
Abstract
Background:
For skeletally immature patients, over-the-top (OTT) anterior cruciate ligament (ACL) reconstruction (ACLR) is preferred. However, increased anterior laxity at deep knee flexion angles remains concerning. We modified the procedure to proximally shift the graft fixation site on the femur to prevent graft loosening at higher knee flexion angles and named it the supra-OTT procedure.
Purpose:
To compare anterior laxity and in situ forces of the ACL graft between conventional OTT and supra-OTT ACLR in a cadaveric model.
Study Design:
Controlled laboratory study.
Methods:
A total of 11 fresh-frozen cadaveric knee specimens underwent 4 robotic testing conditions: ACL intact, ACL resected, conventional OTT, and supra-OTT. For each condition, a 100-N load was applied at 0°, 15°, 30°, 60°, and 90° of knee flexion to simulate the Lachman test or anterior drawer test. In addition, a combined load of 5-N·m internal tibial torque and 10-N·m valgus torque was applied at 15° and 30° of knee flexion as a simulated pivot-shift test. Anterior tibial translation and in situ graft forces were recorded. The only difference between conventional OTT and supra-OTT ACLR was the graft fixation site on the femur. For conventional OTT ACLR, graft fixation was performed just on the proximal and lateral ends of the posterior condyle. For supra-OTT ACLR, the fixation point was around the proximal insertion of the lateral head of the gastrocnemius and the lateral edge of the posterior cortex, approximately 2 cm proximal to the conventional OTT position.
Results:
On the simulated anterior drawer test at 60° and 90° of knee flexion, anterior tibial translation after supra-OTT ACLR was significantly smaller than after conventional OTT ACLR (P < .01). However, no significant differences were noted at other flexion angles or on the simulated pivot-shift test between the conventional OTT and supra-OTT procedures. Some overconstraint and higher graft forces were noted with both techniques, but the supra-OTT technique caused even more overconstraint at higher flexion angles.
Conclusion:
Supra-OTT ACLR showed better biomechanical performance to control anterior laxity than conventional OTT ACLR at higher knee flexion angles.
Clinical Relevance:
The supra-OTT procedure may improve anterior stability at deep knee flexion angles.
Keywords
An anterior cruciate ligament (ACL) injury is a common sports injury, and it is usually treated surgically. 22 Although anatomic ACL reconstruction (ACLR) via femoral and tibial tunnels mostly produces good clinical outcomes, 22 this tunnel technique could be disadvantageous for skeletally immature patients with open physes or for those undergoing revision ACLR with large widened tunnels.
The number of ACLR procedures in skeletally immature patients has recently increased to avoid secondary meniscal or chondral injuries after nonoperative treatment. 24 The main concern in ACLR for skeletally immature patients is physeal damage due to drilling to create the tunnel, resulting in angular deformities or leg-length discrepancies. 4,8,25 These complications occur more often in the femur than in the tibia 4 because the femoral physis closes later than the tibial physis. 6 Additionally, the orientation of the femoral tunnel is usually less perpendicular to the physis than the tibial tunnel.
In patients undergoing revision ACLR, enlarged tunnels around the ACL attachment sites may result in difficulty placing the grafts at proper positions inside the sites. Thus, those with large widened tunnels often have instability after 1-stage revision ACLR with improperly placed grafts or they endure a longer treatment period with 2-stage revision surgery. 28 This problem occurs more often in the femoral tunnel because tunnel widening is more prominent in the femur than in the tibia. 15
In skeletally immature patients, over-the-top (OTT) ACLR attracts much attention because it does not require the creation of a femoral tunnel. 13,14 Instead of the creation of a femoral tunnel, a folded hamstring tendon graft is secured by fixation devices (bicortical screw, washer, staple, etc) at the lateral femoral metaphysis just proximal to the posterior femoral condyle (ie, the OTT position). 1,11,17,20,23 Although satisfactory clinical outcomes as well as good anterior stability at shallow knee flexion angles have been reported on biomechanical testing using cadaveric specimens, increased anterior laxity has been reported at deep knee flexion angles on both biomechanical testing and clinical physical examinations. Moreover, a case of OTT graft slippage from the lateral posterior condyle into the lateral compartment has been reported. 2 Although graft slippage is an extreme case, the ACL graft in conventional OTT ACLR may tend to slip from the lateral posterior condyle to some extent, resulting in slackening of the graft. 17
We modified the conventional OTT technique to shift the femoral fixation site proximally so as to prevent graft loosening at deep knee flexion angles and named it the “supra-OTT” procedure. The purpose of this cadaveric study was to compare anterior laxity and in situ forces of the ACL graft between conventional OTT and supra-OTT ACLR when a simulated anterior drawer test or a simulated pivot-shift test was performed. We hypothesized that the supra-OTT procedure would result in decreased anterior laxity compared with conventional OTT ACLR at higher flexion angles.
