
Abstract
Background:
In previous studies examining the relationship between graft size and failure rate after anterior cruciate ligament reconstruction (ACLR), graft size was determined as diameter of the bone tunnel, and graft failure was defined as revision surgery. Consequently, the correlation between graft size and postoperative recurrent instability could not be assessed.
Purpose:
(1) To intraoperatively measure the cross-sectional area (CSA) of the hamstring tendon (HT) autograft and compare the CSA of the autograft with the bone tunnel and (2) to assess the effect of the graft CSA on postoperative graft failure among patients who underwent double-bundle ACLR.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
The study included 129 patients who underwent double-bundle ACLR using an HT autograft (mean ± SD age, 16.7 ± 1.7 years; all with a Tegner activity level ≥6). All patients had a minimum follow-up of 2 years. During surgery, the graft CSA was measured using an area micrometer, combining the anteromedial (AM) and posterolateral (PL) grafts. The total area of the bone tunnel was defined as the combined CSAs of the AM and PL tunnels as calculated by the diameter of the drill. The relationship between the CSAs of the combined HT graft and the bone tunnel was statistically compared, as was the relationship between graft CSAs and graft failure, defined as reinjury, recurrent instability manifested as quantitative laxity measurement, or revision ACLR.
Results:
The CSAs of the midsubstance of the combined AM and PL graft significantly correlated with those of the bone tunnels (femoral side, R 2 = 0.334, P < .0001; tibial side, R 2 = 0.421, P < .0001). As for the relationship between the graft CSA and ACLR failure, there was no significant difference in the graft CSAs between the groups with and without graft failure in any of the failure criteria (P = .188).
Conclusion:
The graft CSA was not a predictor of early failure after double-bundle ACLR using an HT autograft in this patient population.
Anterior cruciate ligament (ACL) reconstruction (ACLR) using an autogenous tendon graft is a standard procedure for the active patient population with ACL insufficiency subsequent to injury. There have been a number of studies examining factors that potentially influence the surgical outcome. 7,15,27 Among those factors, the size of the graft is regarded as an important determinant for properties of the reconstructed ACL, and the size of the hamstring tendon (HT) autograft has been shown to significantly correlate with the rate of revision 7,16,17,21,25 –27,29,30 ; however, there are some potential shortcomings in the design and contents of those previous studies.
According to previous cadaveric studies on the geometry of the native ACL along the length, the cross-sectional area (CSA) at the midsubstance ranged from 30 to 53 mm2 while its area at the insertion site was substantially larger, presenting an hourglass shape. 6,9 In previous studies examining the effect of graft size on the surgical outcome, the graft CSA was not directly measured, and the diameter of the bone tunnel (drill) derived from a graft sizer measurement was regarded as the graft size. 16,17 In addition, the previous large cohort studies adopted revision ACLR as a definition of graft failure, 16,17,25,26 but some patients would have been reluctant to undergo revision surgery even if instability recurred. Therefore, the effect of the graft CSA on the surgical outcome may not have been critically assessed with an analytic design employed in those relevant studies. Moreover, single-bundle ACLR was performed in the patient population of those studies, and relevant data for the double-bundle reconstructive procedure have not been reported.
In the present study, we intraoperatively measured the CSA of the HT autograft using an area micrometer in patients who underwent double-bundle ACLR to examine the correlation between the graft CSA and the bone tunnel, as well as the effect of graft CSA on postoperative graft failure. We hypothesized that the total bone tunnel CSA would correlate with the graft CSA and there would be no significant correlation between graft CSA and graft failure.
Methods
Study Design and Population
This study was approved by our institutional ethics review board, and informed consent was obtained from all patients. This study was conducted at a single hospital that specializes in knee surgery. For this retrospective study, we initially enrolled 237 consecutive patients aged <20 years who underwent primary double-bundle ACLR with an autogenous HT tendon between January 2011 and December 2015. Exclusion criteria were as follows: a low preinjury activity level (Tegner activity scale ≤5), concomitant ligament reconstruction procedures, ACLR for nonunion after tibial eminence fracture, ACL augmentation for partial tear, and discontinuation of participation in consistent sports activity after ACLR. Of the 208 patients who met the inclusion criteria, 79 were lost to follow-up, leaving a final study population of 129 teenaged athletes (Tegner activity scale ≥6). The process of patient selection is shown in Figure 1.

