
Abstract
Background:
Single-row (SR) and double-row repair techniques have been described to treat rotator cuff tears. We present a novel surgical strategy of arthroscopic-assisted mini-open repair in which a locking-loop suture bridge (LLSB) is used.
Purpose:
To compare the functional outcomes and repair integrity of LLSB technique to the SR technique for arthroscopic-assisted mini-open repair of small to medium rotator cuff tears.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Included were 39 patients who underwent LLSB repair (LLSB group) and 44 patients who underwent SR suture anchor repair (SR group) from 2015 to 2018. We evaluated all patients preoperatively and at 3, 6, 12, and 24 months postoperatively using the visual analog scale (VAS) for pain, Oxford Shoulder Score (OSS), and American Shoulder and Elbow Surgeons (ASES) score. Also, shoulder sonography was performed at 12 months postoperatively to evaluate repair integrity using the Sugaya classification system. The independent-sample t test was used to analyze functional outcomes (VAS, OSS, and ASES scores), and the Fisher exact test was used to analyze postoperative sonography results.
Results:
Patients in both the LLSB and SR groups saw a significant improvement on all 3 outcome measures from preoperatively to 24 months postoperatively (P < .001 for all). However, when comparing scores between groups, only the scores at 3 months postoperatively differed significantly (VAS: P = .002; OSS: P < .001; ASES: P = .005). Shoulder sonography at 12 months postoperatively revealed no significant difference in repair integrity between the LLSB and SR groups (retear rate: 10.26% and 6.82%, respectively; P = .892).
Conclusion:
Better outcome scores were seen at 3-month follow-up in the LLSB group, with no difference in retear rates compared with the SR group at 12 months postoperatively. The LLSB technique was found to be a reliable technique for rotator cuff repair of small- to medium-sized tears.
Keywords
Rotator cuff disease is a common cause of shoulder pain. 42,45 Rotator cuff repair is currently among the most performed shoulder surgical procedures, 19 and its incidence is rising rapidly. 11,46 Techniques for rotator cuff repair have evolved from open techniques to arthroscopically assisted mini-open techniques and all-arthroscopic techniques, 8 and suture anchors are currently the most commonly used implants in rotator cuff repair. Suture anchor repair can primarily be divided into single-row (SR) or double-row techniques; these 2 types of techniques have constituted the basis for various other techniques such as the modified Mason-Allen suture bridge technique, knotless suture anchor technique, transosseous tunnel technique, 7 and cruciate ligament repair techniques. 31 Compared with SR or double-row techniques, these modified techniques can enhance restoration of the footprint contact area and pressure. 6
The senior author (P-.W.W.) has performed a novel modified arthroscopic-assisted mini-open technique called locking-loop suture bridge (LLSB) repair, which is based on the knotless suture anchor technique, 31 and compared its outcomes with those of SR repair. We assumed that the proposed LLSB technique could provide superior restoration of the footprint contact area and pressure, similar to double-row repair, as this technique is a type of the modified Mason-Allen suture bridge technique. However, it requires the same number of suture anchors as SR repair, making it economical.
Therefore, the purpose of our study was to introduce a novel LLSB technique, which combines the benefits of both SR and double-row repair in that it has satisfactory clinical outcomes and depends on only 1 or 2 suture anchors, offering more surgical options for both surgeons and patients. We hypothesized that this technique would show positive clinical outcomes with repair integrity and high patient satisfaction.
Methods
Study Design
After receiving institutional review board approval (No. N202004066), we collected the data of patients who had undergone a surgical intervention for a rotator cuff tear at our hospital between January 1, 2015, and December 31, 2018, and had a follow-up period of ≥24 months (mean, 27.6 months [range, 24-30 months]). A total of 83 patients were included in this prospective cohort study. Inclusion criteria were as follows: (1) being aged between 40 and 80 years, (2) having a full-thickness supraspinatus or infraspinatus tendon tear of a small to medium size (tear diameter <3 cm; DeOrio and Cofield 13 classification), (3) having grade 1 or 2 retraction (Patte 37 classification), and (4) having fatty degradation of grade 1 or 2 (Goutallier classification 17 ) on magnetic resonance imaging (MRI). The exclusion criteria were as follows: (1) undergoing combined type 2 superior labral anterior to posterior (SLAP) repair, (2) having a complete rupture of the subscapularis tendon, (3) having neurological involvement, (4) undergoing a revision procedure, (5) having a partial-thickness rotator cuff tear progress to a full-thickness lesion, (6) having advanced arthritic changes in the glenohumeral joint, or (7) having not fully repairable tears.