Methods
Specimen Preparation
The study protocol was approved by the ethics committee of our institution. A total of 11 fresh-frozen knee specimens from 6 male and 5 female cadaveric donors were used (mean age at death, 84.2 years [range, 70-93 years]). The specimens were donated by donors who had provided informed consent before death. Physical examinations were performed before biomechanical testing to confirm ligamentous stability and range of motion from full extension to 130° of flexion. Specimens with ligamentous instability or loss of range of motion were excluded.
Specimens were thawed at room temperature for at least 24 hours before testing. Then, each specimen was kept wet to avoid tissue deterioration during testing. The femur and tibia were cut to ≥15 cm above and below the joint line, whereas the fibula was cut 5 cm below the proximal tibiofibular joint. The soft tissues, including all the muscles except the popliteus, as well as the patella were removed, whereas the ligaments, posterior capsule, and meniscus were left intact. Both ends of the tibia and femur were fixed using acrylic resin (Ostron II; GC) poured into a cylindrical mold. The fibula was fixed in its original position using resin. The femoral and tibial cylinders were fixed with aluminum clamps and connected to the end-effector of the robotic testing system 5 (FRS2010; Technology Service) (Figure 1).

Robotic testing system with a right knee. The manipulator, which worked with the universal force-torque sensor, was placed on the end-effector. The tibia was fixed on the end-effector, and the femur was fixed to the lower part of the device using metal clamps. An adjustable tension rod was attached to the plate, which was connected to the tibial clamp, and the force gauge was attached to the tendon graft.
Surgical Procedure
Both conventional OTT and supra-OTT ACLR were performed on the same knee, and the testing order of conventional OTT and supra-OTT ACLR was randomized. Conventional OTT 14,17,29 and supra-OTT ACLR were performed via only 1 tibial tunnel. The only difference between conventional OTT and supra-OTT ACLR was the graft fixation site around the OTT position (Figure 2). The same 4-strand hamstring tendon graft, made from doubled semitendinosus and gracilis tendons, was used in both procedures.
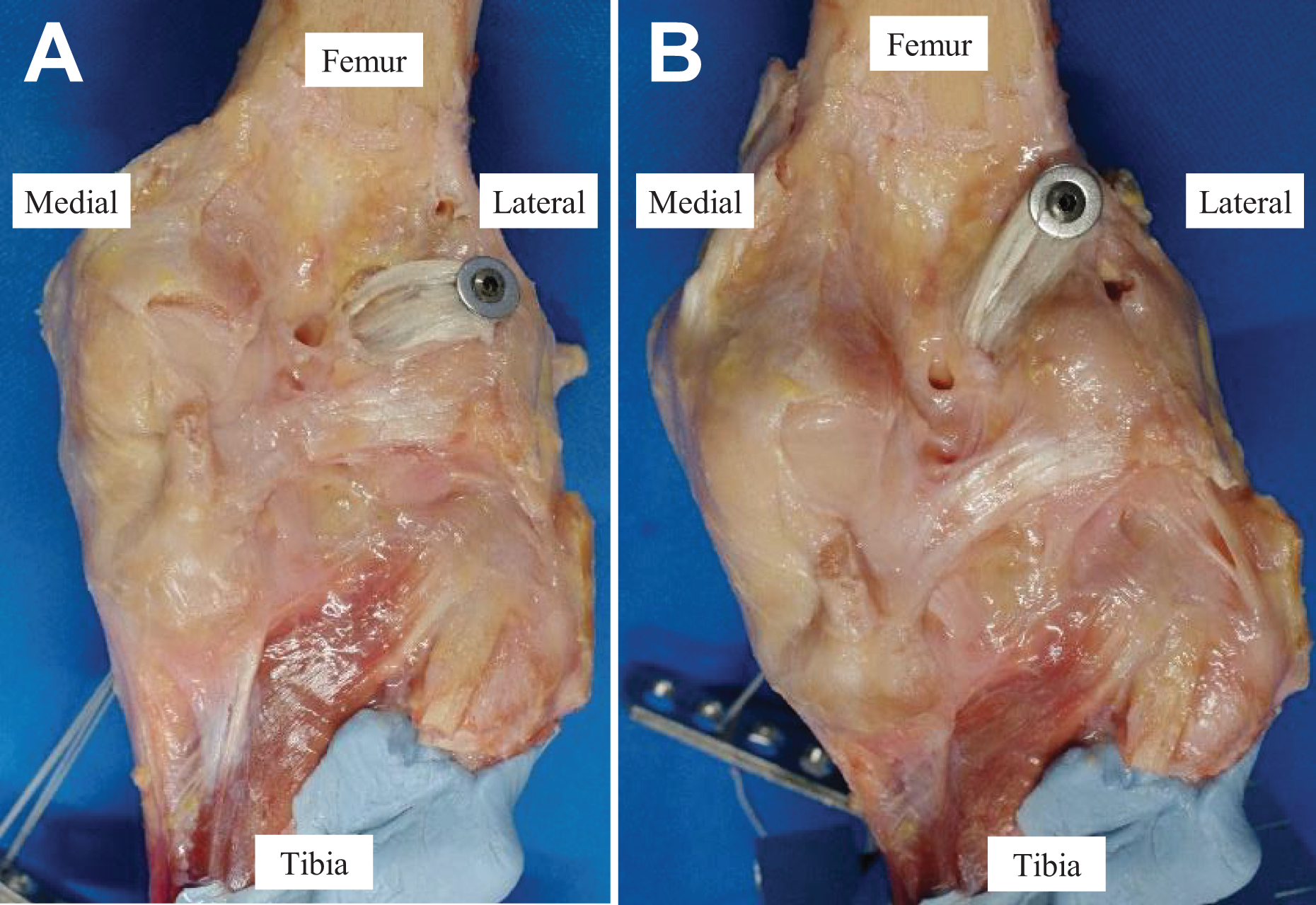
Anterior cruciate ligament reconstruction of the right knee (posterior view): (A) conventional over-the-top (OTT) and (B) supra-OTT.