Flowchart of the patient selection process. ACL, anterior cruciate ligament; TAS, Tegner activity scale.
Surgical Procedure
All ACLR procedures were performed with the patient under general anesthesia by 2 senior authors (A.M., M.Y.). The HT was harvested and prepared into 2 double-stranded tendon grafts for each of the anteromedial (AM) and posterolateral (PL) bundle grafts. Considering the difference of the intra-articular length between the AM and PL bundles, the graft for the AM bundle was prepared 10 mm longer than that for the PL bundle. 18 Although the graft was prepared from the semitendinosus tendon alone in the majority of cases, the gracilis tendon was additionally harvested for preparation of the PL bundle graft in case the harvested semitendinosus tendon was ≤23 cm long or the tissue quality was deemed to be insufficient for its isolated use.
After arthroscopic intra-articular surgery such as meniscal repair, femoral and tibial bone tunnels were drilled via the outside-in technique with diameters corresponding to graft sizes. The femoral AM and PL tunnels were placed behind the resident’s ridge under arthroscopic control, while the locations of the tibial AM and PL tunnels were determined utilizing the remnant footprint and anterior horn of the lateral meniscus as landmarks. For graft fixation, EndoButton CL (Smith & Nephew Endoscopy) was used on the femoral side. The length of the EndoButton CL was determined to preserve the tendon graft end >10 mm within the femoral bone tunnel. On the tibial side, braided polyester or high-strength sutures were placed at the graft end via the Krackow whipstitch technique and tied to the post screw (6.5-mm cancellous screw; Arthrex Japan). During graft fixation to the tibia, manual maximum tension was applied to the AM bundle graft at 20° of knee flexion and to the PL bundle graft at 0°. A supplemental lateral extra-articular procedure was not performed in any of the cases.
Intraoperative CSA Measurement
CSA of the HT graft was measured at the midportion of the graft. To measure the total CSA of the midsubstance of the graft, the AM and PL bundle grafts were combined, and the midsubstance of the combined graft was placed in the oblong-shaped slot in a custom-made area micrometer (MEIRA). As described in previous reports, this device is designed to apply constant contact pressure (0.12 MPa) during measurement (Figure 2). 5,10,14,19 After 1 minute of compressive load application, the area of the combined tendon was calculated. The graft was kept moist before and during the measurement. The measurement accuracy and reliability of this device were confirmed by a previous study. 8

Intraoperative measurement of the cross-sectional area of the hamstring tendon graft. The anteromedial and posterolateral grafts are combined and placed in the oblong-shaped slot that is designed to apply constant contact stress (0.12 MPa) during the measurement.
Calculation of the CSA of the Femoral and Tibial Bone Tunnels
The area of the bone tunnel was defined as the combined area of the AM and PL bone tunnels calculated by the diameter of the drill used. As the cross section of the bone tunnel was round, the following formula was used to calculate the CSA of the combined AM and PL bone tunnels:

Postoperative Rehabilitation and Return to Sports Activity
The operated knee was immobilized for 1 week after surgery, and range of motion exercises were initiated thereafter. Partial weightbearing was allowed at 1 week with progression to full weightbearing at 4 weeks. For the knees with concomitant meniscal repair, the period of immobilization and nonweightbearing was extended an additional week. Jogging and running were initiated at 3 and 4 months, respectively. To evaluate the recovery of strength and functional performance, limb symmetry index values were calculated for isokinetic dynamometer quadriceps strength (Biodex Medical Systems), and results of the functional tests were evaluated (eg, single-leg hop test). Once limb symmetry index values >85% were achieved in muscle strength and functional tests, sport-specific activity was initiated. After acquisition of landing, cutting, and sport-specific skills, patients were allowed to return to sports without restriction. Return to sports was defined as the time from surgery to when patients could participate in all training programs or play in games.
Clinical Outcomes
All patients were followed up at 6 months, 12 months, and biannually or annually thereafter for a minimum of 2 years after surgery. Clinical data relevant to reinjury and revision ACLR were obtained from the patient’s record. For the stability assessment, anterior knee laxity was quantitatively measured at the maximum manual force with the KT-1000 arthrometer (MEDmetric Corp) at every postsurgical evaluation.