Surgical Technique
After receiving a clear explanation of the 2 types of surgical techniques, including the difference between suture anchors (knot-tying suture anchor for SR repair and knotless suture anchor for LLSB repair) and fixation methods, the patients selected the type of technique. In total, 39 patients underwent LLSB repair (LLSB group), and 44 patients underwent SR suture anchor repair (SR group), all performed by a single experienced surgeon (P-.W.W.) using the arthroscopic-assisted mini-open technique.
Patients underwent surgery under general anesthesia in the beach-chair position. Standard arthroscopic portals were created: posterior, lateral, and anterior portals. By first entering from the posterior portal, we conducted an arthroscopic examination of the glenohumeral joint. The arthroscope was then transferred to the subacromial space. In all patients, a clear angle and image were obtained through a radiofrequency device. After performing debridement using a mechanical shaver and radiofrequency device, the rotator cuff was cleaned to provide full visualization of the rotator cuff tear. In addition, acromioplasty was performed in all participants with a bur to create a wider space during rotator cuff repair. Procedures on the biceps tendon were performed in cases of partial tears, subluxations, and complete dislocations. Tenotomy was performed in patients aged >55 years, and tenodesis was performed in patients aged ≤55 years. When necessary, biceps tenodesis was performed with one of the anterior suture anchors above the rotator cuff. After arthroscopic debridement and arthroscopic acromioplasty using the mini-open technique, the deltoid muscle fibers were reached by widening the lateral portal toward the acromion’s anterolateral corner. The fibers of the deltoid muscle were split through blunt dissection, and maximal visualization was established using a soft tissue retractor. Care was taken to avoid damaging the axillary nerve running close to the distal edge of the incision and to minimize detachment of the deltoid muscle fibers from the lateral part of the acromion. SR repair was performed using 1 or 2 knotted suture anchors (5.5-mm titanium Corkscrew FT II suture anchor; Arthrex) and simple stitches.
For LLSB repair in this study, the entrance stitch began from the inferior edge of the torn tendon and exited on the superior surface (Figure 1A). A throw was then created horizontally from the superior to inferior surface of the tendon (Figure 1B). The needle was passed from the inferior to superior medial edge to the throw that was just created (Figure 1C). The needle was next shifted to the other end of the stitch, and the entire process was repeated (Figure 1D), creating a locking loop (Figures 1E and 2A). When the suture was completed, a knotless suture anchor (4.75-mm PEEK [Polyetheretherketone] SwiveLock C anchor with blue FiberTape Loop; Arthrex) was used to fix the stitch (Figure 2, B and C).

Locking-loop suture bridge technique. (A) The entrance stitch began from the inferior edge of the torn tendon and exited on the superior surface. (B) A throw was then created horizontally from the superior to inferior surface of the tendon. (C) The needle was passed from the inferior to superior medial edge to the throw that had just been created. (D) The needle was then shifted to the other end of the stitch, and the entire process was repeated. (E) Completed locking-loop suture bridge repair.

Locking-loop suture bridge technique. (A) Locking-loop suture bridge repair on tendon edge. (B) Application of a knotless suture anchor. (C) Final repair construct.
The number of anchors to utilize was decided during surgery in both groups. At the site of mini-open repair, the subcutaneous layer was closed with inverted 4-0 absorbable, braided sutures and covered with Steri-Strip skin closures (3M). The portals were closed in a similar fashion.
Rehabilitation
All patients followed the same rehabilitation protocol. Patients wore a shoulder sling for 4 weeks postoperatively. Mobilization exercises commenced on day 1. Removal of the sling was allowed for bathing and dressing, and active finger, wrist, and elbow motion and periscapular strengthening were encouraged. At 1 to 4 weeks, passive external rotation with the arm at the side was limited to 0°, and passive flexion or abduction was limited to 90° while wearing the sling. The sling was discontinued at 4 weeks after surgery, and active-assisted range of motion exercises were performed at 4 to 8 weeks, progressing to full motion at 8 to 12 weeks. Advanced strengthening exercises began at 12 weeks to gradual full release.