The free ends of the graft were sutured using No. 3 polyester sutures (ELP, Akiyama Seisakusyo, Tokyo, Japan) with the Krackow suture technique. After the removal of the native ACL, the tibial footprint was clearly visualized, and a guide wire was inserted into the center of the ACL attachment area using an outside-in tibial guide and was overdrilled to the size of the tendon graft (7 or 8 mm). For conventional OTT ACLR, graft fixation was performed at the proximal and lateral ends of the posterior condyle (Figure 2A). For supra-OTT ACLR, the fixation point was around the proximal insertion of the lateral head of the gastrocnemius and the lateral edge of the posterior cortex, approximately 2 cm proximal to the OTT position (Figure 2B). In a pilot study, the supra-OTT position was scrutinized to ensure that the reconstructed graft better mimicked the native ACL in a running route around the femoral attachment area from knee extension to flexion. After the identification of the fixation points for the conventional OTT and supra-OTT procedures, a guide wire was drilled into each point (Smith & Nephew). The posterior joint capsule was penetrated around the OTT position by passing a curved clamp in an inside-out manner, and the looped end of the graft was passed through. The looped portion of the hamstring tendon graft was secured using a cannulated screw with a titanium washer (Smith & Nephew) at the first selected OTT position. The sutures of the free ends of the graft were connected to the force gauge installed at the tibial tunnel entrance (Figure 1).
Before the main tests, as preconditioning of the graft, the specimen was set at 30° of knee flexion in the robotic testing system, and 50 N of tensile loading was applied to the graft for 300 seconds to minimize the viscoelastic effects of creep. Then, initial tension was adjusted to 44 N at 30° of knee flexion, as shown with single-bundle OTT ACLR with a 4-strand hamstring tendon graft in a previous study, 17 and the tests were performed. After the tests of the first selected OTT procedure, the graft was removed and then fixed to the other OTT position, and the same preparation steps and tests were performed.
Testing Apparatus
We utilized a robotic testing system with a custom-made manipulator with 6 degrees of freedom, equipped with a universal force-torque sensor (DELTA IP65, SI-660-60; ATI Industrial Automation) (Figure 1). The robotic testing system can simulate physiological knee joint motion with respect to the joint coordinate system developed by Grood and Suntay 12 in vitro. This system, which guides the displacement of, and force/torque applied to, the knee joints, was controlled in real time by a LabView-based program (Version 12.0.1; National Instruments) running on Windows (Microsoft).
