
Abstract
Background:
There is limited research investigating the diagnostic strength of 3-dimensional computed tomography (3D-CT) and multidirectional CT arthrography (CTA) for femoroacetabular impingement (FAI) and related hip lesions.
Purpose:
To evaluate the diagnostic strength of combined 3D-CT and CTA in patients with FAI and related hip lesions by comparing it with hip arthroscopic surgery findings.
Study Design:
Cohort study (diagnosis); Level of evidence, 2.
Methods:
This study included patients who were suspected of having FAI and related hip lesions and who underwent a combination of 3D-CT and CTA and subsequent hip arthroscopic surgery between December 2013 and December 2017. The CT and intraoperative arthroscopic findings were recorded and compared. The sensitivity, specificity, and accuracy of 3D-CT for FAI and those of CTA for related hip lesions were calculated.
Results:
A total of 114 patients with 114 hips were included in our study. There were 101 patients with positive findings and 13 patients with negative findings for FAI (including cam, pincer, and combined morphology) according to 3D-CT. The sensitivity, specificity, and accuracy of 3D-CT for FAI were 91.58%, 57.14%, and 89.47%, respectively. The sensitivity, specificity, and accuracy of CTA for labral tears were 94.64%, 100.00%, and 94.73%, respectively. For acetabular cartilage defects, the sensitivity, specificity, and accuracy of CTA were 60.71%, 91.37%, and 76.31%, respectively. For femoral cartilage defects, the sensitivity, specificity, and accuracy of CTA were 82.22%, 76.81%, and 78.94%, respectively.
Conclusion:
The study results indicated that 3D-CT was able to provide excellent accuracy for FAI compared with hip arthroscopic surgery findings. In addition, multidirectional CTA demonstrated promising diagnostic strength for hip lesions such as labral tears and chondral defects.
Keywords
Femoroacetabular impingement (FAI) has been recognized as a potential precursor and a critical contributor to hip pain and hip osteoarthritis. 18 It may involve intra-articular lesions, such as cartilage damage and labral tears. 13 In addition to clinical symptoms and physical examination results, imaging is crucial for diagnosing FAI and related hip lesions. 1 Plain radiography in different views (anteroposterior [AP], Dunn, frog, false profile) is recognized as the modality of choice for the diagnosis of FAI, 4,30 while magnetic resonance imaging (MRI), magnetic resonance arthrography (MRA), and computed tomography (CT) arthrography (CTA) are used for diagnosing intra-articular lesions of the hip. 2,21,33 However, there is no consensus on which modality provides the best diagnostic strength for these abnormalities.
There is a paucity of literature reporting the diagnostic strength of 3-dimensional CT (3D-CT) for FAI and of CTA for soft tissue lesions. The purpose of the study was to evaluate the diagnostic strength of combined 3D-CT and CTA for FAI and related hip lesions by comparing it with hip arthroscopic surgery findings. Our hypothesis was that 3D-CT and CTA can provide helpful preoperative information with equal or better diagnostic strength in sensitivity, specificity, and accuracy for FAI and intra-articular lesions than traditional plain radiography and MRI.
Methods
Patient Selection
The study protocol was approved by the institutional review board of our institution. We retrospectively reviewed the records of 136 patients suspected of having FAI with associated soft tissue lesions who underwent 3D-CT and CTA of the hip between December 2013 and December 2017.
All patients with suspected FAI and intra-articular lesions were first diagnosed clinically at our outpatient department according to the patients’ symptoms, clinical signs, and physical examination results. The symptoms included pain in the deep hip or groin region that was motion or position related. The clinical signs from the physical examination included a clicking sensation with hip range of motion and deep hip pain on a hip impingement test with internal rotation of the hip in adduction and flexion. 25 If the patient presented with symptoms and clinical signs of FAI, plain radiography was performed (pelvis AP, pelvis frog). Cam-type FAI was suspected with the presentation of a pistol-grip deformity over the femoral head-neck junction in the pelvis AP view and an alpha angle >50° in the frog view, and pincer-type FAI was suspected with a lateral center-edge angle (LCEA) >39°, presentation of a posterior wall sign, presentation of a crossover sign, and an acetabular index ≤0° in the pelvis AP view. 36
If FAI was suspected from the clinical presentation and plain radiography, 3D-CT and CTA of the hip were arranged for a further evaluation and diagnosis. CTA was arranged in patients who were not allergic to contrast and who agreed to undergo the examination.