The criteria for ACLR failure were defined by 3 conditions: reinjury (major giving way with subsequent swelling and increased laxity), residual or recurrent instability manifested by KT-1000 arthrometer side-to-side difference (SSD) ≥3 mm, and revision ACLR. Diagnosis of reinjury was based on clinical symptoms, subsequent physical examination, and magnetic resonance imaging. When any of these 3 conditions were met, the reconstructed ACL was deemed a failure. In analyzing the effect of the graft CSA on subsequent graft failure, the patients were divided into groups with and without failure, and their difference in CSA was statistically assessed.
Statistical Analysis
Continuous variables were expressed as mean and standard deviation, and the intergroup difference was analyzed using the Welch t test or the Wilcoxon rank-sum test. The normality of data distribution was evaluated using the Shapiro-Wilk test. Categorical characteristic variables were compared with the Fisher exact test. Pearson correlation coefficients and linear regression equations were used for correlation assessment. All statistical analyses were performed with the significance level set at P < .05, and JMP (Version 14.0.2; SAS Institute Inc) was used for the analysis.
Results
Patient Demographics
The demographics and clinical profiles of the 129 study patients are shown in Table 1. The mean ± SD age of the participants was 16.7 ± 1.7 years, and the mean time between surgery and follow-up was 41.2 ± 17.7 months (range, 24-105 months). The sports activities among this population are shown in Table 2.
Characteristics of the Study Patients Versus Initial Population a

a Values are expressed as No. or mean ± SD (range). AM, anteromedial; NA, not applicable; PL, posterolateral.
Sports Activities of the Study Participants (N = 129)

