
Abstract
Background:
The standard radiographic view for diagnosing acromioclavicular joint (ACJ) dislocations is the Zanca view of both shoulders to assess superior displacement of the distal clavicle by measuring the coracoclavicular distance (CCD) and comparing it with the uninjured shoulder; however, there is no consensus on a gold standard for diagnostic measures to classify acute ACJ injuries.
Purpose:
To compare the CCD from an upright chest radiograph with a standard Zanca view of both shoulders in patients with an ACJ dislocation.
Study Design:
Cohort study (diagnosis); Level of evidence, 3.
Methods:
We reviewed the records of 70 patients with an ACJ dislocation between 2010 and 2021 who had both an upright chest radiograph and a Zanca view. An ACJ dislocation was classified as low grade (Rockwood types 1-3) or high grade (Rockwood type 5). The CCD was measured on the upright chest radiograph and the Zanca view by 2 independent reviewers, and the percentage of the CCD difference compared with the unaffected side (ΔCCD) was calculated and compared between the upright chest radiograph and the Zanca view. Interrater and intrarater reliability were determined using the intraclass correlation coefficient.
Results:
Included were 70 patients (55 male and 15 female; mean age, 46 years). There were 29 patients (41.43%) with a low-grade injury and 41 patients (58.57%) with a high-grade injury. In the overall analysis, the ΔCCD on the upright chest radiograph and Zanca view was significantly different (130.25% ± 88.42% vs 152.69% ± 106.56%, respectively; mean difference, 22.44% [95% CI, 2.40% to 42.48%]; P = .029). The subgroup analysis revealed that the ΔCCD on the upright chest radiograph and Zanca view was significantly different for patients with a low-grade injury (60.71% ± 25.79% vs 91.46% ± 68.54%, respectively; mean difference, 30.76% [95% CI, 7.18% to 54.33%]; P = .012) but not different for patients with a high-grade injury (179.45% ± 83.87% vs 196.00% ± 107.97%, respectively; mean difference, 16.56% [95% CI, –14.06% to 47.18%]; P = .281). The intraclass correlation coefficients for the ΔCCD measurements indicated good to excellent interrater and intrarater reliability.
Conclusion:
The study findings indicated that upright chest radiography can be used as a diagnostic screening tool for high-grade ACJ dislocations, but not for low-grade ACJ injuries, compared with the Zanca view.
Keywords
An acromioclavicular joint (ACJ) dislocation is a common shoulder injury, especially in young adults, and about 43% of injuries are sustained in the second decade of life. 15 Acute injuries of the ACJ may occur with other abnormalities, such as 18.2% of intra-articular injuries, superior labral anterior to posterior (SLAP) tears, and rotator cuff tears or 5.2% of bone fractures. 17 Currently, the treatment of ACJ dislocations is based on the severity of the injury according to the Rockwood classification 4 –6,12,19 : type 1, ACJ sprain; type 2, <25% coracoclavicular widening superiorly; type 3, 25%-100% coracoclavicular widening superiorly; type 4, posterior displacement; type 5, >100% coracoclavicular widening superiorly; and type 6, inferior displacement of the distal clavicle in relation to the acromion. Type 1 and 2 injuries are successfully treated nonoperatively, while the treatment for type 3 injuries is still controversial. 13,15 High-grade injuries (types 4-6) are commonly treated surgically. 13,15
The management of ACJ injuries depends on the severity of the injury based on a radiographic evaluation; thus, adequate imaging techniques and measurements are essential to establish the correct diagnosis and classification of an ACJ dislocation. ACJ stability can be classified into vertical and horizontal planes of instability. The common radiographic method to evaluate the vertical stability of the ACJ is the Zanca view with or without weightbearing 9,21 to assess superior displacement of the distal clavicle by measuring the coracoclavicular distance (CCD) and comparing it with the uninjured shoulder. Horizontal stability is still debatable as a suitable radiographic method of measurement. 8,11 There is no consensus on a gold standard for diagnostic measures to classify acute ACJ injuries. 16 Radiographic investigations include the standard anteroposterior (AP) view, transaxillary view of the affected shoulder, and Zanca view of both shoulders. Magnetic resonance imaging (MRI) can be useful for ligamentous and soft tissue structures. 6,18
An ACJ injury can be a concomitant or associated injury in patients with polytrauma or thoracoabdominal injuries. 1,2 Supine or upright chest radiography is the standard investigation tool that is used as an adjunct in the primary survey of patients with polytrauma. Chest radiography can detect bony injuries such as in the scapula, clavicle, and ribs or evaluate cardiopulmonary abnormalities. Also, chest radiography can observe distal clavicle alignment and ascertain ACJ abnormalities, especially upright chest radiography, which can use the arm’s weight similarly to the standard Zanca view of both shoulders.