Patients having positive findings for FAI or hip lesions such as labral tears on 3D-CT were treated nonoperatively first (physical therapy for 3 months, lifestyle changes, and nonsteroidal anti-inflammatory drugs). Diagnosed patients were recommended to undergo hip arthroscopic surgery if nonoperative treatment failed. The failure of nonoperative treatment was defined as continuous pain or if patients were unable to live an active lifestyle.
Inclusion and Exclusion Criteria
The inclusion criteria for patient selection were as follows: patients diagnosed with FAI clinically, patients who underwent 3D-CT and CTA of the hip, and patients who underwent hip arthroscopic surgery afterward for further treatment. The exclusion criteria were as follows: patients who had undergone prior hip arthroscopic surgery, patients who were contraindicated to undergo CTA, and patients who did not undergo hip arthroscopic surgery (patients with severe osteoarthritis on CTA, patients with contraindications for hip arthroscopic surgery, patients lost to follow-up after nonoperative treatment). There were 4 patients who had undergone previous hip arthroscopic surgery, 8 patients did not undergo CTA, and 10 patients did not undergo hip arthroscopic surgery.
CTA Examination
Image Acquisition
Spiral CT was performed with a 256-slice multidetector CT system (Scenaria; Hitachi) using a soft tissue algorithm and slice thickness of 0.625 mm, pitch of 0.58, and reconstruction slice thickness of 2 mm without a gap (field of view of 120-140, 140 kV, 225 mAs) in axial, coronal, and sagittal planes, followed by reconstruction of surface-rendered images. Then, hip arthrography was performed using a 21-gauge needle under fluoroscopic guidance with an anterior approach lateral to the common femoral artery. Finally, 15 to 20 mL of a 3:1 mixture of iopamidol (iodine concentration of 300 mg/mL) and saline was injected, followed by CTA with the same machine and the same parameters except using a bone algorithm.
Image Analysis
Osseous abnormalities, labral tears, and chondral loss were analyzed independently by 1 of the 2 radiologists (C.J.F. and C.T.W.) with 15 and 17 years of experience in musculoskeletal radiology. For FAI, the interpretation criteria were based on the study conducted by Tannast et al. 36 On plain radiography, an alpha angle >50° in the Dunn view, a femoral head-neck offset <0.8 mm, or an offset ratio <0.18 all indicated cam-type morphology. On 3D-CT, cam-type morphology was defined as the presence of an osseous bump or a pistol-grip deformity over the femoral head-neck junction subjectively by the radiologists. An osseous bump was defined as osseous irregularity of the femoral neck that showed on both 3D-CT and 2-dimensional plain radiography. For pincer-type morphology, an LCEA >39°, an acetabular crossover sign or acetabular retroversion, a posterior wall sign, coxa profunda, or protrusio acetabuli on plain radiography and 3D-CT were indicated as positive findings. The LCEA on CT was measured in the coronal plane, independent of the patient’s position. The measurement of retroversion on 3D-CT was according to Dandachli et al. 11 A labral tear was defined as contrast extension into the body of the labrum on CTA of the hip. A labrum presenting with surface irregularity, fissuring, or fraying was also included. The location of the labral tear was determined by the clockface from the reconstructed sagittal view of the acetabular rim on CT images. Chondral defects were detected as the presence of a layer of fluid within the irregular space of the chondral region. Fluid between cartilage and the subchondral bone plate was also diagnosed as a chondral defect as initial cartilage delamination. 10,28 For ligamentum teres tears, the diagnosis protocol was as described by Cerezal et al. 7 Discontinuity of the ligamentum teres or edematous changes/fraying of the ligamentum teres on CTA was defined as a complete tear or partial tear of the ligamentum teres, respectively.
Surgical Procedure
Hip arthroscopic surgery was performed in patients placed in the supine position on a traction table specific for hip arthroscopic surgery. Traction was applied to the operative extremity, and hip joint distraction was confirmed fluoroscopy. If the joint space was not distracted adequately with a limited joint space for the needle to be placed intra-articularly, capsulotomy was performed before addressing the central compartment. Establishment of the portal and placement of the guide wire were conducted under fluoroscopy. During surgery, 2 or 3 portals were used, including anterior, anterolateral, and posterolateral portals. The central compartment was assessed, and labral or chondral damage was addressed if necessary. After the completion of central compartment management, traction was released, and the peripheral compartment was addressed.
