
Abstract
Background:
The tibiofemoral rotation angle has been found to be higher in patients with recurrent patellar dislocations (RPDs) than in healthy people; however, little is known about the clinical significance of this finding.
Purpose:
To determine whether an increased tibiofemoral rotation angle is associated with graft failure after primary medial patellofemoral ligament reconstruction (MPFL-R) and to investigate the role of the tibiofemoral rotation angle in predicting MPFL-R failure in patients with RPDs.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
We retrospectively analyzed the records of 632 consecutive patients with clinically diagnosed RPDs from 2011 to 2018. Postoperative stress radiography of the patellofemoral joint was performed to identify whether the graft failed. After a review, 33 patients who showed MPFL-R failure were allocated to the failure group. They were matched 1:2 to 66 participants who underwent successful MPFL-R (control group). The cutoff value and area under the curve (AUC) of the tibiofemoral rotation angle for predicting graft failure after primary MPFL-R were determined, and the risk factors for MPFL-R failure were assessed by multivariate logistic regression analysis.
Results:
The tibiofemoral rotation angle was significantly higher in the failure group than in the control group (16.4° ± 5.6° vs 6.4° ± 4.5°, respectively; P < .001). The cutoff value of the tibiofemoral rotation angle for predicting graft failure was 12.3° (sensitivity, 81.8%; specificity, 89.4%; AUC, 0.920). Overall, 3 risk factors for MPFL-R failure were determined: excessive tibiofemoral rotation (≥12.3°) (odds ratio [OR], 13.159 [95% CI, 2.469-70.139]; P = .003), a preoperative high-grade J-sign (OR, 7.674 [95% CI, 1.232-47.809]; P = .029), and a femoral tunnel malposition (OR, 6.976 [95% CI, 1.077-45.187]; P = .042).
Conclusion:
In this study, excessive tibiofemoral rotation, a preoperative high-grade J-sign, and a femoral tunnel malposition were identified as risk factors for graft failure after primary MPFL-R in patients with RPDs. More importantly, excessive tibiofemoral rotation ( ≥ 12.3°) may predict the failure of primary MPFL-R, which can help surgeons easily identify high-risk patients of MPFL-R failure before surgery.
Keywords
Medial patellofemoral ligament (MPFL) reconstruction (MPFL-R) is a reliable procedure for the treatment of recurrent patellar dislocations (RPDs); therefore, it is gaining popularity among surgeons. 6,18 However, inferior clinical outcomes have also been reported in the literature, which is usually because of interactions among multiple factors. 22,35 Currently, technical errors and missed risk factors have been recognized as 2 potential causes of poor outcomes after MPFL-R. 17,35 Among the many missed risk factors, rotational deformities of the lower extremities have become top research topics in recent years, and increased femoral anteversion is the focal point. 7,11,31 A recent biomechanical study revealed that increased femoral anteversion could significantly enhance the lateralizing force that acts on the patella. 11 Some clinical studies also found that increased femoral anteversion was associated with MPFL-R failure. 17,34 Given these reasons, femoral derotational osteotomy has been proposed to treat RPDs with increased femoral anteversion, and subsequent clinical studies have confirmed the clinical benefit of this osteotomy procedure. 8,9,16,30
Tibiofemoral rotation is 1 of the 3 components of rotational deformities of the lower extremities; however, it has received far less attention than femoral anteversion or tibial torsion in the literature. The tibiofemoral rotation angle is measured by comparing the angle between the posterior femoral and tibial condylar lines, representing relative external rotation of the proximal tibia to the distal femur. 25 Recently, increased tibiofemoral rotation has been identified as a potential contributing factor to RPDs. 2,5,14,19 Moreover, several recent studies have found that the tibiofemoral rotation angle was correlated with the severity of patellar dislocations and patellar maltracking. 12,14 In theory, abnormal external rotation of the tibia relative to the distal femur can result in excessive lateralization of the tibial tubercle, increase the lateral tilt, and attenuate the MPFL or graft, all of which contribute to decreased patellar stability. 14 Based on these potential mechanisms, it is reasonable to hypothesize that an increased tibiofemoral rotation angle may be one of the contributing factors to inferior clinical outcomes after MPFL-R.
The purpose of this study was (1) to determine whether an increased tibiofemoral rotation angle is associated with graft failure after primary MPFL-R and (2) to investigate the role of the tibiofemoral rotation angle in predicting MPFL-R failure in patients with RPDs. It was hypothesized that abnormal tibiofemoral rotation was associated with MPFL-R failure and that excessive preoperative tibiofemoral rotation was a reliable predictor of graft failure after MPFL-R.