Preoperative and Postoperative Evaluations
Functional scores and the shoulder structure were evaluated both preoperatively and postoperatively. Functional scores included the Oxford Shoulder Score (OSS), the visual analog scale (VAS) for pain, and the American Shoulder and Elbow Surgeons (ASES) score. Postoperative evaluations were conducted at 3, 6, 12, and 24 months. For the structural evaluation, MRI and sonography were performed preoperatively. Sonography was conducted at 12 months after surgery to evaluate the shoulder structure using the Sugaya classification system, 43 which is validated for sonography based on research by Barth et al 4 and Collin et al. 10 All evaluations except for sonography were performed and recorded by the same clinical research nurse. Sonography was performed by an experienced rehabilitation physician (H-.C.C.) using a transducer (12-MHz PLT-1204 BT linear transducer with Aplio 300; Toshiba). During sonography, the patients were seated with the affected arm hanging free by the side of the trunk. The rotator cuff repair site was examined in 3 planes: axial, sagittal, and coronal. The tendons of the supraspinatus and infraspinatus were examined with the arm in adduction and internal rotation. The integrity of the repaired rotator cuff was classified into 5 types as described by Sugaya et al 43 based on frontal, sagittal, and transverse sonographic images only. The sonographic examiner was blinded to the results of the functional outcomes, and the clinical examiner was blinded to the results of shoulder sonography.
Statistical Analysis
