for treatment of FAIS at 1 of 4 separate quaternary academic referral centers between August 27, 2015, and December 31, 2021. Patients were indicated for surgery after failing nonoperative management including activity modification, physical therapy, and nonsteroidal anti-inflammatory medications and/or intra-articular hip injections as noted on the electronic medical record. All surgeries were performed by 1 of 4 fellowship-trained hip arthroscopy surgeons (E.C.M., A.J.K., J.T.R., J.D.H.) with 8 to 12 years of arthroscopy experience and intentionally heterogeneous practices, with case volumes ranging from 25 to 350 patients per year.
Patient inclusion criteria were documented history, physical examination, and plain radiographic findings (cam, pincer, or mixed deformities) consistent with FAIS in patients aged ≤40 years undergoing a primary hip arthroscopy. The age threshold was arbitrarily defined. Exclusion criteria included previous hip surgery, acetabular dysplasia (defined by lateral center-edge angle <20°), underlying hip osteoarthritis (Tönnis grade ≥2), patients with a contraindication to undergoing MRI, patients who elected to reattempt an additional round of nonoperative management, patients who underwent a concomitant periacetabular osteotomy, and patients who were otherwise delayed by extraneous factors (ie, social circumstances). Patients with atypical hip pain, suspicion of stress reaction, synovitis, or pain out of proportion did not meet inclusion criteria, as they failed to have FAIS concordance across the history, physical examination, and radiographs.
Included individuals were stratified into 2 groups for comparison: those who were evaluated without MRI versus those who were evaluated with MRI. The decision to proceed with surgery for both groups was made at the time of the initial visit before MRI for the group that was not evaluated with MRI. MRI scans in those who were not evaluated with MRI were ordered because of protocol and/or prior authorization concerns. These 3.0-T MRI scans were ordered without contrast and performed within the health system regions. MRI scans among those who were evaluated with MRI were of mixed quality (1.5 T, 3.0 T, or other) and included both with and without contrast. If ordered within the health system, both a radiologist and a lead surgeon reviewed the MRI scans in both groups. Only lead surgeons reviewed the MRI scans for patients who were evaluated with MRI outside the health system. Postoperative protocols varied across surgeon practices.
Data Collection
Patients' medical records were retrospectively reviewed to record plain radiographic and MRI findings, documented history and physical examination findings, and baseline demographic data. Clinical diagnostic criteria for FAIS were noted as groin or hip pain; pain in the anterior impingement and/or flexion, adduction, internal rotation positions; and limited hip flexion and internal rotation. Radiographic diagnostic criteria for FAIS were noted as evidence of a cam morphology on the femur, pincer lesion on the acetabulum (crossover sign), a mixed cam-pincer deformity, Tönnis grade <2, alpha angle >55°, and lateral center-edge angle >40°. MRI findings of presence and location of labral tear were recorded.
To assess for agreement, the preoperative MRI interpretations were subsequently compared with the in-office evaluation (history, physical examination, and plain radiographs) and the intraoperative findings at the time of hip arthroscopy. In addition to baseline demographic data, time from the last office visit whereby the next step was established to be hip arthroscopy was recorded in both groups. Time from this office visit to MRI was also recorded in the group that was not evaluated with MRI. Patients were either telephoned or seen in the office after the MRI scans were acquired to review the findings and schedule surgery. Patient-reported outcomes were not consistently collected or available for all 4 surgeon practices and were outside the scope of the study. Total expenditures were calculated based on a previously established median price of US$2114 per MRI session. 2
Statistical Analysis
We used an independent t test with an alpha value of .01 to compare the time from surgical indication to surgery in individuals evaluated with MRI versus those not evaluated with MRI. Statistics were performed in Excel (Microsoft Corp).
Results
A total of 2298 patients underwent hip arthroscopy during the study period: 1767 over 5 years at the first institution, 291 over 1 year at the second institution, 81 over 2 years at the third institution, and 159 over 6 years at the fourth institution. Of these patients, 1391 met the inclusion criteria and were indicated for hip arthroscopy; 63% were female, with a mean body mass index (BMI) of 25.6 and mean age of 25.8 years (Table 1). Of the patients indicated for hip arthroscopy for FAIS correction based on history, physical examination, and radiographs, 322 (23.1%) patients were not evaluated with MRI versus 1069 (76.9%) with MRI (Figure 1). No statistical differences existed between the 2 groups in terms of sex, BMI, age, or Tönnis grade.