Methods
Study Design
This was a case-control study with prospectively collected data and retrospective data analysis. The protocol for this study was approved by our ethics committee, and all participants provided informed consent. From 2011 to 2018, a total of 632 knees with RPDs were treated with MPFL-R in isolation or combined with tibial tubercle transfer. At our institution, stress radiography of the patellofemoral joint is routinely performed at 1 to 2 years after surgery in patients with RPDs to assess the stability of the patella, no matter which procedures have been performed. Patients were excluded from the study if they met at least 1 of the following criteria on the injured side: (1) lack of postoperative stress radiographs of the patellofemoral joint, (2) skeletal immaturity, (3) combined derotational osteotomy or trochleoplasty, (4) lack of preoperative or postoperative radiological data, and (5) no record of the preoperative J-sign grade. The application of exclusion criteria left 453 knees.
The included patients were then allocated to 2 groups according to the MPFL graft status on postoperative stress radiography: If the patellar central ridge surpassed the apex of the lateral femoral trochlea, the graft was defined as having failed (failure group, n=33). Each patient in the failure group was matched 1:2 to participants who had stable patellofemoral joints as shown on stress radiography (n=420). Patients were matched by age, sex, and surgical technique. There were 33 knees with failed MPFL grafts, which were matched with 66 control knees (Figure 1).
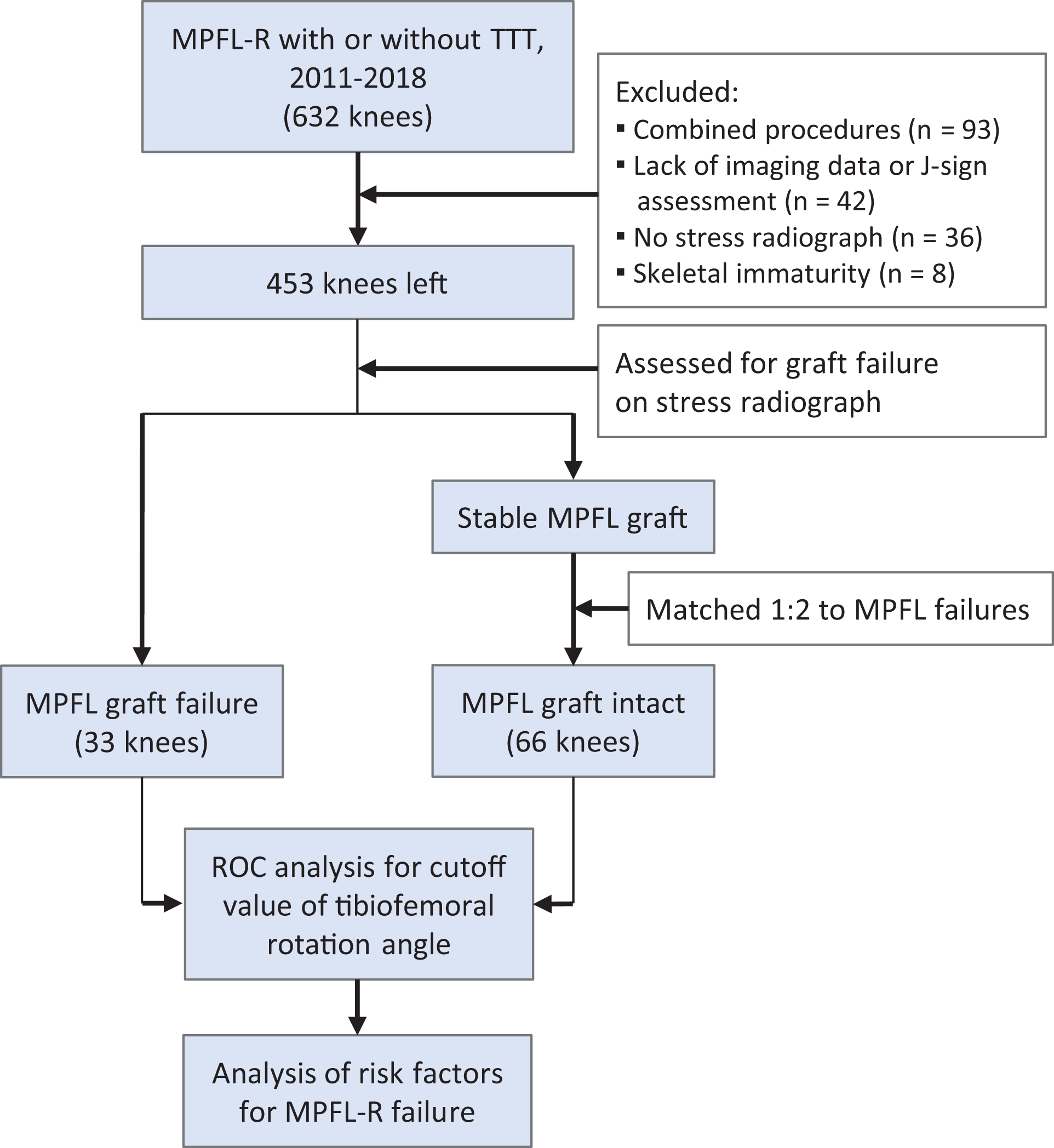
Flowchart of patient selection. MPFL, medial patellofemoral ligament; MPFL-R, MPFL reconstruction; ROC, receiver operating characteristic; TTT, tibial tubercle transfer.