The functional outcomes (VAS, OSS, and ASES scores) were assessed using continuous variables, which are presented as the mean with standard deviation; the differences in outcomes between patients in the LLSB group and those in the SR group were analyzed using an independent-samples t test. The Fisher exact test was used to analyze postoperative sonography results, which were assessed using categorical variables presented as percentages. Differences were considered significant when P < .05. Data were processed and analyzed using R 3.5.2 (R Core Team).
Results
A total of 83 patients participated in the study, 39 of whom were in the LLSB group and 44 were in the SR group (Figure 3). In each shoulder, the preoperative tear size was measured by a probe during arthroscopic surgery according to the DeOrio and Cofield classification 13 and classified as small (<1 cm) or medium (1-3 cm). The tear pattern of either crescent shaped (short and wide) or longitudinal (long and narrow) 12 was examined by a grasper and then recorded. Patient demographics and tear characteristics are summarized in Table 1.
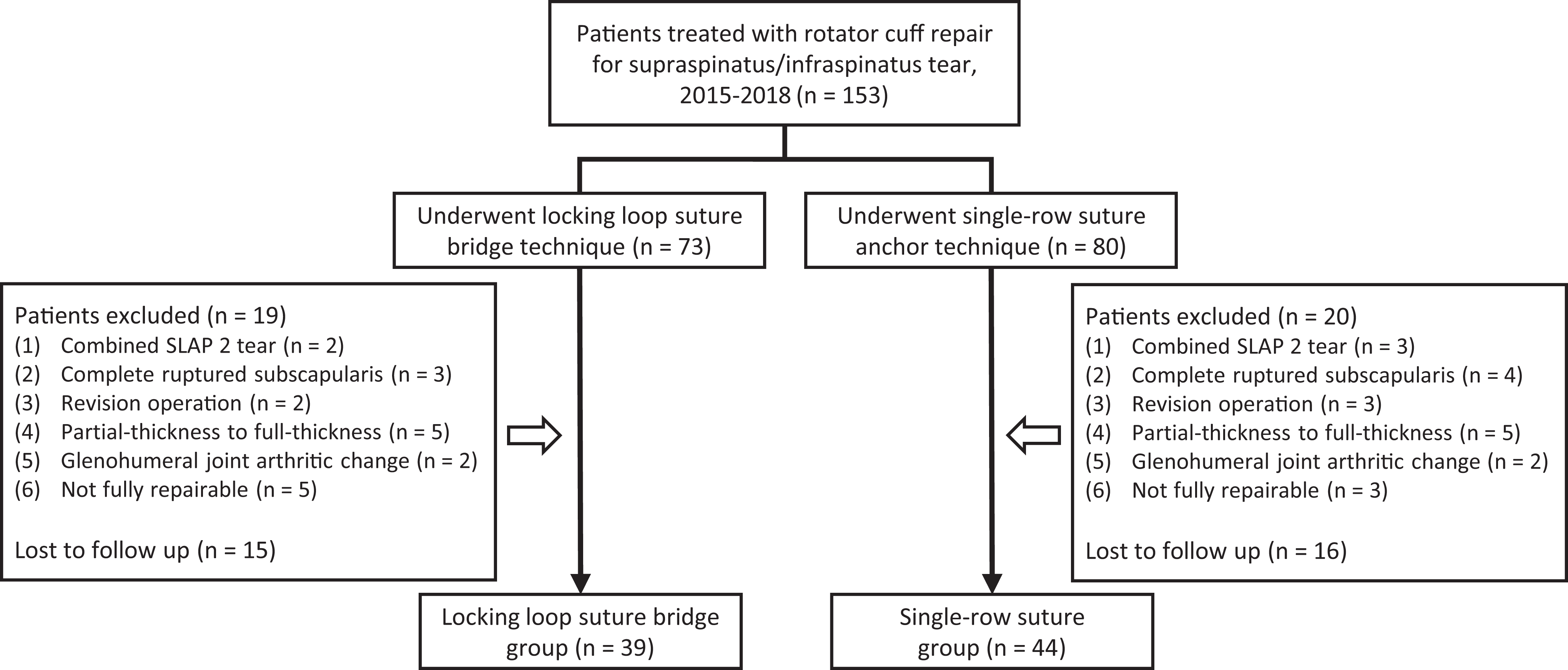
Strengthening the Reporting of Observational Studies in Epidemiology patient flowchart. SLAP, superior labral anterior to posterior.
Patient and Tear Characteristics a

a Data are reported as mean ± SD or n (%). LLSB, locking-loop suture bridge; SR, single-row suture anchor.
b Values were analyzed using the Student t test for continuous variables.
CThe chi-square test for categorical variables for which there is no standard deviation.
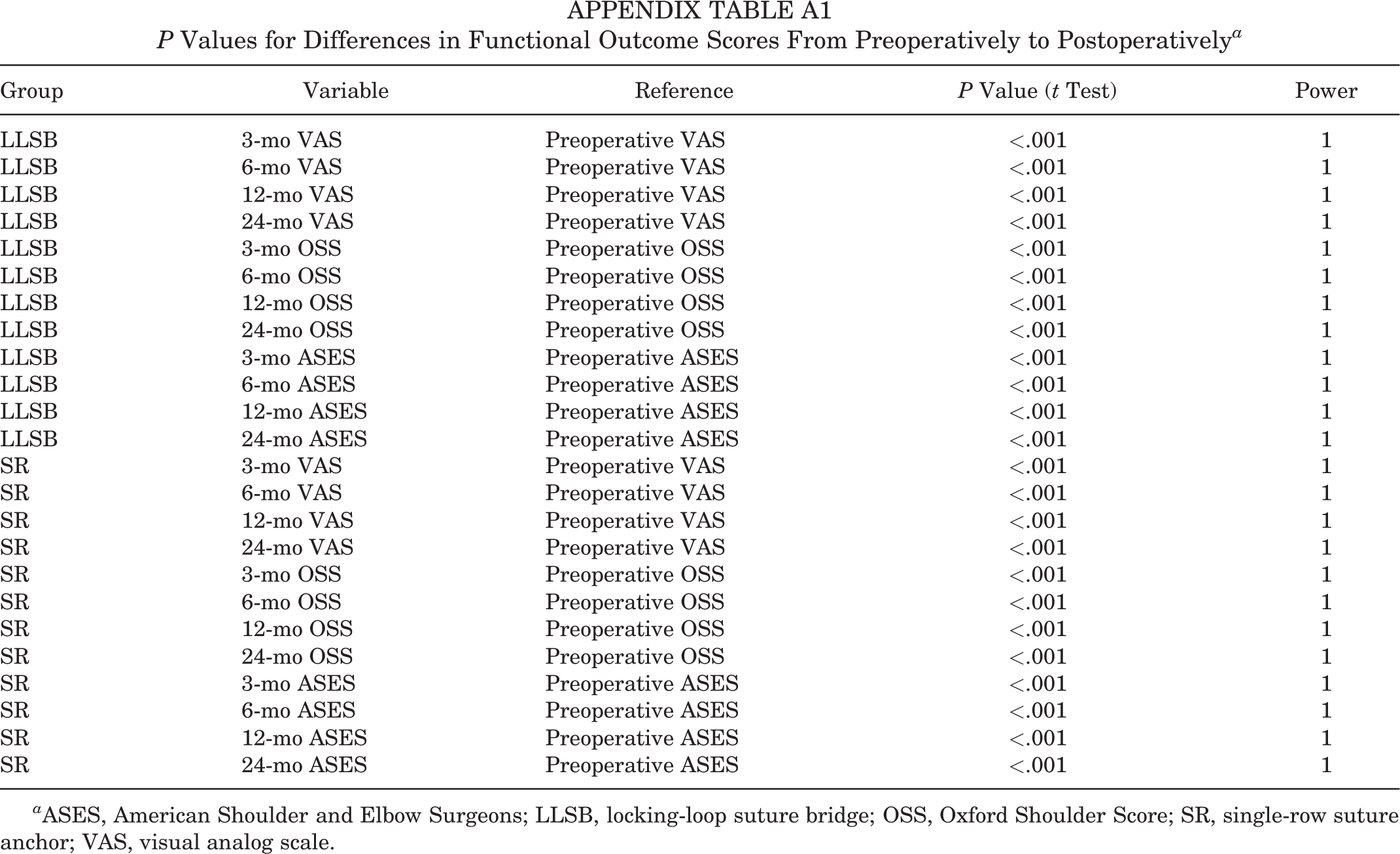