Arthroscopic Assessment
In this study, we regarded intraoperative findings as the gold standard for diagnosing FAI, as in other studies. 15,30,35 Cam-type morphology was defined as the detection of an osseous bump over the femoral head-neck junction. After the identification of cam-type morphology, we performed a dynamic test of the hip from full extension to 80° of flexion, associated with internal rotation and external rotation, to check whether there was impingement of the labrum by the osseous bump. If the osseous bump impinged the labrum, cam-type FAI was diagnosed. Osteoplasty for cam impingement was performed by trimming the osseous bump in 45° of flexion with internal rotation for the lateral part and external rotation for the medial part. Pincer-type FAI was assessed by probing the acetabular rim. If there was significant osseous coverage over the acetabular rim associated with an intrasubstance labral tear, or if there was impingement of the labrum and cartilage delamination on the dynamic test, pincer-type FAI was diagnosed. Acetabuloplasty for suspected pincer-type morphology was performed by trimming excessive osseous acetabular coverage. All the arthroscopic surgical procedures were performed by, and intraoperative findings recorded by, 1 senior surgeon (Y.S.C.) who has 15 years of hip arthroscopic surgery experience, with around 70 cases per year and approximately 800 cases in total volume.
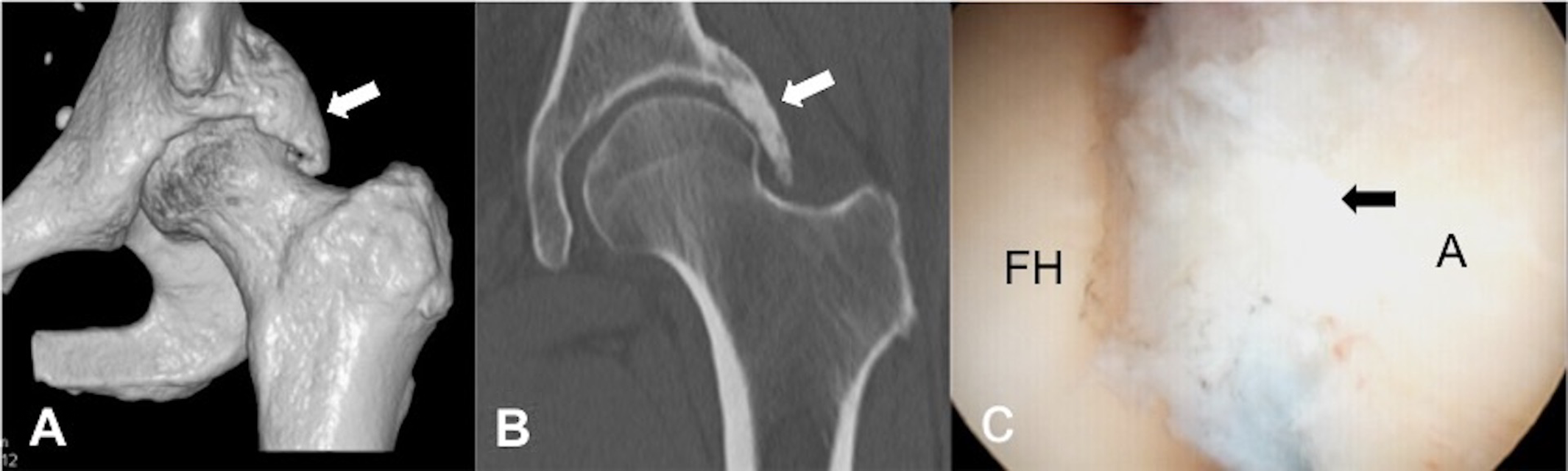
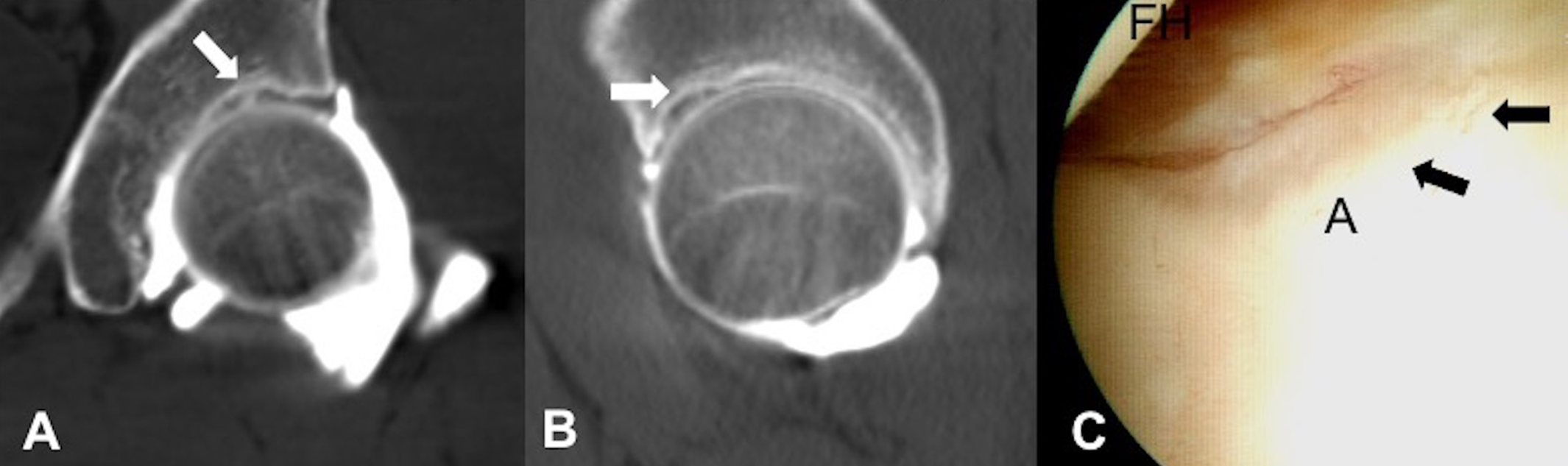
Examples of cam- and pincer-type FAI on CTA and 3D-CT and corresponding arthroscopic images are shown in Figures 1 and 2, respectively. Examples of labral tears, cartilage defects, and ligamentum teres tears on CTA and 3D-CT and corresponding arthroscopic images are shown in Figures 3, 4, and 5, respectively.

Images from a 36-year-old male patient diagnosed with cam-type morphology of the right hip with an osseous bump over the femoral head-neck junction: (A) 3-dimensional computed tomography (CT), (B) axial CT arthrography, and (C) arthroscopic examination. The cam lesion is indicated by an arrow in each image. A, acetabulum; FH, femoral head; FN, femoral neck.
Images from a 56-year-old female patient diagnosed with pincer-type morphology of the left hip: (A) 3-dimensional computed tomography (CT), (B) coronal CT arthrography, and (C) arthroscopic examination. The pincer lesion is indicated by an arrow in each image. A, acetabulum; FH, femoral head.