The reliability of upright chest radiography to diagnose ACJ dislocations is still unknown; therefore, the purpose of the current study was to compare the CCD from an upright chest radiograph with a standard Zanca view of both shoulders in patients with ACJ dislocations. Our hypothesis was that upright chest radiography would be a useful imaging modality to determine the vertical instability of an ACJ dislocation compared with the standard Zanca view.
Methods
The study protocol received ethics committee approval. Patients with an ACJ dislocation at Thammasat University Hospital between 2010 and 2021 were retrospectively reviewed from medical records, operative notes, and radiographic and other imaging reports. Included were patients with an ACJ injury of all Rockwood types who had undergone upright chest radiography for any reason (eg, preoperative investigation, investigation of thoracic or chest injuries). Excluded were patients with open injuries; those <18 years; and those with bilateral ACJ dislocations, previous ACJ surgery, or associated fractures of the ipsilateral shoulder girdle.
The diagnosis of either an acute or chronic ACJ dislocation was based on clinical features (ACJ tenderness, ACJ deformity) and radiographic investigations (AP view, transaxillary view of affected shoulder, and Zanca view of both shoulders). The severity of the ACJ dislocation was classified as low grade (Rockwood types 1-3) or high grade (Rockwood type 5).
A radiological evaluation was performed with an upright chest radiograph and a Zanca view with the arm in adduction so that the bilateral CCD could be measured (Figure 1) . The images were reviewed on a picture archiving and communication system workstation. The CCD 3 was defined as the distance from the superior aspect of the coracoid vertically to the clavicle. In addition, the side-to-side difference in the CCD between the affected and unaffected shoulders (ΔCCD) was determined: ΔCCD (%) = [(Affected side CCD – Unaffected side CCD)/Unaffected side CCD] × 100. This ΔCCD was used to classify the grading of ACJ dislocations according to the Rockwood classification; a ΔCCD between 25% and 100% represented a type 3 injury, and a ΔCCD >100% represented a type 5 injury.

Coracoclavicular distance (CCD) measurement on (A) the Zanca view and (B) an upright chest radiograph. The CCD was defined as the distance from the superior aspect of the coracoid vertically to the clavicle (red arrow in the affected shoulder and yellow arrow in the unaffected shoulder).
There were 2 independent evaluators (T.C. and P.R., both orthopaedic sports medicine fellows) who evaluated the radiological parameters separately in all patients after practicing CCD measurements in 10 sample cases. The intrarater reliability was calculated, and the measurements were repeated 2 weeks after the first measurement to determine the interrater reliability.
Statistical Analysis
The sample-size calculation was based on a pilot study of 20 patients with ACJ injuries using the infinite population proportion (n4Studies). 14 With a proportion of high-grade ACJ of 0.5, an error of proportion of 0.15, and an alpha of .05, a sample size of least 43 patients was needed.
Categorical data (age, sex, affected side) were analyzed using the chi-square test of independence, and continuous data (ΔCCD) were analyzed using the paired t test. Interrater and intrarater reliability were calculated using the intraclass correlation coefficient (ICC), with ICC values interpreted as poor (<0.50), moderate (0.50-0.75), good (>0.75-0.90), and excellent (>0.90). 10 The threshold for significance was set at P < .05. Statistical analysis was performed using SPSS (Version 25; IBM).
Results
A series of 70 consecutive patients were included (55 male and 15 female; mean age, 46 years [range, 18-80 years]). Demographic data are shown in Table 1. There were 29 patients (41.43%) with a low-grade ACJ injury and 41 patients (58.57%) with a high-grade ACJ injury.