At all 4 postoperative time points, the VAS, ASES, and OSS scores improved significantly compared with preoperatively (P < .001 for all) (Appendix Table A1). When comparing scores between the LLSB and SR groups at each postoperative time point, only the scores at 3 months differed significantly (VAS: P = .002; OSS: P < .001; ASES: P = .005) (Table 2).
Shoulder Functional Scores a

a Data are reported as mean ± SD. Boldface P values indicate statistically significant differences between groups (P < .05). ASES, American Shoulder and Elbow Surgeons; LLSB, locking-loop suture bridge; OSS, Oxford Shoulder Score; SR, single-row suture anchor; VAS, visual analog scale.
b Values were compared from preoperatively to 24 months postoperatively.
For the structural assessment, shoulder sonography was performed on every patient at 12 months after surgery using the Sugaya classification system. Table 3 summarizes the results of shoulder sonography at 12 months after rotator cuff repair. The overall rotator cuff retear rate was 10.26% and 6.82% in the LLSB and SR groups, respectively (P = .892). Those with a retear on sonography, 3 of 4 in the LLSB group and 2 of 3 in the SR group, underwent revision surgery. The other 2 participants were lost to follow-up. A superficial stitch abscess was found in 2 cases in the LLSB group and 3 cases in the SR group. There was no need for a reoperation, and the stitch abscess was managed with simple debridement during follow-up in the outpatient department.
Sugaya Classification 43 of Rotator Cuff Integrity at 12 Months a
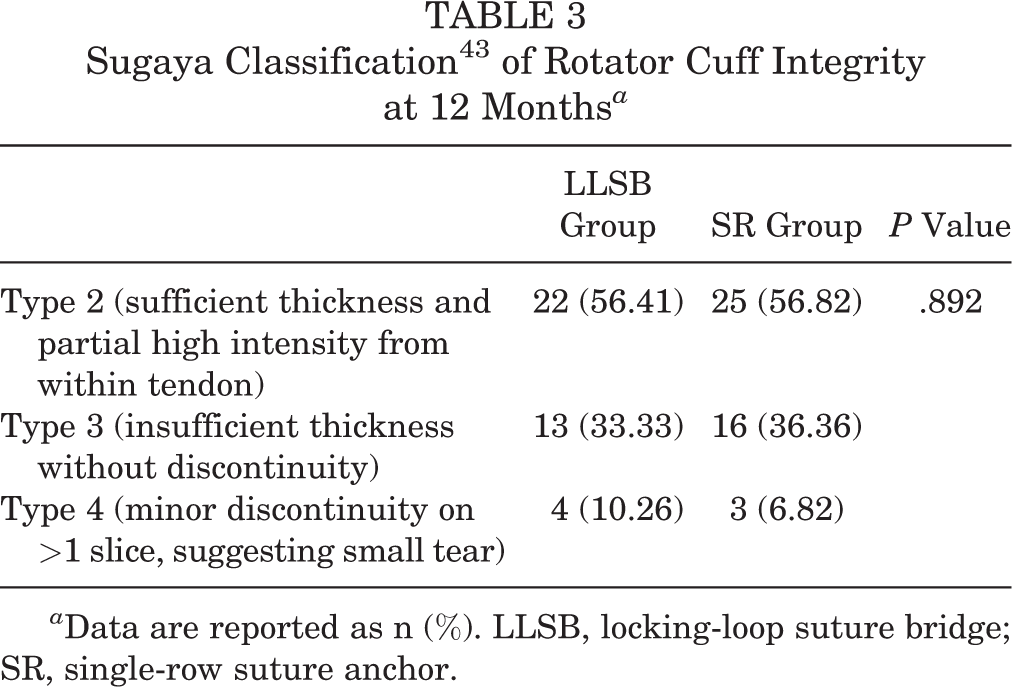
a Data are reported as n (%). LLSB, locking-loop suture bridge; SR, single-row suture anchor.