Images from a 39-year-old male patient diagnosed with a labral tear of the right hip with contrast invasion at the acetabulum-labrum junction: (A) coronal computed tomography arthrography (CTA), (B) axial CTA, and (C) arthroscopic examination. The labral tear is indicated by an arrow in each image. A, acetabulum; LB, labrum.
Images from a 22-year-old male patient diagnosed with an acetabular cartilage defect of the left hip with irregularity of the chondral region: (A) coronal computed tomography arthrography (CTA), (B) sagittal CTA, and (C) arthroscopic examination. The chondral defect is indicated by an arrow in each image. A, acetabulum; FH, femoral head.

Images from a 31-year-old male patient diagnosed with a ligamentum teres tear of the left hip with discontinuity of the ligamentum teres: (A) coronal computed tomography arthrography (CTA), (B) axial CTA, and (C) arthroscopic examination. The ligamentum teres tear is indicated by an arrow in each image. A, acetabulum; FH, femoral head; LT, ligamentum teres.
Statistical Analysis
Surgical and imaging findings correlated with arthroscopic results. A true-positive result for FAI or soft tissue lesions was defined as a positive finding on 3D-CT and CTA and confirmed by a subsequent arthroscopic examination. A true-negative result was defined as a negative finding on 3D-CT and CTA with a negative arthroscopic result. A false-positive result was defined as a hip lesion identified on 3D-CT and CTA that was unconfirmed by an arthroscopic examination, whereas a false-negative result was defined as a negative finding on 3D-CT and CTA but a hip lesion was identified during the arthroscopic examination. For example, if 3D-CT and CTA detected mixed-type morphology while hip arthroscopic surgery reported pincer-type FAI, the case would be considered as true positive for pincer morphology, owing to the detection of pincer lesions by 3D-CT, CTA, and arthroscopic surgery. On the other hand, the case would be regarded as false positive for cam lesions under the same scenario, owing to negative findings of cam morphology intraoperatively. The sensitivity of 3D-CT and CTA was defined as the percentage of hip lesions with an arthroscopically confirmed diagnosis by 3D-CT and CTA. The specificity of the examination was defined as the percentage of hip lesions not identified on 3D-CT and CTA and later confirmed by negative arthroscopic findings. The accuracy of the technique was defined as the percentage of hip lesions with a correct diagnosis by 3D-CT and CTA. The diagnostic strength of 3D-CT and CTA for the assessment of FAI and soft tissue lesions was calculated and analyzed accordingly.