Demographic Data of Patients (N = 70) a
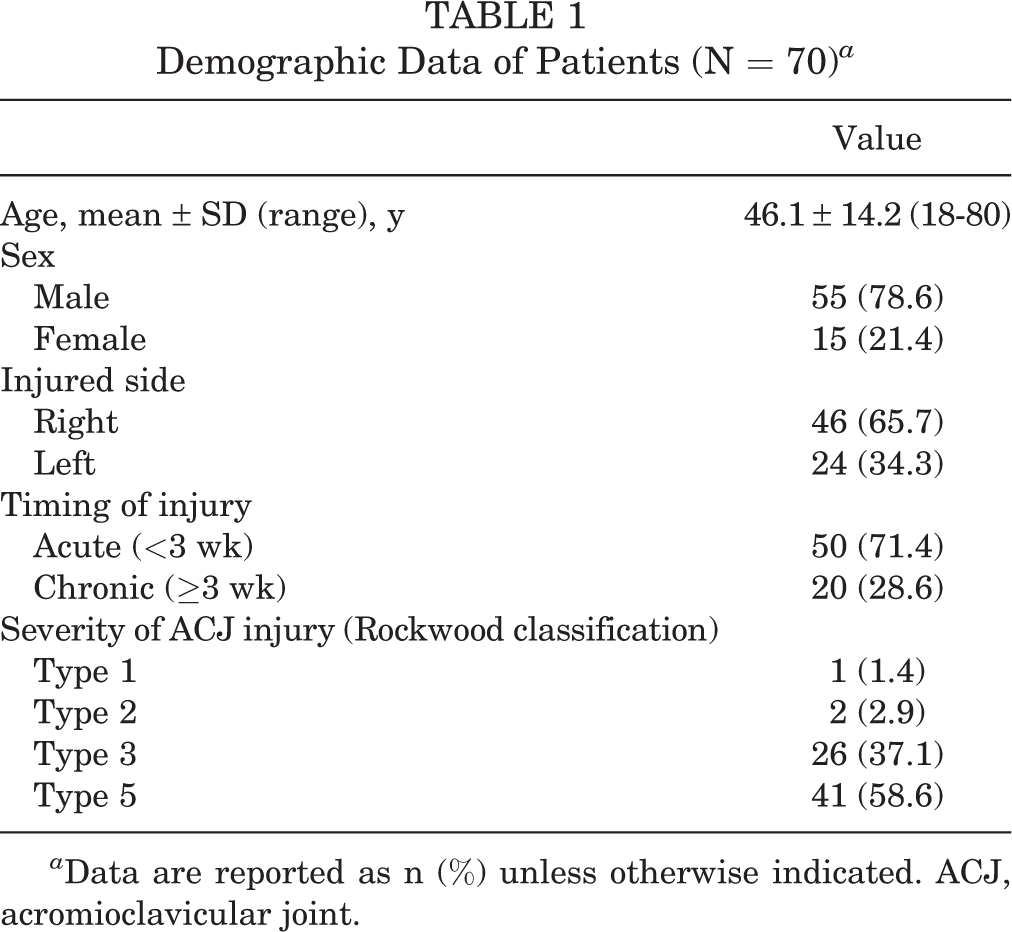
a Data are reported as n (%) unless otherwise indicated. ACJ, acromioclavicular joint.
Overall, the mean ΔCCD was significantly different between the radiographic views, with 130.25% ± 88.42% for the upright chest radiograph and 152.69% ± 106.56% for the Zanca view (mean difference, 22.44% [95% CI, 2.40% to 42.48%]; P = .029) (Table 2 and Figure 2). The subgroup analysis revealed significant differences between radiographic views in patients with low-grade injuries (ΔCCD: 60.71% ± 25.79% [upright chest] vs 91.46% ± 68.54% [Zanca]; P = .012) (Figure 3A); however, there were no significant differences in patients with high-grade injuries (ΔCCD: 179.45% ± 83.87% [upright chest] vs 196.00% ± 107.97% [Zanca]; P = .281) (Figure 3B).
ΔCCD According to Radiographic View a

a Data are reported as mean ± SD unless otherwise indicated. Boldface P values indicate a statistically significant difference between groups (P < .05). ACJ, acromioclavicular joint; ΔCCD, side-to-side difference in the coracoclavicular distance between the affected and unaffected shoulders.

Bland-Altman plot of the percentage of the side-to-side difference in the coracoclavicular distance as measured on an upright chest radiograph and the Zanca view. CXR, upright chest radiograph.