Discussion
In this study, superior outcomes were found in the LLSB group compared with the SR group in terms of VAS, OSS, and ASES scores at 3 months after surgery (VAS: P = .002; OSS: P < .001; ASES: P = .005). Thus, the proposed LLSB technique of arthroscopic-assisted mini-open repair was not inferior to SR repair in terms of postoperative functional outcomes and repair integrity in patients with small to medium rotator cuff tears.
Multiple factors affect rotator cuff healing, including gap formation, stiffness, restoration of footprint contact area and pressure, materials, and techniques. 47 A previous study 25 suggested that double-row sutures result in more favorable structural healing compared with SR sutures. Sandow and Schutz 40 demonstrated that arthroscopic rotator cuff repair using transosseous knotless anchors provides satisfactory healing and anchor stability, enabling the achievement of high functional recovery. Kim et al 22 reported that superior bone ingrowth could be achieved with open-construct PEEK anchors than with nonvented biocomposite anchors at early healing stages. On the basis of these findings, we believe that the proposed LLSB technique can provide favorable healing because of its similar mechanics to double-row repair and its use of knotless anchors.
However, several studies have reported similar functional outcomes regardless of the technique used to treat rotator cuff tears. 24,47,48 Liu et al 24 found no long-term difference in primary or secondary outcomes between all-arthroscopic and mini-open techniques; a significant difference was found only at 1 day and 1 month after surgery. Yamakado 47 reported no difference in clinical outcomes or rotator cuff integrity between suture bridge and medially based SR techniques at 1-year follow-up; postoperative rotator cuff failure was observed only in the suture bridge group, and incomplete healing was observed in the medially based SR group. Zafra et al 48 reported no difference in clinical results between SR transtendon and double-row suture bridge techniques for partial-thickness articular surface rotator cuff tears at 6 or 32.5 months (final follow-up) after surgery. These findings are consistent with our results; that is, at 2-year follow-up, no significant between-group difference in functional outcomes was observed, but at 3-month follow-up, the LLSB group exhibited more favorable outcomes than did the SR group.
Miller et al 26 reported no retears at 6 months after arthroscopic repair of massive rotator cuff tears. They also classified the causes of retears into 2 categories: “mechanical failure” in which retears occur in the early postoperative period (<3 months) and “biological failure” of healing at the tendon-bone interface in which recurrent tears happen later. In our study, the LLSB group exhibited superior outcomes at 3 months after surgery; it may be speculated that LLSB repair provided better initial mechanical stability than SR suture anchor repair, but after 3 months, both groups achieved biological healing, and the difference attributed to a mechanical effect gradually diminished.
Caldow et al 6 reported that the average footprint contact pressure and ultimate tensile strength after Mason-Allen repair did not differ significantly from those after double-row repair, but Mason-Allen repair had an inferior contact area compared with double-row repair. Their results also indicate that cruciate repair provided a better average footprint contact area and pressure without a difference in ultimate tensile strength than Mason-Allen repair. However, our technique can possibly achieve a similar contact area to double-row repair because it is based on a modified version of the traditional Mason-Allen technique, also mimicking cruciate repair. Moreover, Park et al 34,35 reported an improved mean contact area and pressure between the tendon and the footprint with the suture bridge technique. Shin et al 41 performed modified Mason-Allen repair and observed similar outcomes to those of double-row suture bridge repair. Kim et al 23 determined that arthroscopic suture bridge repair results in similar clinical outcomes and retear rates compared with double-row repair. Although not statistically significant, they noted a trend toward lower retear rates in the suture bridge group. These findings support our hypothesis that the proposed LLSB technique may provide good to excellent biomechanical benefits in rotator cuff healing, especially in the short term. Yet, long-term follow-up in our study revealed no significant difference between the LLSB and SR groups. In addition, the benefits, including pain relief, of a shorter recovery time may increase patient satisfaction and facilitate the implementation of rehabilitation protocols, both of which improve patients’ quality of life postoperatively.