CSA of the HT Graft and the Bone Tunnel
The mean intraoperative CSA of the midsubstance of the combined AM and PL graft was 35.9 ± 5.0 mm2, and the mean combined area of the AM and PL bone tunnels was 41.1 ± 3.0 mm2 and 49.0 ± 5.4 mm2 on the femoral and tibial sides, respectively. The graft CSA was calculated as follows: –3.55 + (0.96 × area of femoral tunnel) and 6.37 + (0.6 × area of tibial tunnel).
The CSA measured in the graft was significantly smaller than the combined CSAs of the AM and PL bone tunnels on the femoral and tibial sides (P < .0001). The intraoperative CSA of the graft closely correlated with the area of the femoral bone tunnel (R 2 = 0.334; P < .0001) as well as the tibial bone tunnel (R 2 = 0.421; P < .0001) (Figure 3).
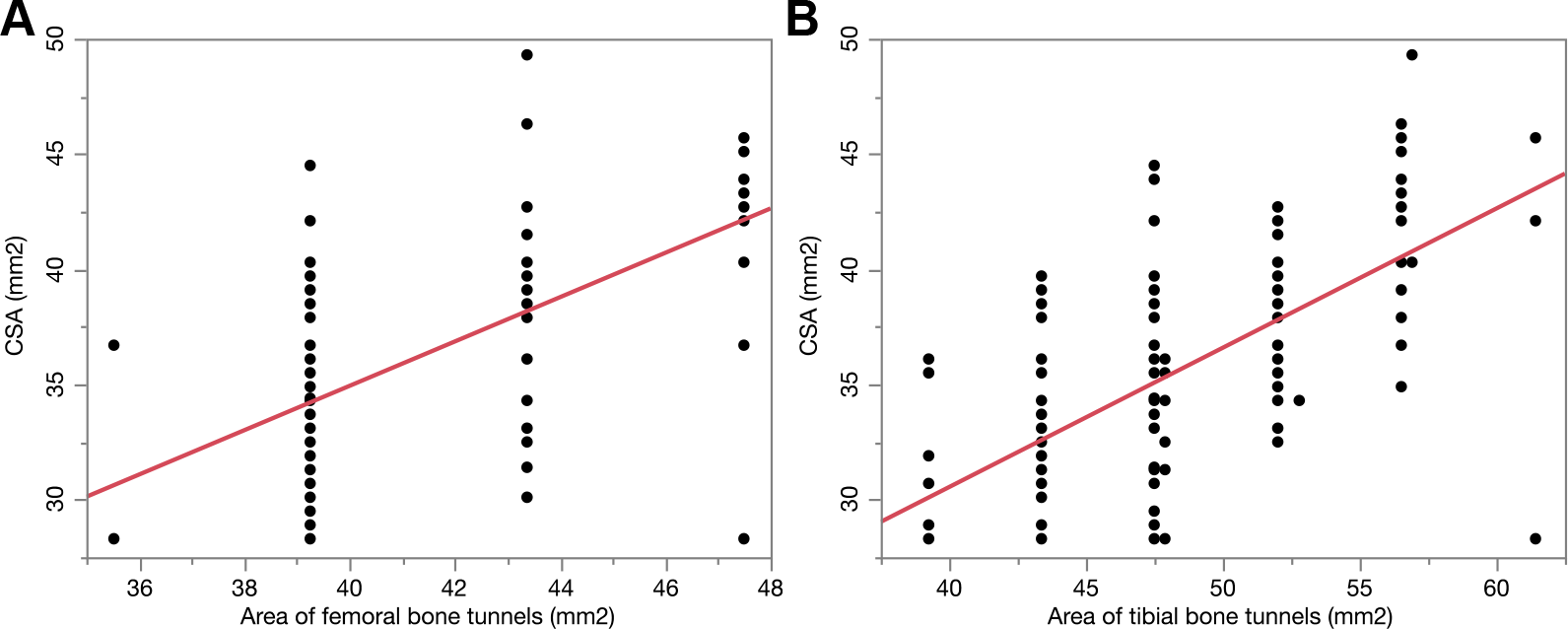
Correlations between the cross-sectional area (CSA) of the midsubstance of the combined hamstring tendon graft and (A) the total area of the femoral bone tunnels (R 2 = 0.334; P < .0001) and (B) the total area of the tibial bone tunnels (R 2 = 0.421; P < .0001).
Relationship Between Graft Size and Graft Failure
During the follow-up period, 22 patients sustained reinjury, 9 exhibited recurrent or residual instability during KT-1000 arthrometer measurement (excluding those sustaining reinjury), and 18 eventually underwent revision ACLR. Based on the failure criteria in this study (ie, meeting ≥1 of the 3 failure conditions), 31 (24.0%) of the 129 ACLRs were considered failures. Comparisons of demographic and clinical characteristics between the patients with and without graft failure did not demonstrate a significant difference, except for larger height and body weight values in the graft failure group (Table 3). When the graft CSA values were compared between the groups with and without graft failure, no significant difference in CSA value of the combined HT graft was seen between the groups (Table 4).
