
Abstract
Background:
While medial meniscocapsular tears (ramp lesions) are commonly associated with isolated anterior cruciate ligament injuries, there are limited descriptions of these meniscal injuries in multiligament knee injuries (MLKIs).
Purpose:
To (1) retrospectively evaluate preoperative magnetic resonance imaging (MRI) scans for the presence of ramp lesions in patients surgically treated for acute grade 3 combined posterolateral corner (PLC) knee injuries and (2) determine if a preoperative posteromedial tibial plateau (PMTP) bone bruise is associated with the presence of preoperative ramp lesions on MRI in these same patients.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Data on consecutive patients at a level 1 trauma center with MLKIs between 2001 and 2021 were retrospectively reviewed. Only patients with acute grade 3 combined PLC injuries who received an MRI scan within 30 days of injury were assessed. Two musculoskeletal radiologists retrospectively reviewed each patient’s preoperative MRI for evidence of ramp lesions and bone bruises. Intraclass correlation coefficients (ICCs) were used to calculate reliability among the reviewers. Multivariate analysis was used to evaluate the relationship between PMTP bruising and the presence of a ramp lesion on MRI.
Results:
A total of 68 patients (79.4% male; mean age, 33.8 ± 13.7 years) with an acute grade 3 combined PLC injury were included in the study. On MRI, the ICCs for detection of ramp lesions and PMTP bone bruising were 0.921 and 0.938, respectively. Medial meniscal ramp lesions were diagnosed in 18 of 68 (26.5%) patients. Eleven of 18 (61.1%) patients with ramp lesions also showed evidence of PMTP bruising, while 13 of 50 (26.0%) patients without ramp lesions had PMTP bruising (P = .008). When controlling for age and sex, PTMP bruising was significantly associated with the presence of a ramp lesion in combined PLC injuries (odds ratio, 4.62; P = .012).
Conclusion:
Preoperative medial meniscal ramp lesions were diagnosed on MRI in 26.5% of patients with acute grade 3 combined PLC injuries. PMTP bone bruising was significantly associated with the presence of a ramp lesion on MRI. These findings reinforce the need to assess for potential ramp lesions at the time of multiligament reconstruction.
Keywords
Injury to the posterolateral corner (PLC) of the knee is often devastating, most commonly occurring with combined injuries to the anterior cruciate ligament (ACL) and/or posterior cruciate ligament (PCL). 6,12,20 In acute grade 3 combined PLC injuries, the PLC can be treated with surgical repair, repair plus augmentation, or reconstruction, depending on both the location and chronicity of the injuries. 6,12,20,21,29 In combined PLC injuries (ACL-PCL-PLC), a single-staged surgery is recommended in order to treat all the ligamentous injuries. While experts have taken a particular interest in improving surgical outcomes, there exist limited studies reporting on the prevalence of concomitant meniscal injuries in a combined PLC injury. 5,6,12,18 –20,26
Meniscocapsular tears of the posterior horn of the medial meniscus, termed ramp lesions, have garnered particular attention in the setting of isolated ACL ruptures; if not addressed, these injuries confer an increased risk for graft failure after ACL reconstruction. 4,7,10,22 Ramp lesions have been reported to occur concomitantly in 9% to 42% of isolated ACL injuries and can be difficult to detect through physical examination and standard anterolateral and anteromedial arthroscopic exploration, as these tears hide in the posteromedial “blind spot.” 1,7,16,28,30 Despite the well-established association between isolated ACL injuries and ramp lesions, there are limited studies that have reported on ramp lesions in the multiligament-injured knee. This association is particularly important, as it is unknown whether missed ramp lesions could increase the failure risk of the reconstructed ACL, PCL, and/or PLC.
As ramp lesions have a propensity to elude diagnosis, secondary signs of injury have been described in an effort to increase detection and recognition. 4,7,8,16,22 Bone bruises have proven to be useful in such a manner, serving as an indirect sign that concomitant injury may be present. 16,23,27 As such, various reports have suggested that ramp lesions are 3 to 6 times more likely to be observed when posteromedial tibial plateau (PMTP) bone bruising is present in patients with isolated ACL injuries. 2,15 However, there are limited reports of this secondary sign in combined PLC injuries.
The primary goal of this study was to retrospectively evaluate preoperative magnetic resonance imaging (MRI) scans for the presence of ramp lesions in patients surgically treated for acute grade 3 combined PLC knee injuries. A secondary goal was to determine if a preoperative PMTP bone bruise is associated with the presence of preoperative ramp lesions on MRI in these same patients.