Double-row suture bridge repair with arthroscopic surgery has become the predominant procedure for rotator cuff tears because it provides more contact area and pressure, a greater footprint percentage, a high load to failure, reduced gap formation at the repair site, and no increase in the retear rate. 23,41 However, double-row repair requires a longer operating time and a higher cost. 1,15,34 –36 In the present study, arthroscopic-assisted mini-open repair with modified suture bridging not only reduced the number of required suture anchors to half of that required in double-row repair but also reduced the stress of the greater tuberosity bone base. These effects are similar to those achieved through the double-row suture bridge technique.
We used an arthroscopic-assisted technique instead of an all-arthroscopic technique because of the limitations of LLSB repair. This is because if surgery were performed through an all-arthroscopic technique, the limited space would make it difficult for the needle to pass through and create a locking loop. Previous studies have revealed no difference in long-term functional outcomes or wound healing between all-arthroscopic and arthroscopic-assisted techniques. 5,21,24,28 Ozbaydar et al, 29 for example, reported the arthroscopic-assisted mini-open technique to be an effective method for rotator cuff repair. The cost incurred by the mini-open technique is also lower than that incurred by the all-arthroscopic technique, although both techniques produce equal outcomes. 18
Of the patients in our study, 73% underwent tenotomy of the long head of the biceps tendon with arthroscopic surgery because of a type 2 SLAP lesion and partial tearing with fraying or fibrillation of the tendon. This could cause factors outside of rotator cuff injuries to be overlooked, which may influence the prognosis of rotator cuff repair. The possible complications arising from these factors would not have been reduced if surgery were performed using the traditional mini-open technique instead of an arthroscopic-assisted mini-open technique.
The assessment of postoperative shoulder integrity through sonography has become the preferred method because of its convenience and ability to produce similar results to MRI. 4,9,30 Moreover, for an SR group with metallic implants, using MRI as an assessment tool may disturb the results. Although some scholars have claimed sonography to be less sensitive than MRI, 10 sonography is currently widely used for the evaluation of rotator cuff repair. 3,15,27,33 In our study, shoulder sonography was performed by a single rehabilitation physician, who has experience with sonography of the shoulder of >10 years. We also used sonography as an auxiliary diagnostic tool for rotator cuff tears; however, sonography is limited for assessments because of both its being operator dependent and its learning curve. 2,39
There are risk factors that influence the healing rate in patients undergoing rotator cuff repair, especially in the elderly. 16 However, a study conducted by Park et al 32 reported that patients aged >75 years with small to medium rotator cuff tears showed similar healing rates with those aged <60 years. Other studies supported that rotator cuff repair provides good stability and functional outcomes in elderly patients with full-thickness rotator cuff tears, with comparable results in younger patients. 14,38,44 Our study included patients aged 40 to 80 years with small to medium full-thickness rotator cuff tears. Despite the wide range in ages, similar results with the identical type of rotator cuff tears make the current study compatible with previous studies. However, there is evidence of higher retear rates in octogenarians in whom the only factor affecting the retear rate is the initial tear size. 32
The minimal clinically important difference (MCID) is an important metric to include in evaluations of outcomes and has become more popular recently. A systematic review conducted by Jones et al 20 concluded that the MCIDs for the ASES and OSS are 6.4-21.9 and 5-6.9, respectively. Based on this result, in comparing between the groups, our study achieved the MCID for both the ASES and OSS at 3-month follow-up (ASES: 7.89; OSS: 8.56). Moreover, in comparing within the groups, the LLSB and SR groups also achieved the MCID for both outcome measures at 3 months. The MCIDs for the ASES and OSS in the LLSB group were 50.53-68.15 and 21.65-37.31, which increased by 9.62 and 15.66, respectively. The MCIDs for the ASES and OSS in the SR group were 49.26-60.00 and 19.34-28.75, which increased by 11.03 and 9.41, respectively.