Characteristics Between the Failure and Nonfailure Groups a
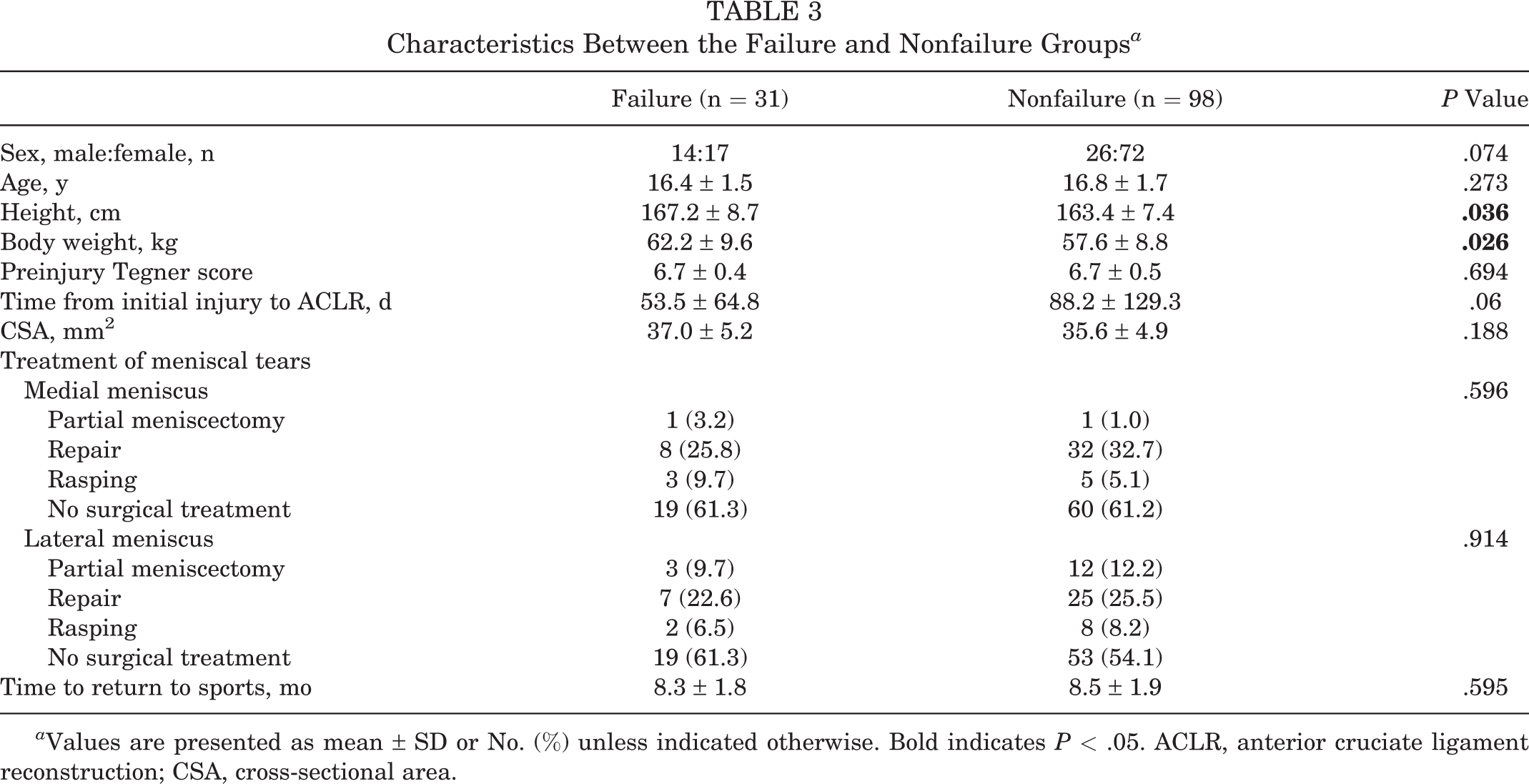
a Values are presented as mean ± SD or No. (%) unless indicated otherwise. Bold indicates P < .05. ACLR, anterior cruciate ligament reconstruction; CSA, cross-sectional area.
CSA of the Midsubstance of the Hamstring Tendon Graft Between the Groups With and Without ACLR Failure a
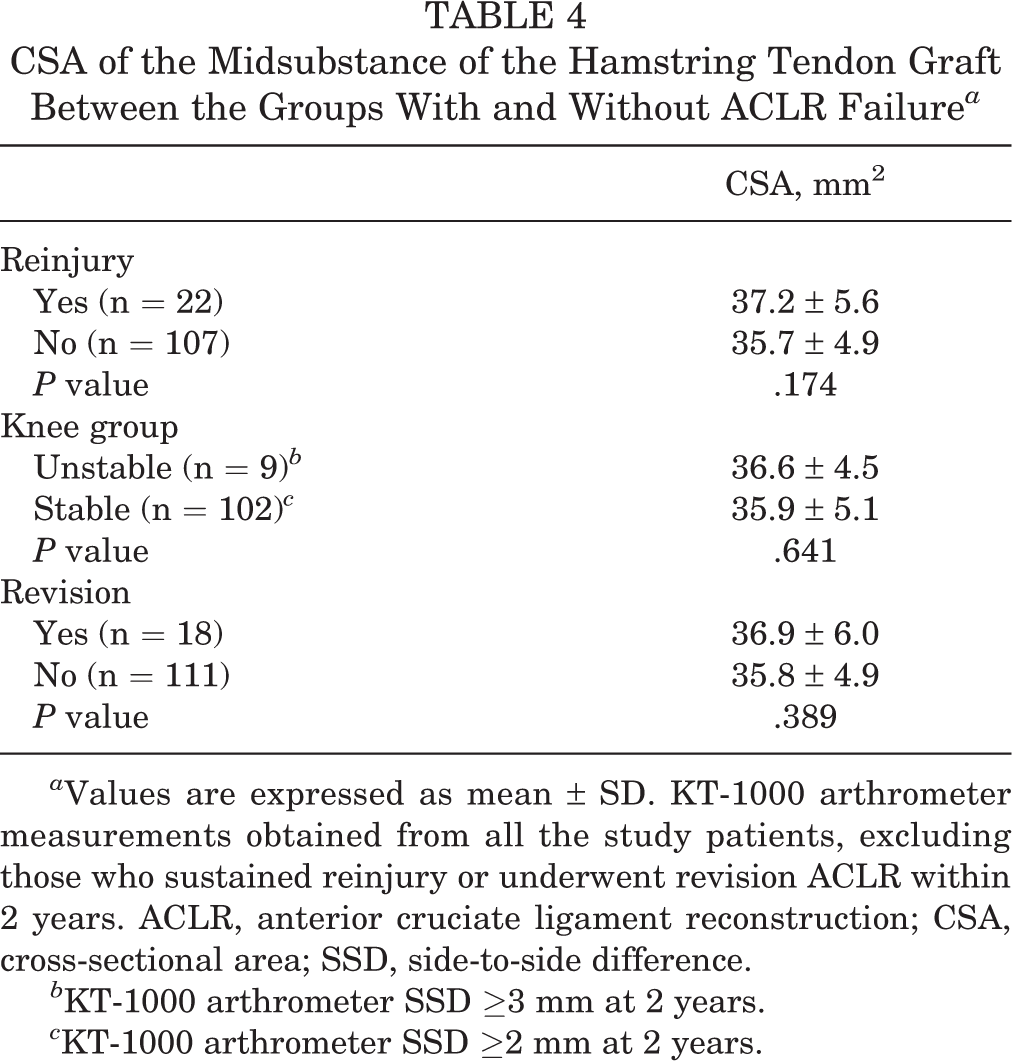
a Values are expressed as mean ± SD. KT-1000 arthrometer measurements obtained from all the study patients, excluding those who sustained reinjury or underwent revision ACLR within 2 years. ACLR, anterior cruciate ligament reconstruction; CSA, cross-sectional area; SSD, side-to-side difference.
b KT-1000 arthrometer SSD ≥3 mm at 2 years.
c KT-1000 arthrometer SSD ≥2 mm at 2 years.
The postoperative period for the KT-1000 arthrometer measurement ranged from 24 to 105 months (mean, 41.2 months). The KT-1000 SSD laxity values at 2 years and final follow-up (before any reinjury or revision ACLR) averaged 0.8 ± 1.0 mm (range, –1 to 4 mm) and 0.9 ± 1.1 mm (range, –1 to 4 mm), respectively. In 9 knees defined as graft failure attributed to increased laxity (SSD ≥3 mm) during the study period, instability became apparent by 12 months in 5 knees and by 24 months in all cases. No significant correlations were noted between the CSA of the HT graft and the SSD in laxity at 2 years (Figure 4).

Correlations between the cross-sectional area (CSA) of the midsubstance of the hamstring tendon graft and KT-1000 arthrometer side-to-side difference (SSD) with maximum manual force at 2 years (R 2 < 0.001; P < .879).
Discussion