Demographic Data of the Included Patients a
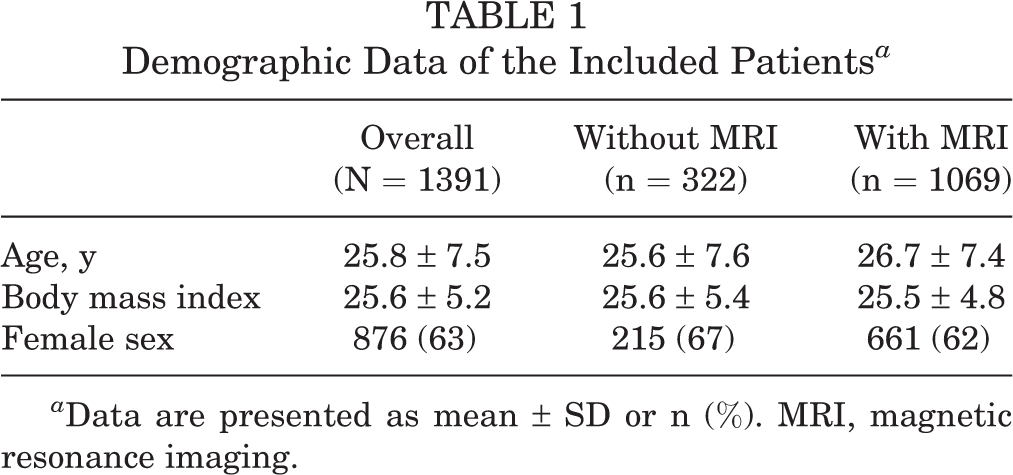
a Data are presented as mean ± SD or n (%). MRI, magnetic resonance imaging.

Flowchart of inclusion and exclusion criteria of patients in the current study. MRI, magnetic resonance imaging.
Of the 322 patients without MRI, preoperative MRI did not alter the decision to operate or the surgical plan at any institution. Patients in both groups had preoperative MRI findings demonstrating anterosuperior labral tears that were redemonstrated upon surgeon review. All labra were repaired intraoperatively during arthroscopy, with the exception of 5 (0.2%) that were selectively debrided. No labra were primarily reconstructed. Radiologists reported labral pathology in 1041 of the 1069 (97.4%) MRI scans. Upon surgeon review, all 1069 had labral pathology. No patients in either group had a “surprise diagnosis” at the time of arthroscopy (Table 2). MRI demonstrated questionable articular cartilage pathology in 7 patients; however, none underwent additional surgical treatment beyond chondroplasty.
Patients With History, Clinical Examination, Radiographic Findings, and MRI Consistent With FAISa

a Data are presented as percentage or mean ± SD. FAIS, femoroacetabular impingement syndrome; MRI, magnetic resonance imaging.
The estimated aggregate preoperative MRI cost was US$2,940,574 for the entire cohort of patients whose preoperative MRI did not alter the preoperative or intraoperative surgical plan. The mean times from office visit to the operating room for arthroscopy for patients who were not evaluated with MRI versus those who were was 93.5 ± 61.7 and 63.0 ± 34.6 days, respectively (P < .01). Patients who initially were not evaluated with MRI underwent surgery 6.5 ± 18.7 days after MRI acquisition. Time to noncontrast MRI was 24.0 ± 5.3 days for the patients without MRI. The data from all 4 cohorts are detailed in Table 3.
Summary Data Across All 4 Hip Arthroscopy Practices for Patients Evaluated With Versus Without MRIa

a Data are presented as mean ± SD. MRI, magnetic resonance imaging.
b Statistically significant difference in time from surgical indication visit to hip arthroscopy (P < .01).
Discussion
The study findings demonstrated that MRI in patients aged ≤40 years with a history, physical examination, and radiographs consistent with FAIS did not affect the decision to operate or surgical plan in a cohort of 1391 patients from 4 academic referral centers. MRI scans are ordered to provide additional information when diagnosis is unclear based on ambiguous physical examination and radiographs. Similarly, insurance may require MRI scans before authorization, and patients may want imaging to verify diagnosis. However, in patients not evaluated with MRI, surgical wait times were longer than those evaluated with MRI (93.5 ± 61.7 vs 63.0 ± 34.6 days; P < .01). This suggests that preoperative hip MRI in this patient cohort delays time from surgical indication to surgery without changing the decision to operate or surgical plan. Therefore, the MRI did not provide additional information or affect diagnosis in this group of patients. Interestingly, patients not evaluated with MRI underwent surgery 6.5 days after acquiring the MRI instead of the expected 63 days of surgical wait time. This is likely because patients not evaluated with MRI were placed on the surgical schedule before imaging to prevent delays in treatment. Therefore, this supports the idea that hip specialists should order the MRI versus referring providers. 12 –16,19 Primary care physicians should feel comfortable referring hip pain to a hip arthroscopy specialist despite any influx of nonspecific hip pain because hip arthroscopy specialists are the gatekeepers of clinical value and resource stewardship. While there does exist the risk that primary care providers may refer an increased volume of non-FAI hip pathologies to hip arthroscopy surgeons, this will provide ample opportunity for imaging stewardship and expert triage.