Methods
A retrospective review of the electronic medical records was performed to identify patients with specific Current Procedural Terminology and International Classification of Disease codes that indicate the management of a multiligament knee injury (MLKI) between January 2001 and March 2021 at Yale–New Haven Hospital, a level 1 trauma center. A total of 123 MLKI patients were identified.
Classification of MLKIs
For our institutional MLKI database, all ligament injuries were initially diagnosed via MRI and confirmed through operative reports. The official radiology report was completed by a board-certified musculoskeletal fellowship-trained radiologist and then reviewed and compared with the MRI assessment of a board-certified orthopaedic sports medicine fellowship-trained surgeon (M.J.M). All multiligament injuries were listed and classified according to the location of the structural injury. If there was discrepancy between the 2 MRI assessments and intraoperative findings, or if there was uncertainty in the structural ligamentous diagnosis, clinical, and/or intraoperative findings, the orthopaedic surgeon’s final postoperative diagnosis was utilized as the definitive diagnosis of the patient’s ligament injury. 13,14
In our previously established MLKI database, an MLKI was defined as an injury to 2 or more of the 4 major ligaments of the knee (the ACL, PCL, superficial medial collateral ligament [sMCL], and/or the lateral [fibular] collateral ligament [LCL]). Grade 3 combined PLC injuries were defined as complete ligamentous disruption to the PLC with combined injuries to the ACL, PCL, and/or MCL. Grade 3 PLC injuries were defined as complete ligamentous disruption of the LCL, in addition to complete injury to ≥1 of the following: the biceps femoris tendon, the popliteofibular ligament, and/or the popliteal tendon. Patients were then classified into subgroups based on the ligament injuries according to the modified Schenck classification (Table 1).
Modified Schenck Classification System for Knee Dislocations a

a ACL, anterior cruciate ligament; KD, knee dislocation; LCL, lateral cruciate ligament; MCL, medial collateral ligament; PCL, posterior cruciate ligament.
Patient Selection
Of the 123 MLKIs in our database, 77 patients were identified as having surgically treated grade 3 combined PLC injury that was originally diagnosed on MRI and confirmed with operative reports. The exclusion criteria for this study included (1) >30 days between initial injury and MRI; (2) lack of T2-weighted fat-suppressed MRI sequences; and (3) prior ipsilateral ligamentous knee injury. As a result, 9 patients were excluded from this study. Of the remaining 68 patients with surgically treated grade 3 combined PLC injuries, the following inclusion criteria were then applied: (1) <30 days between date of the reported injury and date of the MRI; (2) T2-weighted fat-suppressed MRI sequences available in both the coronal and sagittal planes; and (3) no history of prior ligamentous or meniscal knee injury. All 68 patients with acute grade combined 3 PLC injuries were included in the final analysis.
Preoperative MRI Review for Medial Meniscal Ramp Lesions and PMTP Bone Bruising
Preoperative MRI scans were performed with a field strength of 1.5 T or 3.0 T using a 15-channel knee coil with a combination of fat suppression and proton-density sequences. For the current study, the MRI scans of the 68 patients were retrospectively and independently re-reviewed by 2 board-certified musculoskeletal radiologists blinded to all clinical data, one of whom (A.W.) had 7 years of clinical experience and the other (L.D.K.) with 39 years of clinical experience. MRI scans were retrospectively reviewed for the presence of ramp lesions and the presence of a PMTP bone bruise. Ramp lesions were not confirmed with arthroscopic exploration.
The MRI criteria put forth by Zappia et al 32 were used to define the presence of a ramp lesion in this study. These criteria have exhibited excellent sensitivity, specificity, and interreader reliability for the detection of ramp lesions on MRI relative to arthroscopically confirmed ramps through a posteromedial portal. 32 On MRI, medial meniscal ramp lesions were defined as a vertical (longitudinal) tear of the peripheral capsular attachment of the posterior horn of the medial meniscus at the meniscocapsular junction. Zappia et al’s criteria for diagnosing the presence of a ramp lesion on MRI included if the concave band (ramp capsule) with low signal intensity posterior to the posterior horn of the medial meniscus was interrupted by a line of hyperintensity crossing this capsular reflection.