This study demonstrated that the intraoperatively measured CSA of the midsubstance of the HT graft was smaller than the area of the femoral and tibial bone tunnels (approximately 87% and 73% of the area of bone tunnels, respectively). In the analysis of the effect of the graft CSA on postoperative graft failure and knee stability, graft size was not shown to be a predictor of early graft failure in our patient population that underwent double-bundle HT autograft ACLR.
It has been generally thought that graft size is an important, influential factor in surgical outcomes. 3,24 There have been several studies of a large patient population showing that small graft size is a predictor of revision ACLR attributed to early graft failure. 7,16,17,21,25 –27,30 In general, a diameter of 8 mm is regarded as a critical cutoff value associated with a higher revision rate. 16,20 By contrast, a few studies have shown that the size of the HT autograft does not influence the graft failure rate. 12,29 Therefore, somewhat discordant results have been reported on the relationship between graft size and survival rate, and the effect of graft size on graft failure in ACLR has not been well clarified in previous literature.
In the majority of those previous relevant studies, there are some shortcomings in the analytic design. First, graft size was determined by measurement using a graft sizer, which measures the thickest part of the graft, and the diameter value of the bone tunnel was used as a parameter for graft size. Second, revision ACLR was counted as graft failure, and all patients with reinjury or recurrent instability were not in the analysis unless they underwent revision ACLR. Therefore, in the present study, CSA of the midsubstance of the HT graft was directly measured using an area micrometer, and knees with postoperative reinjury and recurrent anterior instability were also counted as graft failure.