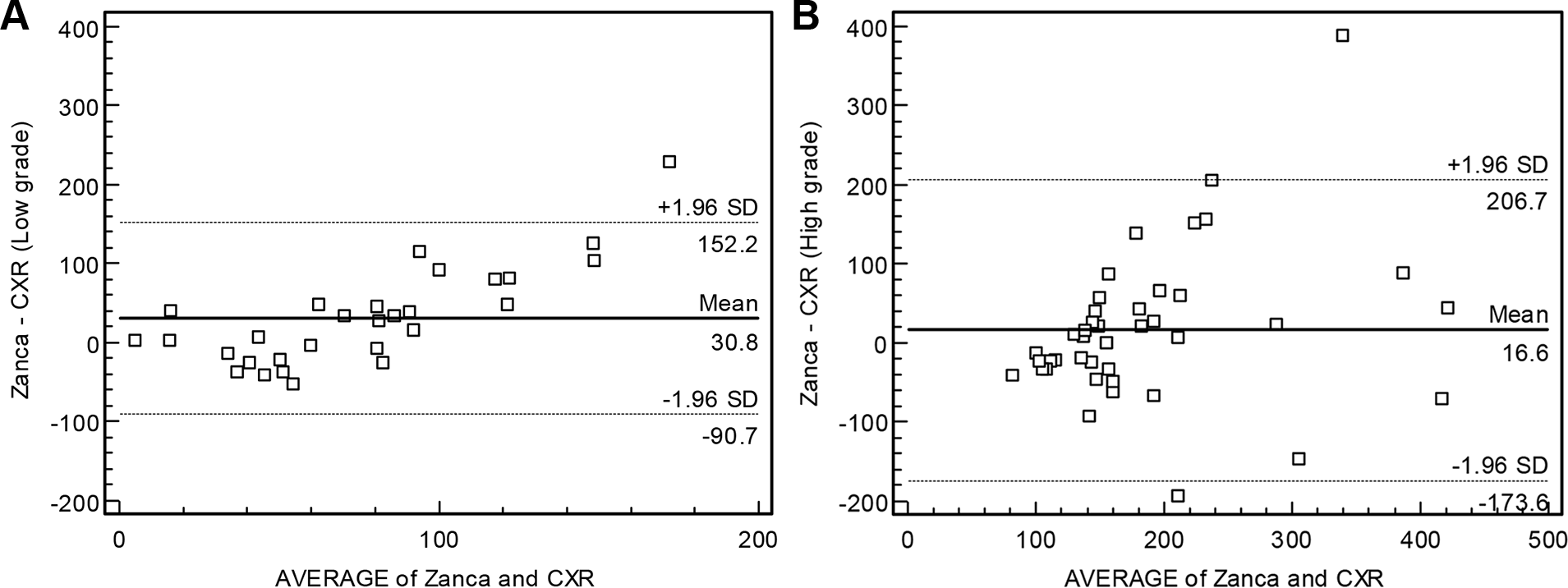
Bland-Altman plots of the percentage of the side-to-side difference in the coracoclavicular distance as measured on an upright chest radiograph and the Zanca view for (A) low-grade acromioclavicular joint (ACJ) dislocations and (B) high-grade ACJ dislocations. CXR, upright chest radiograph.
The ICC analysis revealed good to excellent interrater and intrarater reliability for the CCD measurements. The intrarater ICC was between 0.851 and 0.983, and the interrater ICC was between 0.926 and 0.928 (Table 3).
ICCs for Intrarater and Interrater Reliability of CCD Measurements a

a Data are reported as ICC (95% CI). CCD, coracoclavicular distance; ICC, intraclass correlation coefficient.
Discussion
The study findings indicated that the ΔCCD between the upright chest radiograph and Zanca view was significantly different in low-grade dislocations (Rockwood types 1-3; P = .012) and in the overall cohort (P = .029). Upright chest radiography was beneficial as a diagnostic tool in high-grade ACJ dislocations (Rockwood type 5) compared with the Zanca view, with a mean difference of ΔCCD of 16.56% (95% CI, –14.06% to 47.18%; P = .281). Our hypothesis was proved that an upright chest radiograph could detect the vertical instability of high-grade ACJ dislocations and might be useful to screen high-grade ACJ dislocations.