For bone bruises, only fat-suppressed T2-weighted coronal and sagittal images were reviewed to determine the location of the bone bruises within the tibiofemoral compartment in the injured knee. For mapping bone bruises, a standardized technique described by Moran et al 23 –25 was utilized to record the location of the bruise(s) on the tibia. For tibial plateau bruise mapping, contusions on the medial side were defined as any bruise that occurred in the tibial-medial-medial (TMM) and/or tibial-medial-central (TMC) zones in the coronal plane (Figure 1A). Next, the sagittal location of these medial tibial plateau contusions was then recorded and localized to the either the anterior, central, or posterior zone (Figure 1B). PMTP bone bruises were defined as any contusion that occurred in the posterior (P)-TMM and/or P-TMC zones. The signal intensity and volume of the contusions were not recorded. If the contusion(s) was located across multiple zones, each individual zone of extension was counted. Similarly, if multiple contusions were present, contusions were counted separately to the individual zone(s) they spanned.

(A) Coronal proton-density magnetic resonance imaging (MRI) with distinct femoral and tibial zones used to record the location of the lesions in the coronal plane. The white circle marks the 2 zones (medial [M] and central [C]) for posteromedial tibial plateau bruising in the coronal plane. (B) Sagittal proton-density MRI of the medial tibial plateau with 3 zones: anterior (A), central (C), and posterior (P) for localization. The white circle marks the sagittal posterior (P) zone for posteromedial tibial plateau bruising. 23 L, lateral; LSs, lateral subspine; LT, lateral trochlea; MSs, medial subspine; MT, medial trochlea; N, notch.
An example of a patient with a surgically treated combined PLC injury that showed evidence of a ramp lesion and posteromedial bone bruise on preoperative MRI can be seen in Figure 2.

A magnetic resonance imaging example of a ramp lesion (top arrow) and a resultant bone bruise on the posteromedial tibial plateau (bottom arrow) in a patient with grade 3 combined posterolateral corner injury.
Statistical Analysis
Statistical analyses were performed using chi-square tests for categorical variable distributions when cell sizes were >5, Fisher exact tests when cell sizes were ≤5, Z tests for 2 proportions, and Student t tests for continuously distributed variables. Intraclass correlation coefficients (ICCs) were used to calculate the reliability between the 2 radiologists for diagnosing both medial meniscal ramp lesions and PMTP bone bruises; ICC values were defined as poor (<0.5), moderate (0.5-0.75), good (>0.75-0.9), or excellent (>0.9). 3 Multivariate logistic regression analysis was used to evaluate the correlation between bone bruising patterns and the presence of a ramp lesion, and a receiver operating characteristic (ROC) curve analysis was conducted to assess the discriminative ability for the presence or absence of a ramp lesion. All statistical analyses were performed using SPSS Version 28.0 (IBM) or Microsoft Excel (Microsoft). Statistical significance was set as P < .05, 2-sided.
Results
A total of 68 patients (79.4% male; mean age, 33.8 ± 13.7 years) with an acute grade 3 combined PLC injury were included in the study. The ICCs for the presence or absence of a PMTP bone bruise and ramp lesions were excellent and calculated to be 0.921 and 0.938, respectively. Medial meniscal ramp lesions were noted on MRI in 18 of 68 (26.5%) patients overall. Of the patients with ramp lesions, 14 of 18 (77.8%) had a knee dislocation (KD) 3L (ACL-PCL-PLC) injury, and 4 of 18 (22.2%) had a KD 1L (ACL-PLC or PCL-PLC) injury.
Bivariate Analysis
The bivariate analysis did not find significant differences between the patients with and patients without ramp lesions with respect to age, sex, body mass index, or injury classification (Table 2).
Baseline Characteristics Overall and in Patients With and Without Ramp Lesions a

a Values are presented as n (%) or mean ± SD. KD, knee dislocation.
Overall, 24 of 68 (35.3%) patients had a PMTP bone bruise, while 44 of 68 (64.7%) patients did not have a PMTP bone bruise. Of the 24 patients with a PMTP bone bruise, 11 (45.8%) had evidence of a ramp lesion on MRI. Of the 44 patients without a PMTP bone bruise, 7 (15.9%) had an associated ramp lesion. The presence of a PMTP bone bruise was significantly more common in patients with an associated ramp lesion compared with patients without a ramp lesion, as 11 of 18 (61.1%) patients with ramp lesions had PMTP bone bruises, compared with 13 of 50 (26.0%) patients with PMTP bone bruises but without ramp lesions (P = .008). The rates of the presence and absence of PMTP bone bruising in patients with and without ramp lesions are summarized in Table 3. The presence of other concomitant injuries was similar between the ramp and no-ramp groups, as demonstrated in Table 4.