Testing Protocol
First, the flexion-extension axis of the knee was defined as 0° of flexion when 0.5 N·m of extension moment was applied to the intact knee. Next, passive flexion-extension was performed from its hyperextended position, with 5 N·m of extension moment, to 120° of knee flexion; this was applied at a rate of 0.5 deg/s and repeated 3 times as preconditioning. Finally, 2 types of external loading tests were performed: (1) a 100-N load was applied to the knee at 0°, 15°, 30°, 60°, and 90° of knee flexion to simulate the Lachman test or anterior drawer test; and (2) a combined load of 5-N·m internal tibial torque and 10-N·m valgus torque was applied to the knee at 15° and 30° of knee flexion as a simulated pivot-shift test. 27 After testing of the intact knee, the ACL was resected. Then, both loading tests were performed, and the recorded intact knee motion was reproduced for the ACL-resected knee, while the force/torque of the knee was recorded. By applying the principle of superposition, 9,10 the in situ force of the ACL was determined using the 6 degrees of freedom force/torque data of the ACL-intact and ACL-resected states. Then, the 2 OTT techniques were performed in the same knee in randomized order. A simulated anterior drawer test and a simulated pivot-shift test were performed for each testing condition, and the 3-dimensional motion and in situ graft force obtained by the force gauge were recorded.
Visualization of the Route of the OTT Grafts
In a pilot study, photographs were obtained to visualize the route of the graft of the 2 OTT techniques. First, the route of the graft for conventional OTT ACLR was examined. After the anterior drawer test, the medial femoral condyle was removed to visualize the graft. The motion of the knee was repeated using the joint motion reproduction function of the robotic testing system, and the medial view of the graft route was recorded using a full high-vision video camera (HDR-CX500; Sony). Next, the route of the graft for supra-OTT ACLR was similarly examined.
Statistical Analysis
Anterior tibial translation (ATT) under both loads for the ACL-intact state, ACL-resected state, conventional OTT ACLR state, and supra-OTT ACLR state was analyzed using 2-factor repeated-measures analysis of variance with post hoc pairwise comparisons using the Bonferroni correction. The in situ forces of the graft between conventional OTT and supra-OTT ACLR were analyzed using 2-factor repeated-measures analysis of variance with post hoc pairwise comparisons using the Bonferroni correction. All analyses were performed using Statistical Package for Social Sciences (Version 28.0; IBM). A P value <.05 was considered statistically significant.
Post hoc power analysis was performed to determine the power of the study. On the basis of the mean and standard deviation values of ATT and in situ forces during the anterior drawer test, the power of this study ranged from 0.856 to 1.000.
Results
ATT in Each Condition
In the ACL-intact state, ATT increased with higher flexion angles. After ACL sectioning, ATT was markedly greater compared with the ACL-intact state at all flexion angles. On the anterior drawer test at 60° and 90° of knee flexion, ATT of knees that underwent supra-OTT ACLR was significantly smaller compared with that of knees that underwent conventional OTT ACLR (P < .01) (Figure 3). Under a 100-N load at 0°, 15°, 30°, and 60° of knee flexion and under a combined load at 15° of knee flexion, ATT of both conventional OTT and supra-OTT ACLR knees was smaller than that of the ACL-intact condition (P < .01 for all). Additionally, on the anterior drawer test at 90° of knee flexion, ATT of knees that underwent supra-OTT ACLR was smaller versus the ACL-intact condition, whereas there was no difference in knees that underwent conventional OTT ACLR versus intact knees.