A recent systematic review 16 focused on which imaging modality should be used to accurately diagnose acute ACJ injuries. The authors included 17 studies that met the inclusion criteria for final analysis. Many imaging modalities were shown to diagnose ACJ injuries, such as the bilateral AP view, Zanca view, and weighted radiography as well as ultrasonography, computed tomography, and MRI. Still, there is no gold standard for diagnostic measures to classify acute ACJ injuries because of the heterogeneity of the literature. Plain radiography is generally preferred because of its availability and examiner independence. 16 A comprehensive review of ACJ injuries recommended that diagnostic imaging should begin with a shoulder series of radiographs (AP view, scapular Y-view, and axillary view), weighted radiographs, a cross-arm AP view, the Zanca view, or bilateral shoulder view. MRI is useful to detect intra-articular lesions (SLAP tears and rotator cuff tears), but it is not routinely performed. 3
Patients with polytrauma have a high prevalence of shoulder injuries of up to 28%, with 3% consisting of ACJ injuries, that are associated with severe thoracic injuries. 1,2 It is not uncommon that distracting pain or disability from injuries may lead to undetected shoulder or ACJ injuries. The Advanced Trauma Life Support guideline 7 suggests evaluating breathing using chest radiography but does not recommend the exact radiographic technique (either supine or upright). In an actual real-life situation, performing supine or upright chest radiography in patients with trauma depends on the patient’s condition. Upright chest radiography is one of the crucial investigation tools for diagnosing patients suspected of having thoracic or chest trauma. Upright chest radiography can detect pulmonary abnormalities, associated rib/scapular/clavicular fractures, or fractures around the shoulder girdle. CCD widening can be observed on chest radiographs, especially upright chest radiographs in patients with ACJ dislocations. No previous studies have mentioned the detection of ACJ dislocations on chest radiographs, and no study has examined the role of CCD measurements on chest radiographs compared with the standard AP or Zanca view of the shoulder in patients with ACJ dislocations.
This is the first study that has compared CCD measurements from an upright chest radiograph and the standard Zanca view of the shoulders. The CCD measurements showed reliability and relevance in patients with high-grade ACJ dislocations. Upright chest radiography may help to detect high-grade ACJ dislocations in patients. Early reconstruction of ACJ injuries of Rockwood types 3 to 5 showed better clinical results compared with delayed reconstruction 17 ; thus, an early diagnosis could be more beneficial than a delayed diagnosis. If we can diagnose a high-grade ACJ dislocation using upright chest radiography in patients with trauma, we would have another evaluation method to screen for ACJ injuries without the need for weightbearing radiographs. Weighted views of the ACJ have no influence on decision making regarding the treatment of low-grade ACJ injuries (Rockwood types 1-3). 20
Limitations
The limitations of this study have to be discussed. First, this study was focused on the vertical instability of ACJ dislocations instead of horizontal instability, which could be important in treating Rockwood type 3 and 4 injuries. Second, upright chest radiography is a static radiographic technique that could not detect dynamic instability of the ACJ. Third, although chest radiography is the primary investigational tool used in patients with polytrauma, supine chest radiography is more widely used than upright chest radiography. Upright chest radiography has more risk in patients with concomitant injuries such as spine fractures with spinal cord injuries or multiple fractures. Most upright chest radiographs in our patients were obtained preoperatively before the surgical management of ACJ injuries. Fourth, many chest radiographs, either upright or supine, do not adequately incorporate both shoulder joints. The evaluation of ACJ dislocations by upright chest radiography is limited to only chest radiographs that include both distal clavicles, the medial border of the acromion, and the coracoid process (as in Figure 2). Last, the accuracy of CCD measurements using an upright chest radiograph and the Zanca view to diagnose an ACJ injury was not evaluated in a population without an ACJ injury.
Conclusion
Upright chest radiography can be used as a diagnostic screening tool for high-grade ACJ dislocations, but not for low-grade ACJ injuries, compared with the Zanca view. The CCD measurements on the upright chest radiograph and Zanca view demonstrated reproducibility and reliability.
Footnotes
Acknowledgment
The authors thank the Department of Orthopaedics, Faculty of Medicine, Thammasat University and Thammasat University Hospital for their kind support. They also thank Dollapas Punpanich for statistical analysis as well as the editors and proofreaders for their assistance.
Final revision submitted September 20, 2022; accepted September 26, 2022.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Thammasat University Hospital (registration No. MTU-EC-OT-0-244/64).