Posteromedial Tibial Bone Bruising in Patients With and Without Ramp Lesions a
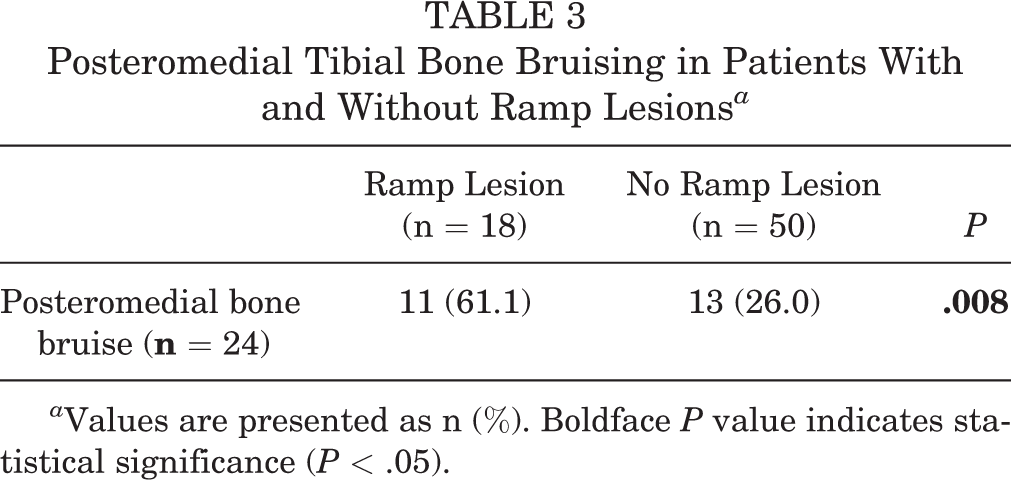
a Values are presented as n (%). Boldface P value indicates statistical significance (P < .05).
Concomitant Injuries in Patients With and Without Ramp Lesions a

a Values are presented as n (%). ACL, anterior cruciate ligament; IT, iliotibial; MCL, medial collateral ligament; PCL, posterior cruciate ligament.
Regression Analysis
The results of the multivariate logistic regression analysis indicated that PMTP bone bruising was a significant predictor for the presence of ramp lesions, when controlling for age and sex (odds ratio, 4.62; 95% CI, 1.402-15.19; P = .012). The results of the multivariate logistic regression model are summarized in Table 5.
Logistic Regression Model a

a OR, odds ratio; PMTP, posteromedial tibial plateau.
ROC Curve Analysis
The ROC curve of the predicted probabilities from the final logistic regression model demonstrated acceptable discrimination for the presence or absence of a ramp lesion, with an area under the curve of 0.716.
Discussion
The most important finding of this study was that medial meniscal ramp lesions were diagnosed on preoperative MRI in 26.5% of patients who were surgically treated for acute grade 3 combined PLC injuries. Second, we found that a PMTP bone bruise is significantly associated with the presence of a ramp lesion on preoperative MRI in these combined PLC injuries. The vast majority of ramp lesions (94%) recognized on MRI occurred in combined PLC injuries with ACL involvement (ACL-PLC or ACL-PCL-PLC). These findings reinforce the need to assess for potential ramp lesions at the time of ligament reconstruction in combined PLC injuries.
In this study, ramp lesions were retrospectively diagnosed in 18 (26.5%) patients with combined PLC injuries based on preoperative MRI. It is important to note that during the initial ligament reconstruction/repair, patients were not routinely assessed with a standard Gillquist maneuver or posteromedial portal for ramp lesions, and the presence or absence of a ramp lesion was not routinely documented in operative reports or searched for. Therefore, it is possible that these ramp lesions could have healed by the time of surgery, were missed at the time of surgery because of inadequate visualization and awareness, or, less likely, were not actually present. However, the possibility exists that the majority of these ramp lesions diagnosed on preoperative MRI were missed at the time of surgery, given the high specificity of the MRI methodology used in the current study. 30
Biomechanically, the static and dynamic stabilizers of the PLC primarily act to resist external tibial rotation. 6,17 As unrecognized ramp lesions increase the degree of external tibial rotation within the knee, 9 combined PLC injuries that contain this concomitant meniscal injury, in the setting of a repaired or reconstructed posterolateral knee, may be at an increased risk of not only ACL graft failure, but also failure of PLC graft/repair. However, future biomechanical and clinical studies are needed to assess the impact that missed ramp lesions can have not only on the ACL but also on the stability of the PLC repair and/or reconstruction, along with how this may influence clinical outcomes in these combined MLKIs.