Limitations
Our study has the following limitations. (1) The sample size was relatively small; this might have caused statistical bias, and a larger number of cases should be collected in the future to compare these 2 patient groups. However, we ensured that all procedures were performed by a single surgeon. This was intended to produce identical diagnostic indications and criteria, consistent surgical techniques, and similar preoperative and postoperative assessment results, which reduced bias in the study. (2) We collected data from patients with small- to medium-sized tears; therefore, the outcomes at 6-month follow-up were somewhat inconsistent. (3) We assessed patients for only up to 2 years after surgery. A longer follow-up period is necessary to add strength to our findings. (4) We did not randomly separate the patients into different groups. On the contrary, patients chose the surgical technique after we described the methods. The difference between suture anchors (knot-tying suture anchor for SR group and knotless suture anchor for LLSB group) and fixation techniques produces different final patient costs in our health care system. This might possibly result in a selection bias. (5) The results might be influenced by some unpredictable factors, perhaps selection bias. Although both groups of patients were evaluated preoperatively, there was no difference in either patient demographics or tear characteristics. (6) Our novel technique provided mechanical stability similar to that of double-row suture anchor repair; however, our study compared the novel technique with SR repair. We did not create a control group of double-row repair because we no longer perform double-row repair. Future studies should be conducted to compare LLSB repair with other rotator cuff repair techniques.
Conclusion
Our data showed that the LLSB technique resulted in better VAS scores and functional outcomes at 3-month follow-up, with no difference in retear rates at 12 months by sonography, compared with the SR technique. In conclusion, the proposed LLSB technique is a reliable technique to consider for rotator cuff repair of small to medium-sized tears. Also, future randomized designed studies and biomechanical and histological studies may be important to improve our knowledge of rotator cuff repair techniques.
Footnotes
Acknowledgment
The authors thank Chen-Yu Douglas Wang for illustrations of the LLSB technique. They also thank Yu-Chi Katie Yu for helping with the English-language proofreading of the study.
Final revision submitted September 5, 2022; accepted September 13, 2022.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Taipei Medical University (TMU-JIRB No. N202004066).
APPENDIX
P Values for Differences in Functional Outcome Scores From Preoperatively to Postoperatively a
| Group | Variable | Reference | P Value (t Test) | Power |
|---|---|---|---|---|
| LLSB | 3-mo VAS | Preoperative VAS | <.001 | 1 |
| LLSB | 6-mo VAS | Preoperative VAS | <.001 | 1 |
| LLSB | 12-mo VAS | Preoperative VAS | <.001 | 1 |
| LLSB | 24-mo VAS | Preoperative VAS | <.001 | 1 |
| LLSB | 3-mo OSS | Preoperative OSS | <.001 | 1 |
| LLSB | 6-mo OSS | Preoperative OSS | <.001 | 1 |
| LLSB | 12-mo OSS | Preoperative OSS | <.001 | 1 |
| LLSB | 24-mo OSS | Preoperative OSS | <.001 | 1 |
| LLSB | 3-mo ASES | Preoperative ASES | <.001 | 1 |
| LLSB | 6-mo ASES | Preoperative ASES | <.001 | 1 |
| LLSB | 12-mo ASES | Preoperative ASES | <.001 | 1 |
| LLSB | 24-mo ASES | Preoperative ASES | <.001 | 1 |
| SR | 3-mo VAS | Preoperative VAS | <.001 | 1 |
| SR | 6-mo VAS | Preoperative VAS | <.001 | 1 |
| SR | 12-mo VAS | Preoperative VAS | <.001 | 1 |
| SR | 24-mo VAS | Preoperative VAS | <.001 | 1 |
| SR | 3-mo OSS | Preoperative OSS | <.001 | 1 |
| SR | 6-mo OSS | Preoperative OSS | <.001 | 1 |
| SR | 12-mo OSS | Preoperative OSS | <.001 | 1 |
| SR | 24-mo OSS | Preoperative OSS | <.001 | 1 |
| SR | 3-mo ASES | Preoperative ASES | <.001 | 1 |
| SR | 6-mo ASES | Preoperative ASES | <.001 | 1 |
| SR | 12-mo ASES | Preoperative ASES | <.001 | 1 |
| SR | 24-mo ASES | Preoperative ASES | <.001 | 1 |
a ASES, American Shoulder and Elbow Surgeons; LLSB, locking-loop suture bridge; OSS, Oxford Shoulder Score; SR, single-row suture anchor; VAS, visual analog scale.