Assessment of MPFL Graft Status
A previous study found that the results of postoperative stress radiography of the patellofemoral joint were correlated with patient-reported outcomes after MPFL-R, 32 and this assessment was routinely performed postoperatively in patients with RPDs. Axial patellofemoral fluoroscopy was performed with the knee flexed at 30° by the same surgeon (H.Z.) to identify patients with objective MPFL graft failure, according to the method described by Zhang et al 30 in which if the patellar central ridge surpassed the apex of the lateral femoral trochlea, the graft was defined as having failed (Figure 2).
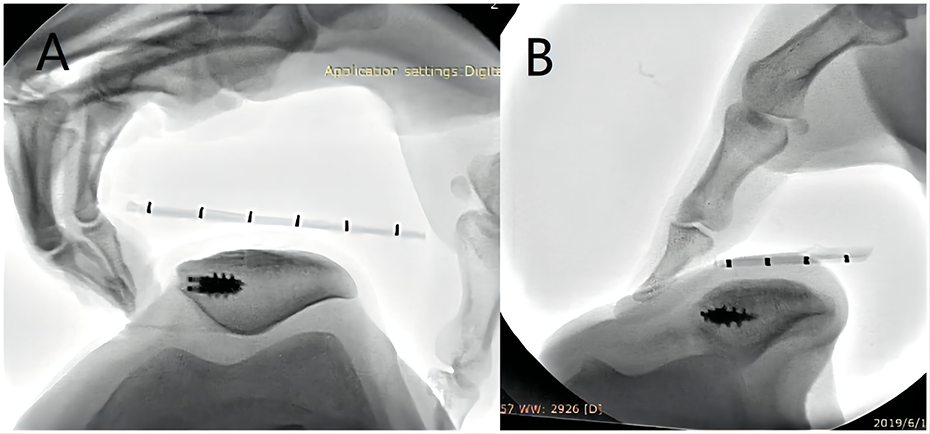
Assessment of medial patellofemoral ligament graft status. (A) Patient with a stable graft. (B) Patient with a failed graft.
Assessment of Lower Leg Rotational Parameters
Computed tomography (CT) was performed on an Toshiba Aquilion scanner (Toshiba) for all patients with RPDs preoperatively according to a standardized protocol, keeping the foot in 0° of external rotation and the knee in full extension. Digital Imaging and Communications in Medicine data from the hip-knee-ankle CT scan were reconstructed into 3-dimensional models with Mimics Version 20.0 (Materialise) to measure the rotational parameters of the lower extremities according to a method described previously 25 (Figure 3). The femoral anteversion angle was defined as the angle formed between the axis of the femoral head-neck and the distal femur. The tibiofemoral rotation angle was measured by comparing the angle between the posterior femoral and tibial condylar lines. A positive angle indicates internal rotation of the distal femur relative to the proximal tibia. The tibial torsion angle was assessed by measuring the rotational angle of the proximal tibia relative to the distal tibia.

Assessment of lower leg rotational parameters. (A) Femoral anteversion angle. (B) Tibiofemoral rotation angle. (C) Tibial torsion angle.