To evaluate the reliability of 3D-CT and CTA findings, the images were reviewed by the other radiologist (C.J.F. or C.T.W.) to compare the results with initial reports. Kappa values (κ) were calculated to quantify the level of interobserver agreement and were interpreted according to Landis and Koch 19 as slight (0.00-0.20), fair (0.21-0.40), moderate (0.41-0.60), good (0.61-0.80), or excellent (0.81-1.00). The findings from the senior observer were used for statistical analysis with regard to surgical results. All statistical analyses were performed using SPSS for Mac (Version 23.0; IBM).
Results
Of the initial 136 patients, 114 patients (114 hips) were ultimately enrolled in the current study. There were 55 male and 59 female patients with a mean age of 42.6 years (range, 16-67 years). The total number of affected hips was 46 on the left and 68 on the right. The mean CT dose index volume and dose length product for the hip joint were 55.98 mGy (range, 53.52-56.52 mGy) and 689.8 mGycm (range, 630-730 mGycm), respectively.
The arthroscopic results are presented in Table 1. There were 107 patients (93.9%) diagnosed with FAI, 112 patients (98.2%) diagnosed with a labral tear, and 105 patients (92.1%) diagnosed with both. On the other hand, 64 patients (56.1%) had a chondral defect, and 25 patients (21.9%) had a ligamentum teres tear.
Hip Arthroscopic Findings (N = 114) a

a FAI, femoroacetabular impingement.
Disagreement between the 2 observers was recorded in 6 cases (5.3%) for cam-type morphology and 8 cases (7.0%) for pincer-type morphology. Regarding intra-articular lesions, disagreement between the 2 observers was recorded in 4 cases (3.5%), 9 cases (7.9%), 7 cases (6.1%), and 8 cases (7.0%) for labral tears, acetabular cartilage defects, femoral cartilage defects, and ligamentum teres tears, respectively. The interobserver reliability was good for FAI with cam lesions (κ = 0.80) and pincer lesions (κ = 0.85). For intra-articular lesions, the interobserver reliability was good for labral tears (κ = 0.73) and excellent for acetabular cartilage defects (κ = 0.82), femoral cartilage defects (κ = 0.87), and ligamentum teres tears (κ = 0.81).
There were 101 patients with positive findings and 13 patients with negative findings for FAI by 3D-CT. Of 101 patients diagnosed with FAI, 30 presented with the cam type, 3 presented with the pincer type, and 68 presented with the mixed type. The sensitivity, specificity, and accuracy of 3D-CT for the diagnosis of FAI were 91.58%, 57.14%, and 89.47%, respectively. The sensitivity, specificity, accuracy, positive predictive value, and negative predictive value of 3D-CT for detecting cam and pincer lesions are presented in Table 2.
Diagnostic Results for FAI by 3D-CT a

a 3D-CT, 3-dimensional computed tomography; FAI, femoroacetabular impingement; NPV, negative predictive value; PPV, positive predictive value.
There were 106 patients diagnosed with labral tears by CTA. All 106 patients diagnosed with labral tears by CTA had positive results from hip arthroscopic surgery, and no patient had an intact labrum. On the other hand, of 8 patients with negative findings of labral tears on CTA, 6 had positive findings and 2 had negative findings from hip arthroscopic surgery. The results showed 94.64% sensitivity, 100.00% specificity, and 94.73% accuracy of CTA for diagnosing labral tears.
For cartilage defects, 39 patients were diagnosed with acetabular chondral defects, and 53 patients were diagnosed with femoral chondral defects on CTA. In 39 patients diagnosed with acetabular cartilage defects on CTA, 34 patients had cartilage defects on hip arthroscopic surgery. Among 53 patients diagnosed with femoral cartilage defects on CTA, 37 patients presented positive findings of cartilage defects on hip arthroscopic surgery.
On CTA of the ligamentum teres, 24 patients were diagnosed with ligamentum teres tears, and 90 patients were diagnosed with an intact ligament. Hip arthroscopic surgery of 24 ligamentum teres tears diagnosed by CTA showed 15 tears and 9 intact ligaments.
The sensitivity, specificity, and accuracy of CTA for chondral defects and ligamentum teres tears compared with arthroscopic findings are shown in Table 3.
Diagnostic Results for Hip Lesions by CTA a

a CTA, computed tomography arthrography; NPV, negative predictive value; PPV, positive predictive value.