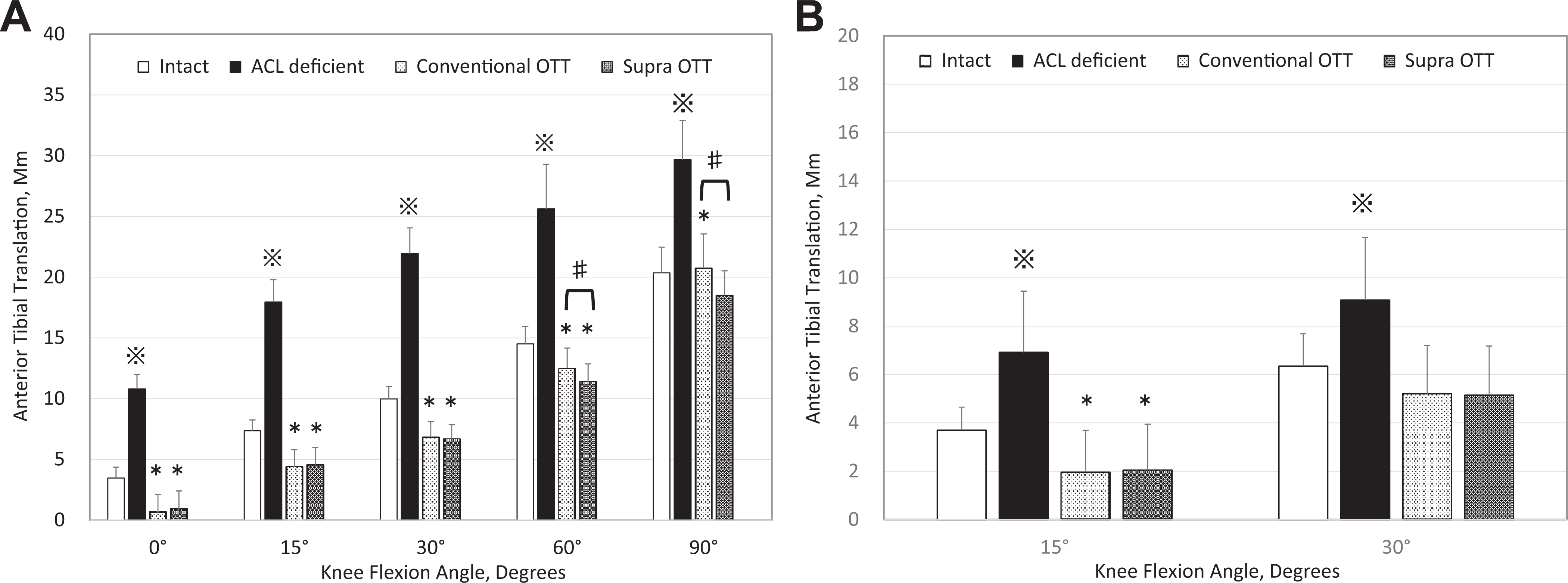
Anterior tibial translation at each knee flexion angle in each testing state (A) under a 100-N load (simulated anterior drawer test) and (B) under a combined load of 5-N·m internal tibial torque and 10-N·m valgus torque (simulated pivot-shift test). Statistically significant difference *compared with the anterior cruciate ligament (ACL)–intact state, ※compared with all other states, and #between the conventional over-the-top (OTT) and supra-OTT states.
In Situ Force in Each Condition
The in situ force of the native ACL was similar between 0° and 30° of flexion but decreased with higher flexion angles. No significant difference was found regarding in situ forces between the grafts of knees that underwent conventional OTT and supra-OTT ACLR (Figure 4). The in situ force of the knees that underwent conventional OTT and supra-OTT ACLR was significantly higher than that of the ACL-resected knees under a 100-N load at 0° (P < .01) and 15° (P < .01 and P = .01) of knee flexion and under a combined load at 15° and 30° of knee flexion (P < .01).

In situ force at each knee flexion angle in each testing state (A) under a 100-N load (simulated anterior drawer test) and (B) under a combined load of 5-N·m internal tibial torque and 10-N·m valgus torque (simulated pivot-shift test). *Significantly different compared with the native anterior cruciate ligament (ACL). OTT, over-the-top.
Visualization of the Route of the OTT Grafts
Figure 5 shows the medial view of the route of the graft at 90° of knee flexion during the reproduction of motion when the anterior drawer test was performed. The graft after conventional OTT ACLR at 90° of knee flexion (Figure 5A) was observed to slip down from the medial wall of the lateral femoral condyle. On the contrary, the graft after supra-OTT ACLR appeared to be running on the medial wall of the lateral femoral condyle around the ACL femoral attachment area at 90° of knee flexion (Figure 5B). Similarly, Figure 6 shows the medial view of the route of the graft at 0° of knee flexion. The route of the graft at 0° of flexion was similar with both techniques.