Radiological Measurements and Patellar Tracking Assessment
The knee radiographs included the anteroposterior view and the lateral view at 30° of knee flexion. The Caton-Deschamps Index was used to measure patellar height. Trochlear dysplasia was detected in the true lateral view of the knee and classified according to the Dejour classification system. 4 Type B and type D were defined as severe trochlear dysplasia. 32 The tibial tubercle–trochlear groove (TT-TG) distance was measured on a CT according to the method described by Camp et al. 3
A J-sign evaluation was performed to evaluate the severity of patellar maltracking, and grading was performed according to the modified classification system of Zhang et al. 33
Assessment of Femoral Tunnel Position
A true medial view of the femur was achieved by superimposing the posterior aspects of the femoral condyles using 3-dimensional CT according to the method described by Kita et al. 13 The distance between the center of the femoral tunnel and the Schöttle point was measured in millimeters. According to Servien et al, 21 a femoral tunnel was considered malpositioned when the center of the tunnel was at a distance of >10 mm from the Schöttle point (Figure 4).

Assessment of femoral tunnel position. The true lateral view of the femur was obtained when the posterior margins of the femoral condyles were superimposed on a 3-dimensional computed tomography image. Then, the Schöttle point (S) was identified (intersection of the 2 red lines), and the distance between point S and the center of the femoral tunnel (point O) was measured (blue line).
Statistical Analysis
Statistical analyses were performed with the SPSS Version 20.0 software (IBM). The Pearson chi-square test or Fisher exact test was used to compare the categorical variables. For comparisons of continuous variables, the Student t test or Mann-Whitney U test was used. Moreover, multivariable conditional logistic regression was used to examine the risk factors for MPFL-R failure. The diagnostic value of rotational parameters was evaluated by receiver operating characteristic curve analysis: null (area under the curve [AUC] = 0.5), poorly informative (0.5 ≤ AUC < 0.7), fairly informative (0.7 ≤ AUC < 0.9), highly informative (0.9 ≤ AUC < 1.0), or perfect (AUC = 1.0). 24 No a priori sample size was calculated because this study included all patients with MPFL-R failure at our institute.
Results
Patient Characteristics
The patient characteristics are summarized in Table 1. The mean age was 20.2 ± 4.3 years in the failure group and 20.7 ± 2.4 years in the control group (P = .832). The tibiofemoral rotation angle was significantly higher in the failure group than in the control group (16.4° ± 5.6° vs 6.4° ± 4.5°, respectively; P < .001). Moreover, the TT-TG distance, patellar height, femoral anteversion, incidence of severe trochlear dysplasia, incidence of a high-grade J-sign, and incidence of a femoral tunnel malposition were also significantly higher in the failure group than in the control group. All patients in the failure group underwent isolated MPFL-R.
Patient Characteristics a