In combined PLC injuries, our findings suggest that a PMTP bone bruise is significantly associated with the presence of a ramp lesion on MRI. While this secondary sign of meniscal injury has been reported in isolated ACL ruptures, 2,7,15,31 few studies have described these bruise findings in a cohort of patients with MLKIs. Geeslin and LaPrade 11 reported that the most common bruises in acute grade 3 combined PLC injuries were located on the anteromedial femoral condyle and the PMTP. However, the association between PMTP bruising and ramp lesions was not reported in this study. In their patients with combined injuries to the PLC and ACL, regardless of other ligamentous injuries, PMTP bone bruising was reported in 17 of 58 (29.3%) patients. 11 Therefore, the aforementioned authors inferred that the presence of a PMTP bone bruise may act as a secondary sign of a potential combined PLC injury in the setting of ACL rupture. In the present study, 11 of 18 (61.1%) patients with combined PLC injuries and ramp lesions had PMTP bruises. These findings may expand our understanding of the bruise patterns reported by Geeslin and LaPrade 11 and should be confirmed in future studies.
It is important to note that nearly all the ramp lesions (17 of 18 [94%]) reported in our combined PLC injury cohort had ACL involvement (ACL-PLC or ACL-PCL-PLC). While ramp lesions in combined PLC injuries are most likely the result of ACL involvement, another consideration of this study was the presence of ramp lesions in combined PLC injuries without ACL involvement. Only one patient with a PCL-PLC injury had evidence of a ramp lesion on MRI. While this patient did have a PMTP bone bruise, we are unable to draw any conclusions in this combined PLC injury because of limited numbers. Geeslin and LaPrade 11 reported 5 patients who sustained isolated PLC or combined PCL-PLC injuries that had evidence of a PMTP bone bruise, but the presence or absence of ramp lesions was not reported. Future higher-powered studies are needed to assess ramp lesions and PMTP bone bruises in isolated and combined PLC injuries without ACL involvement.
Limitations
The current study has several limitations. First, given its retrospective nature, this study is susceptible to selection bias. In addition, the patients used in this study had heterogeneous combined PLC injuries, which makes it difficult to study a specific type of combined PLC injury. Second, ramp lesions were diagnosed on MRI and not through arthroscopic exploration. 7 Therefore, it is possible that the reported prevalence of ramp lesions (n = 18; 26.5%) in the current study may be an underestimate of the true frequency, although this is impossible to confirm without arthroscopic exploration. Additionally, these injuries were retrospectively analyzed over a 20-year period, and the presence and arthroscopic exploration of ramp lesions have only recently become of interest to the sports medicine community. Finally, bone bruise patterns reported in this study can be difficult to accurately localize on MRI. We qualitatively described the location of the bruises and did not record the signal intensity quantitatively. Bone bruise patterns can be misinterpreted or heal when the time between injury and MRI is delayed, typically after 6 weeks; however, we sought to obviate this limitation by including only those patients with an MRI performed within a 30-day time period from the date of injury. Similar to the diagnosis of ramp lesions, the methodology utilized for bone bruises sought to reduce any bias by including strict guidelines and mapping techniques and resulted in excellent interobserver reliability for the location and presence of PMTP bone bruises.
Conclusion
Preoperative medial meniscal ramp lesions were diagnosed on MRI in 26.5% of patients with acute grade 3 combined PLC injuries. PMTP bone bruising was significantly associated with the presence of a ramp lesion in patients. These findings reinforce the need to assess for potential ramp lesions at the time of multiligament reconstruction.
Footnotes
Final revision submitted July 26, 2022; accepted September 13, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.E.J. has received grant support and education payments from Arthrex. M.J.A. has received education payments from Arthrex, consulting fees from DePuy, and speaking fees from Arthrex. R.F.L. has received consulting fees from Arthrex and Smith & Nephew, speaking fees from Smith & Nephew, and royalties from Arthrex and Smith & Nephew. M.J.M. has received consulting fees and speaking fees from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Yale University (protocol ID 2000028578).