Moreover, the near-consensus labral repair in the absence of cartilage repair techniques in this report suggests that the surgical management of FAIS is primarily a bony operation. 20,21 Cunningham et al 7 reported that history and a physical examination may be preferred to advanced imaging in FAIS diagnosis, as MRI did not provide additional value besides increased cost. Similarly, authors in Ontario, Canada, noted that as hip MRI scans increased from 700,000 to 1.7 million over a 10-year period, patient wait times for hip MRI scans increased to several months. 19 This further supports our conclusion that routine preoperative hip MRI adds limited clinical utility in patients aged ≤40 years with FAIS with concordant history, physical examination, and radiographs. 34
Aside from delays in treatment, MRI scans have monetary costs. Anthony et al 2 reported on the bundled cost of MRI in the state of Iowa across 136 institutions. The median call duration for scheduling an MRI was 9 minutes, with a median bundled cost of $2114 without an appreciable cost decrease for 1.5-T MRI scans compared with 3-T MRI scans. 2 When extrapolated to the current study of approximately 1300 patients, this would result in 209 hours of phone time for scheduling and an additional cost of $2,940,574 for the patients. This does not consider the cost of the patient missing work, time for interpretation by a radiologist, or personnel needed to authorize and contact patients about results. This approximates a mean cost of $2114 per patient. Similarly, this does not factor in the additional costs of imaging errors such as false negatives on clinical resources and patients. Taken together, the money and time saved from not ordering MRI scans may be better used in other direct patient-related activities. 6,30
Our data provide multicenter validation to the study by Ramkumar et al 28 that initially questioned the clinical utility of preoperative hip MRI and quantified the delay to surgical management in this population. Aside from cost, delay due to MRI potentially compromises patient outcomes, too. Ouyang et al 25 reported that younger age at surgery results in earlier achievement of clinically meaningful improvement after hip arthroscopy. Similarly, Mehta et al 22 reported that immediate hip arthroscopy results in significantly better outcomes due to immediate restoration of good function when compared with delayed hip arthroscopy. Delayed hip arthroscopy may result in rapidly progressive arthritis in some patients, and earlier evaluation may be key in limiting chondral damage from large cam lesions in FAIS. 29
Overall, the data and literature suggest that the fundamental cornerstone in FAIS diagnosis is history, physical examination, and radiographs, not MRI scans. 17 An international consensus of 22 panel members agreed that MRI is not a requirement but a recommendation to gain additional information if warranted by the acting surgeon. 10 This agreement is endorsed by 25 subspeciality societies, including the American Medical Society for Sports Medicine, the International Society for Hip Arthroscopy, and the European Society of Sports Traumatology, Knee Surgery and Arthroscopy, among others. 10
Limitations
This study is not without limitations. We did not evaluate patients who had an MRI but never went to surgery. Likewise, the strict inclusion criteria may not represent patients with FAIS with important anatomical considerations, such as version, dysplasia, borderline dysplasia, or avascular necrosis of the hip. A computed tomography scan may be useful, but this report should not be applied to computed tomography scan necessity. 1,3 While the multiple institutions and surgeons serve variable geographic populations, there may be inherent biases among patients who are evaluated at academic versus nonacademic centers. Additionally, only practices within the United States were studied, and the time to see a physician, acquire an MRI, and undergo surgery may not be generalizable to health systems in other countries. Heterogeneity between practices may also affect generalizability. For example, primary labral reconstruction and a preference for repair over debridement, as in this study, may not be globally reflected at other institutions. The inclusion of high- versus low-volume hip arthroscopic surgeons may skew results, as 1 of the 4 surgeons had all patients evaluated with MRI, which is not reflective of other groups. 23,33 Additionally, the COVID-19 pandemic affected surgical volumes and practice patterns in a manner that could not be accounted for in this review. Ideally, a prospective study with longitudinal follow-up would better elucidate the importance and drawbacks of MRI on surgical access for patients.
Conclusion
Once indicated for surgery on the basis of history, physical examination, and radiographs alone, preoperative MRI did not alter the indications or plans for primary hip arthroscopy in patients with FAIS aged ≤40 with concordant history, physical examination, and radiographs. Rather, MRI delayed surgery and wasted resources. Routine hip MRI acquisition for the young primary FAIS population with a typical presentation should be challenged.
Footnotes
Final revision submitted September 11, 2022; accepted September 26, 2022.
One or more of the authors has declared the following potential conflicts of interest or source of funding. P.N.R. has received consulting fees from Pacira Pharmaceuticals. A.P. has received hospitality payments from Medical Device Business Services. A.J.K. has received grant support from DJO and Exactech; consulting fees from Arthrex, Joint Restoration Foundation, and Responsive Arthroscopy; speaking fees from Arthrex; honoraria from Joint Restoration Foundation and Vericel; and royalties from Arthrex. E.C.M. has received education payments from Arthrex and Endo Pharm, consulting fees from Endo Pharm and Smith & Nephew, speaking fees from Smith & Nephew, and hospitality payments from Stryker. J.D.H. has received education payments from Medinc and Smith & Nephew, speaking fees and consulting fees from Smith & Nephew, and hospitality payments from Stryker. B.U.N. has received grant support from Arthrex; education payments from Arthrex, Medwest, and Smith & Nephew; consulting fees from Stryker; and hospitality payments from Medical Device Business Services. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by Cleveland Clinic (reference No. 21-470).