Discussion
The current study compared the results of 3D-CT and CTA with the findings of hip arthroscopic surgery. The sensitivity and accuracy of 3D-CT for the diagnosis of FAI were 91.58% and 89.47%, respectively. The sensitivity, specificity, and accuracy of CTA for labral tears were 94.64%, 100.00%, and 94.73%, respectively, and for cartilage defects, they were 60.71%, 91.37%, and 76.31%, respectively, in the acetabulum and 82.22%, 76.81%, and 78.94%, respectively, in the femoral head. We believe that the combination of 3D-CT and CTA is able to provide excellent predictive strength for FAI and related hip lesions.
3D-CT for FAI
Few studies have reported the efficacy of 3D-CT for FAI. Beaulé et al 5 reviewed 30 hips with FAI that underwent 3D-CT and concluded that 3D-CT is an accurate tool to quantify the femoral head-neck concavity related to cam-type FAI. Heyworth et al 15 conducted a study that assessed the preoperative 3D-CT images of 118 patients who underwent primary hip arthroscopic surgery. According to their results, patients who were diagnosed with cam-type FAI intraoperatively had 97% agreement with preoperative 3D-CT findings by radiologists. They found moderate agreement of 3D-CT findings with arthroscopic findings for cam-type lesions and concluded that the diagnostic assessment of patients with suspected FAI might be improved with the use of 3D-CT. Roling et al 31 reviewed 127 patients with FAI and compared the diagnostic strength of plain radiography and dynamic 3D-CT. According to their findings, the sensitivity and specificity of dynamic 3D-CT were 90% and 43%, respectively, for cam-type morphology and 84% and 51%, respectively, for pincer-type morphology. The results were consistent with those of our study, which reported a sensitivity and specificity of 3D-CT of 89.62% and 62.50%, respectively, for cam-type morphology and 86.48% and 49.35%, respectively, for pincer-type morphology. Similar to our study, they used intraoperative findings from hip arthroscopic surgery as the gold standard for the diagnosis of FAI. Although a previous study had defined FAI using objective parameters on both plain radiography and CT, 36 the intraoperative assessment of FAI has been used in recent literature. 22,31 Not only is the intraoperative diagnosis of FAI able to relate the impingement site to the region of the labral tear or chondral damage, 32 but a dynamic test intraoperatively could also assess impingement and therefore assist the operator with fewer measurements during fluoroscopy, as described by Locks et al. 22 A previous study reported that cam-type morphology had higher agreement between 3D-CT and intraoperative assessments than pincer-type morphology (κ = 0.48 vs 0.16, respectively). 15 This result might explain that the higher diagnostic strength of 3D-CT for cam lesions may be because of higher consistency between the radiologist and surgeon in our study.
Bony evaluations of pincer morphology are relatively difficult. A previous study reported limitations in the radiographic and surgical assessments of pincer morphology. 38 Heyworth et al 15 also reported inconsistencies in the evaluation of pincer morphology both on plain radiography and CT. Our study reported an accuracy of 61.40% and a specificity of 49.35% of 3D-CT for diagnosing pincer morphology. Pincer morphology can be categorized as focal or global types. 23 The focal type may present as anterior or posterior. Most focal-type pincer morphology is located at the anterolateral acetabulum region, causing anterior impingement. However, in cases regarding global types of pincer morphology or focal-type posterior pincer morphology, the pincer lesion may extend from the anterolateral to medial or posterior region of the acetabulum. In these particular cases, owing to the limited approach of hip arthroscopic surgery, the identification of the bony deformity around the acetabular rim is challenging. 3D-CT of the hip joint could, however, detect a more comprehensive bony structure, including focal- or global-type pincer morphology. Despite the detection of pincer morphology by 3D-CT, particular pincer morphology cases such as focal-type posterior pincer lesions or pincer lesions involving the medial site of the central compartment may not always result in impingement on dynamic tests during surgery, which might increase the number of cases with false-positive findings on 3D-CT. The above results explain the challenges in the diagnosis of FAI during arthroscopic surgery for pincer lesions and contributed to the low specificity (49.35%) and low positive predictive value (45.07%) of 3D-CT.
Although there might be difficulties during hip arthroscopic surgery in particular patients, and the operative diagnosis for the bony structure may not be completely comprehensive, the general results of the current study showed 91.58% sensitivity and 89.47% accuracy of 3D-CT for the diagnosis of FAI. We believe that 3D-CT provides sufficient information on the bony contour for the operator to perform treatment at suspected lesion sites.