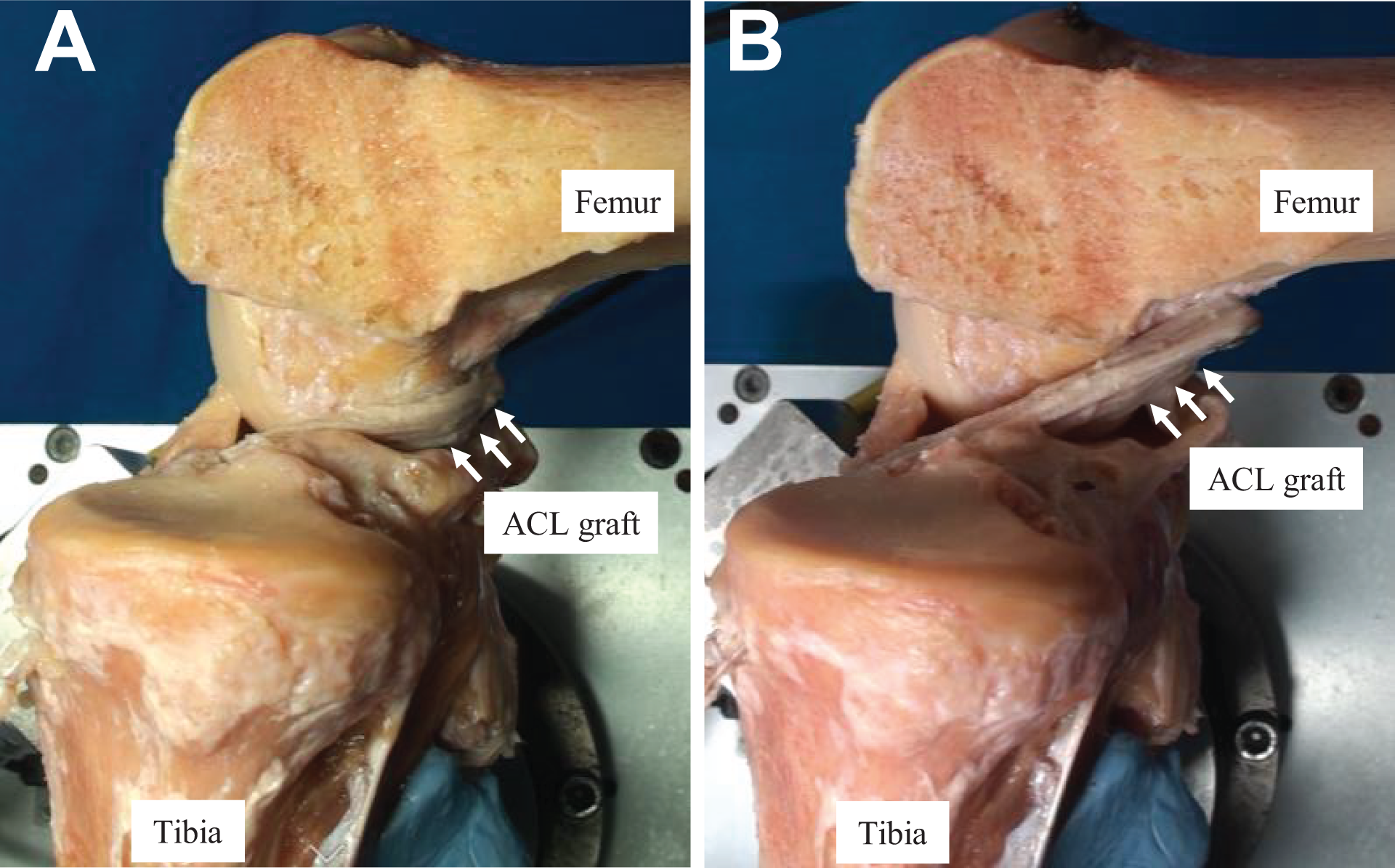
Route of the graft on the anterior drawer test at 90° of knee flexion (medial view) for (A) conventional over-the-top (OTT) and (B) supra-OTT anterior cruciate ligament (ACL) reconstruction. The medial femoral condyle was removed to allow visualization of the graft. The white arrows indicate the ACL graft. The graft in A was dislocated from the posterior femoral condyle.

Route of the graft on the anterior drawer test at 0° of knee flexion (medial view) for (A) conventional over-the-top (OTT) and (B) supra-OTT anterior cruciate ligament (ACL) reconstruction. The medial femoral condyle was removed to allow visualization of the graft. The white arrows indicate the ACL graft.