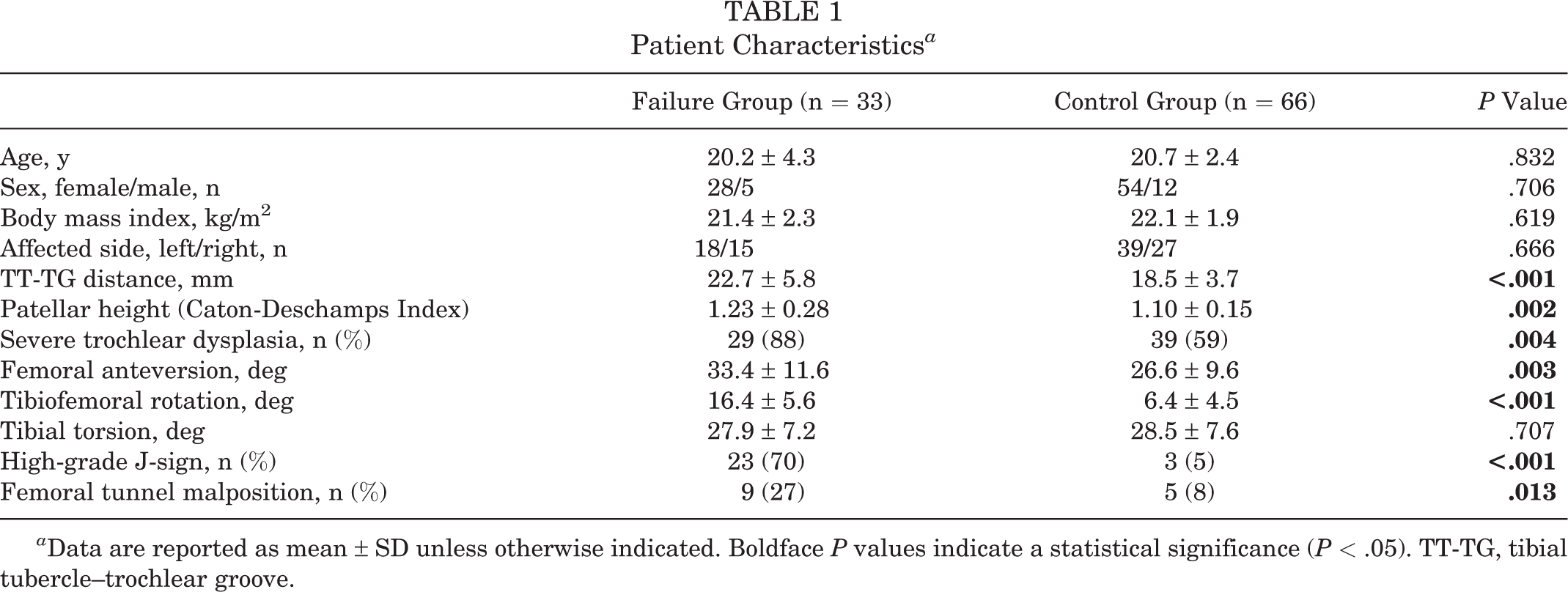
a Data are reported as mean ± SD unless otherwise indicated. Boldface P values indicate a statistical significance (P < .05). TT-TG, tibial tubercle–trochlear groove.
Cutoff Values of Rotational Parameters for Predicting MPFL-R Failure
A receiver operating characteristic curve was drawn to explore the cutoff values and respective AUCs of 3 rotational parameters for predicting MPFL-R failure (Figure 5 and Table 2). Receiver operating characteristic curve analysis showed that the tibiofemoral rotation angle (AUC, 0.920) was highly informative; in contrast, the femoral anteversion angle (AUC, 0.665) and tibial torsion angle (AUC, 0.522) were poorly informative. The cutoff value of the tibiofemoral rotation angle for predicting MPFL-R failure was 12.3° (sensitivity, 81.8%; specificity, 89.4%).
If patients with a femoral tunnel malposition (n = 14) were excluded from receiver operating characteristic curve analysis, the results demonstrated that the tibiofemoral rotation angle was still highly informative for predicting MPFL-R failure, with a higher AUC of 0.938.

Cutoff values of 3 rotational parameters for predicting medial patellofemoral ligament reconstruction failure.
Rotational Parameters for Predicting MPFL-R Failure a

a Boldface P values indicate a statistical significance (P < .05). AUC, area under the curve; MPFL-R, medial patellofemoral ligament reconstruction.
Risk Factors for MPFL-R Failure
A total of 7 variables were included in multivariate logistic regression analysis for risk factors for MPFL-R failure (Table 3). Excessive tibiofemoral rotation (≥12.3°) (odds ratio [OR], 13.159 [95% CI, 2.469-70.139]; P = .003), a high-grade J-sign (OR, 7.674 [95% CI, 1.232-47.809]; P = .029), and a femoral tunnel malposition (OR, 6.976 [95% CI, 1.077-45.187]; P = .042) were identified as risk factors for MPFL-R failure, whereas increased femoral anteversion, patella alta, increased TT-TG distance, and severe trochlear dysplasia were not (Table 4).
Risk Factors for Predicting MPFL-R Failure a

a MPFL-R, medial patellofemoral ligament reconstruction; TT-TG, tibial tubercle–trochlear groove.
Results of Logistic Regression Analysis of Risk Factors for MPFL-R Failure a

a Boldface P values indicate a statistical significance (P < .05). MPFL-R, medial patellofemoral ligament reconstruction; OR, odds ratio; TT-TG, tibial tubercle–trochlear groove.
Characteristics of Patients With Excessive Tibiofemoral Rotation
Overall, 27 patients in the failure group and 7 patients in the control group had excessive tibiofemoral rotation (≥12.3°). The comparison between patients with excessive tibiofemoral rotation (risk group) and those with normal rotation (normal group) is shown in Table 5. All of the parameters except tibial torsion were significantly higher in the risk group than in the normal group.
Characteristics of Patients With Versus Without Excessive Tibiofemoral Rotation a

a Data are reported as mean ± SD unless otherwise indicated. Boldface P values indicate a statistical significance (P < .05). TT-TG, tibial tubercle–trochlear groove.