CTA for Hip Lesions
Multidirectional CTA is known as a feasible tool for the detection of soft tissue lesions in the hip. Its spatial resolution provides excellent diagnostic strength in labral tears and chondral defects. 32
For evaluating the labrum, Christie-Large et al 10 conducted a retrospective study reviewing 96 patients who underwent multidirectional CTA with suspected labral tears. Among these patients, 27 underwent surgery, and the findings of CTA and surgery were compared and recorded. They demonstrated the excellent detection ability of CTA for labral tears with a sensitivity of 90%. Jung et al 16 performed a retrospective study reviewing 36 hips that underwent ultrasound and CTA and correlated the diagnosis of labral tears with arthroscopic findings. They revealed a sensitivity of 88% to 96% of CTA for labral tears with an accuracy of 89% to 94%. A systematic review with a meta-analysis conducted by Reiman et al 29 reported that CTA demonstrated the strongest overall diagnostic accuracy, with a pooled sensitivity of 91% and specificity of 89% for acetabular labral tears.
For chondral defects, the results from the literature varied. Christie-Large et al 10 reported the excellent diagnostic ability of multidirectional CTA, with 88% sensitivity and 100% specificity for acetabular chondral loss as well as 94% sensitivity and 100% specificity for femoral chondral loss. On the other hand, Lee et al 20 found that the sensitivity and specificity of CTA for detecting acetabular cartilage defects by both observers were 46% and 72%, respectively, and 64% and 72%, respectively.
The findings of the current study are in line with those of previous literature. The sensitivity, specificity, and accuracy of CTA for the detection of labral tears were 94.64%, 100.00%, and 94.73%, respectively. The results for cartilage defects were moderate. The sensitivity, specificity, and accuracy were 60.71%, 91.37%, and 76.31%, respectively, in the acetabulum and 82.22%, 76.81%, and 78.94%, respectively, in the femoral head.
The combination of 3D-CT and multidirectional CTA is thought to be a helpful examination tool for FAI and related hip lesions. 3D-CT provides the whole osseous contour of the hip joint, and multidirectional CTA presents different planes of view for soft tissue and cartilage lesions. Despite the promising diagnostic strength of CTA and the assistance of 3D-CT in preoperative evaluations, CT is still a concern regarding the risk of radiation exposure compared with nonradiation examinations, such as sonography or MRI/MRA. MRI/MRA lacks the risk of radiation exposure and is capable of analyzing quantitative bony morphology. However, a low relative proton density makes MRI less effective in the detection of cortical bone than CT.
Comparison of 3D-CT and Plain Radiography
Previously, FAI had been diagnosed using plain radiography. Different parameters and clinical signs were used to diagnose cam and pincer morphology, such as the alpha angle in the Dunn view, the LCEA, the crossover sign, and the posterior wall sign. 4,30 However, the Warwick Agreement has discussed the limitations of plain radiography in interpreting 3D morphology of the hip, while 3D reformatting of CT can identify morphological abnormalities in FAI. 14 Khan and Witt 17 used a 3D-CT model to measure cam deformities. They stated that the 2-dimensional image formation by plain radiography using a single alpha angle could not detect exact impingement, which was caused by an osseous bump at the femoral head-neck junction. 17 For pincer lesions, Cadet et al 6 conducted a study assessing the interobserver and intraobserver agreement of FAI parameters, comparing plain radiography and 3D-CT. They reported that 3D-CT demonstrated higher intraobserver agreement when determining the presence of a crossover sign. 6
Comparison of CTA and MRI/MRA
MRI and MRA are common radiological evaluation tools for soft tissue lesions such as labral tears and chondral defects of the hip. Both conventional 3.0- and 1.5-T MRI have been reported to be able to identify hip lesions such as labral tears and cartilage defects with moderate diagnostic strength. 3,24 A recent study found that conventional 3.0-T MRI is equivalent to 1.5-T MRA in detecting acetabular labral tears and is superior to 1.5-T MRA in detecting cartilage defects in patients with suspected FAI. 9 In previous studies, the sensitivity of MRA for diagnosing labral tears was between 83% and 100%, and for chondral defects, it was between 71% and 92%. 8,33 –35 However, limitations of MRI in the detection of small labral tears have been reported. 37 Some studies have also reported an equal or better sensitivity of CTA compared with MRA for the assessment of articular cartilage loss in the hip. The above findings may be attributed to superior spatial resolution of multidirectional CTA. 21,27