Discussion
In this cadaveric study, we compared the conventional OTT and supra-OTT techniques with respect to anterior laxity and in situ graft forces in response to a simulated anterior drawer test and a simulated pivot-shift test. The results showed that ATT of supra-OTT ACLR at 60° and 90° of knee flexion was significantly smaller than that of conventional OTT ACLR, although the differences between them were small. The knees that underwent conventional OTT ACLR were not overconstrained at 90° of knee flexion, while they were overconstrained at 0° to 60°.
Previous studies have reported that knees that underwent conventional OTT ACLR were overconstrained at shallow knee flexion angles but were not overconstrained at deep knee flexion angles. In other words, these knees showed more laxity than the intact knee at deep knee flexion angles, as observed in the present study. 16,17,20 On the contrary, the results of the present study indicated that ATT of supra-OTT ACLR was significantly smaller than that of conventional OTT ACLR at higher flexion angles. The graft of conventional OTT ACLR slipped off from the posterior femoral condyle, and this resulted in slackening of the graft (Figure 5). In contrast, the graft of supra-OTT ACLR did not slip off and aligned straightly on the anterior drawer test (Figure 5). This may be the cause of the larger ATT at deep knee flexion angles in conventional OTT ACLR compared with the smaller ATT in supra-OTT ACLR. Previous clinical studies 2,21 have also shown graft slippage after conventional OTT ACLR, as observed in this study.
The in situ forces of the grafts with both conventional OTT and supra-OTT ACLR were higher than that of the native ACL in response to a simulated anterior drawer test at 0° and 15° of knee flexion and a simulated pivot-shift test at 15° and 30° of knee flexion. Furthermore, ATT of knees that underwent conventional OTT and supra-OTT ACLR was smaller than that of the intact knee in response to a simulated anterior drawer test at 0° to 60° of knee flexion and a simulated pivot-shift test at 15° of knee flexion. These results suggest that the initial tension of 44 N at 30° of knee flexion may be too much for OTT ACLR. Another possible reason for the overconstraint may be that the fixation point of the graft is not anatomic. As the initial tension applied to a graft is one of the key factors for successful ACLR, 3,7,18,19 excessive initial tension may cause abnormal tibiofemoral compressive forces, result in graft failure, or lead to degeneration of the articular cartilage. 7,29 Especially in supra-OTT ACLR, the knee was constantly overconstrained throughout the entire range of flexion. Thus, the initial tension to the graft may need to be reconsidered in supra-OTT ACLR.
Limitations
This study has several limitations. First, we only performed OTT ACLR procedures under an initial tension of 44 N at 30° of knee flexion according to a previous study. 17 This amount of initial tension appears to be excessive for supra-OTT ACLR, as the knee was overconstrained at all knee flexion angles. The initial tension for supra-OTT ACLR could be reduced to less than 44 N at 30° of knee flexion to avoid too much overconstraint. Second, anatomic ACLR via tunnels was not performed for a comparison; however, previous comparative studies have shown minor differences between anatomic and OTT ACLR. 1,16,17,20 Third, while no tunnel breakage or graft damage was macroscopically observed during or after the experiments, the experiments were performed using specimens from elderly donors with poor bone quality as well as degenerative tendons, which could have caused potential biases. Fourth, this experimental model used the same knee joints and tendons multiple times. However, the use of the same hamstring tendon grafts in the same knees with 2 different techniques of OTT ACLR made it possible to compare the 2 procedures with minimized interspecimen variation and increased statistical power. Fifth, as the present results were obtained through in vitro tests, muscle forces, graft remodeling, load relaxation, and the contribution of soft tissues such as the anterior capsule and extensor mechanism, which had been excised during specimen preparation, were not taken into account. Moreover, the simulated pivot shift, comprising coupled moments at a static flexion angle, may not have sufficiently replicated the in vivo kinematics of the pivot-shift test, even though such biomechanical tests have been used in numerous studies. 10,26,29
Conclusion
Supra-OTT ACLR showed better biomechanical performance to control anterior stability than conventional OTT ACLR, as the former prevented graft slippage at deeper knee flexion angles. However, although some overconstraint and higher graft forces were noted with both techniques, the supra-OTT technique caused even more overconstraint at higher flexion angles.
Footnotes
Final revision submitted August 29, 2022; accepted September 13, 2022.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Sapporo Medical University (No. 1-2-68).