In the assessment of graft failure after ACLR, a higher incidence of ipsilateral graft tear was reported in younger athletes, especially in adolescents, 1,27,30 while results on the relationship between graft diameter and clinical outcomes in previous large cohort studies were derived from the analysis on patient populations including adults with a relatively low risk of reinjury. 25,26 To evaluate the effect of graft CSA on ipsilateral tear in a patient population with a high risk of reinjury, only teenaged patients with Tegner activity level ≥6 were subjected to analysis in this study. The reported reinjury rate for ACLR in a young active patient population ranges from 9% to 25%. 2,11,15,22 Thus, the reinjury rate of 17% during a 41.2-month follow-up period in the present study is comparable with that in previous relevant studies.
Another issue regarding the relationship of initial graft size and surgical outcome is a change in graft morphology after surgery during its healing and remodeling process. 4,14 Kinugasa et al 14 reported that the CSA of the HT graft increased to 134% within a year and decreased gradually to 117% around 3 years during the remodeling-to-maturation process. Yet, an oversized graft may cause impingement between the graft and the intercondylar notch or posterior cruciate ligament, leading to inferior graft healing. 20
The present study results do not show a significant association of small graft size with postoperative failure. The discrepancy between the present and aforementioned study results may stem from the differences in the method of CSA measurement, the definition of graft failure, and reconstructive procedures (single- vs double-bundle reconstruction). In the patient population selected for the present study analysis, the CSA of the HT graft did not influence the surgical outcomes, and it is thought that augmentation by other graft materials may not be required even when the harvested HT autograft seems small in diameter.
Limitations
We recognize several limitations in this study. First, the CSA of the HT autograft might vary depending on multiple factors, such as patient race, sex, and physical characteristics; however, those demographic and constitutional characteristics were not adopted as factors conjointly influencing graft failure in the analysis of this study. There have been studies reporting that anthropometric characteristics such as height are strong predictors of graft diameter. 13,21,23,28 Given the physical characteristics of Japanese teenagers, the mean CSA of the HT autograft in the present study might be smaller than that of skeletally matured Western patients. Second, only graft failure was adopted as an outcome measure, while clinical measures such as International Knee Documentation Committee and Lysholm scores were not in the analysis.
As a third limitation, the CSA of the HT graft in this study was measured at the midportion of the combined AM and PL grafts using an area micrometer. Although the accuracy and reliability of area micrometer measurements were confirmed in a previous in vitro study, 8 there are some sources of error, such as the time of compressive load application and the time from graft harvest and measurement. Furthermore, after graft implantation, the graft CSA changes over time owing to tension creep and subsequent tissue remodeling. In addition, the implanted AM and PL bundle grafts run 3-dimensionally and move dynamically during knee motion. Therefore, the graft CSA in intraoperative measurement may not represent the size of the reconstructed ACL in vivo. Fourth, the CSA of the femoral and tibial graft ends was not measured using an area micrometer. Especially in regard to the size of the tibial bone tunnel, the CSA in this study was assessed with the suture materials placed at the graft end. Fifth, the graft size was measured with a custom-made area micrometer, and the diameter measurement for the combined graft using a graft sizer was not conducted. The lack of data on graft sizer measurement of composite grafts makes it difficult to discuss the results of this study in comparison with related studies that used a graft sizer.
Last, we acknowledge that the present study was relatively short term and about 40% of the patients were lost to follow-up. Although no significant differences in demographics were present between the patient groups after exclusions for clinically relevant criteria and the final study population, there is a concern for a transfer bias. Therefore, further long-term evaluations with a higher follow-up rate are required to more accurately investigate the effect of the intraoperative CSA of the graft on clinical outcomes.
Conclusion
Graft CSA was not a predictor of early failure after double-bundle ACLR using an HT autograft in this patient population. Further study with prospectively collected data, longer follow-up, and additional outcome metrics is essential to make a definitive statement.
Footnotes
Acknowledgment
The authors acknowledge Rebecca Imaizumi for her assistance in editing the English of this article.
Approval for this study was provided by the institutional ethics review board (No. 2020-3) at Meiwa hospital.
Final revision submitted July 31, 2022; accepted September 13, 2022.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.