Christie-Large et al 10 suggested the superior ability of CTA over MRI to detect cartilage injuries and a similar sensitivity of CTA and MRI for the detection of labral tears. Lee et al 20 compared the accuracy of CTA and MRI by reviewing 36 hips diagnosed with hip lesions. They revealed a better accuracy of CTA over MRI for labral tears, with 86% to 89% for CTA and 64% to 69% for MRI. However, both CTA and MRI in diagnosing chondral defects demonstrated moderate diagnostic strength, with an accuracy of 64% to 69% for CTA and 69% to 75% for MRI in their study. Al-Saadawy et al 2 compared multidetector CTA and MRA for the detection of acetabular labral tears and articular cartilage defects in 61 patients. They defined the confirmation of a diagnosis as findings from MRA. The sensitivity and specificity were 90.7% and 100%, respectively, for the detection of acetabular labral tears, and the specificity was 95% and 100% for the detection of femoral and acetabular chondral defects, respectively, by multidetector CTA. They concluded that multidetector CTA might be an efficient alternative to MRA in the evaluation of hip lesions. Sahin et al 32 reported the excellent diagnostic ability of CTA for labral tears with 100% sensitivity, specificity, and accuracy, while MRA had 100% sensitivity, 50% specificity, and 86% accuracy for labral tears. However, MRA might be better in demonstrating acetabular and femoral cartilage defects, with a sensitivity, specificity, and accuracy of 89%, 40%, and 71%, respectively, for the acetabulum and 100%, 90%, and 86%, respectively, for the femoral head. The same values for CTA were 56%, 60%, and 71%, respectively, for the acetabulum and 75%, 70%, and 71%, respectively, for the femoral head. Comparing CTA with both MRI and MRA, Reiman et al 29 found a moderate increase in the probability of labral tears being found by CTA, whereas MRI/MRA presented positive findings with a minimal to small increase.
Our results demonstrated that the sensitivity, specificity, and accuracy of CTA for labral tears were 94.64%, 100.00%, and 94.73%, respectively. The sensitivity, specificity, and accuracy of CTA for cartilage defects were 60.71%, 91.37%, and 76.31%, respectively, in the acetabulum and 82.22%, 76.81%, and 78.94%, respectively, in the femoral head. The results were comparable with other studies in which the accuracy of CTA for labral tears was excellent and might be better than that noted in MRI/MRA studies. However, no articles thus far have provided strong evidence for the superiority of MRI, MRA, or CTA for cartilage defects. Our results support the capability of CTA for diagnosing labral tears. For cartilage defects, CTA is thought to be the imaging modality that provides moderate to good diagnostic accuracy.
According to our results and the literature review in the above 2 sections, we believe that 3D-CT, followed by contrast injection and CTA, is equal to or better than radiography and MRI for diagnosing various abnormalities in patients with FAI. 3D-CT provides better information on the impingement area in a different plane of the femoral head-neck junction than radiography, which is also not affected by the patient’s position when assessing pincer morphology. For soft tissue lesions, CTA had good diagnostic strength in chondral defects compared with MRI and an equal to better diagnostic strength in labral tears compared with MRI.
Ligamentum Teres Tears
With the increased use of hip arthroscopic surgery, the ligamentum teres has gained much interest in recent years, and there is a better understanding of its biomechanical function and roles in the hip. 26 Devitt et al 12 reported the capability of MRI for diagnosing injuries of the ligamentum teres. Cerezal et al 7 reported that CTA and MRA have a better diagnostic accuracy than conventional MRI. Our results demonstrated 89.88% specificity and 83.33% accuracy of CTA for detecting ligamentum teres tears. Although there is no consensus on the gold standard examination for ligamentum teres tears, CTA showed moderate accuracy for the detection of this abnormality.
Limitations
There are limitations of this study. First, this is a retrospective study with a moderate sample size. Second, patients in this study underwent an examination before surgery, and this fact might have influenced the intraoperative assessment of the operator. Third, the diagnosis of FAI on 3D-CT was subjectively made by radiologists. Although there was an accompanying measurement on 2-dimensional imaging, and the interobserver reliability was calculated with excellent agreement, an objective measure for FAI on 3D-CT would strengthen the reliability. Finally, the intraoperative diagnosis of FAI remains controversial. The diagnostic confirmation of FAI by hip arthroscopic surgery was relatively subjective, and the intraoperative assessment was challenging at times, especially in particular pincer morphology cases.
Conclusion
Our study results indicated that 3D-CT was able to provide excellent accuracy in FAI compared to hip arthroscopic surgery findings. In addition, multidirectional CTA demonstrated promising diagnostic strength in hip lesions such as labral tears and chondral defects. We believe that the combination of 3D-CT and multidirectional CTA is a promising examination method for assessing patients with FAI and related hip lesions.
Footnotes
Final revision submitted September 9, 2022; accepted September 15, 2022.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Chang Gung Medical Foundation (No. 202100717B0).