A moderate linear correlation was found between the tibiofemoral rotation angle and the TT-TG distance (r = 0.545; P < .001). In contrast, no linear correlation was found between the tibiofemoral rotation angle and the femoral anteversion angle (r = 0.269) or tibial torsion angle (r = –0.028).
Discussion
The most important finding of this study was that excessive tibiofemoral rotation, the presence of a high-grade J-sign, and a femoral tunnel malposition were 3 independent risk factors for MPFL-R failure in patients with RPDs. Moreover, a preoperative tibiofemoral rotation angle of ≥12.3° was a reliable predictor of primary MPFL-R failure, which can help surgeons easily and precisely identify high-risk patients of failure before performing MPFL-R.
Few studies have uncovered the possible causes of increased tibiofemoral rotation angles. Theoretically, the tibiofemoral rotation angle can be changed by either an increased femoral anteversion angle or tibial torsion angle. According to the theory proposed by Teitge, 26 when there is excessive femoral anteversion, the trochanter is moved anteriorly in some patients to maintain normal hip abductor muscle strength at the cost of excessive internal rotation of the distal femur. However, in this situation, the proximal tibia will externally rotate for the purpose of maintaining a normal foot progression angle (10°-15°), 15,20 which usually remains stable even in patients with torsional deformities in the lower extremities: This is the most stable position of the foot on the ground. 20 The upshot of all of this is that the distal femur and proximal tibia will rotate in opposite directions, resulting in an increase of the tibiofemoral rotation angle because of the gradual laxity of soft tissue around the knee and the formation of a characteristic sign—the “inwardly pointing knee.” 26 Therefore, to facilitate understanding of the clinical significance of the tibiofemoral rotation angle, it can be regarded as a quantization parameter of the “inwardly pointing knee.” It should be noted that increased femoral anteversion does not always lead to excessive tibiofemoral rotation. In some patients, the distal femur is still pointed forward by means of external rotation of the ipsilateral hip. This changes the effective lever arm of the hip stabilizers and may account for the frequency of soft tissue hip complaints as well as an increased pelvic tilt in these patients. 26 This theory also helps explain why some patients with increased femoral anteversion show good clinical outcomes, whereas others do not, after MPFL-R without derotational osteotomy. 30 Similarly, Kaiser et al 11 also assumed that in cases of increased femoral anteversion, the tension and force vector of the vastus lateralis increase relative tibial external rotation, leading to an increase in the TT-TG distance and therefore tibiofemoral rotation.
The tibiofemoral rotation angle, as an important component of rotational parameters of the lower extremities, has been found to be higher in patients with RPDs than in the healthy population, which indicates that an increased tibiofemoral rotation angle is a potential risk factor for RPDs. 2,5,14,19 However, few studies have further explored the clinical significance of abnormal tibiofemoral rotation in RPDs. Lin et al 14 compared the degree of tibiofemoral rotation in different populations and found that tibiofemoral rotation was correlated with the severity of patellar dislocations, with the greatest value in patients with fixed or obligatory dislocations. Keshmiri et al 12 analyzed the influence of rotational limb alignment parameters on patellar kinematics and demonstrated that tibiofemoral rotation had a significant influence on patellar tracking in cadaveric knees. To our knowledge, our study is the first to directly link abnormal tibiofemoral rotation with MPFL-R failure in the literature, and we found that an increased preoperative tibiofemoral rotation angle can be used as a reliable predictor of MPFL-R failure. It is a challenge to systematically explain the cause-and-effect relationship between abnormal tibiofemoral rotation and MPFL-R failure; however, the following points may partially illuminate the exact mechanisms involved. First, an increased tibiofemoral rotation angle can cause the TT-TG distance to increase, 1,27,28 and a 1° increase in tibiofemoral rotation can approximately increase the TT-TG distance by 0.5 mm. 23 In the present study, a moderate linear correlation was found between the tibiofemoral rotation angle and the TT-TG distance (r = 0.545; P < .001), confirming the close relationship between tibiofemoral rotation and the TT-TG distance. Therefore, it is not surprising that an increased tibiofemoral rotation angle can predict worse clinical outcomes after MPFL-R. Second, several biomechanical and clinical studies have found that increased femoral anteversion can significantly increase the lateralizing force that acts on the patella, and it may be a cause of MPFL-R failure. 7,11,17,34 According to the theory of Teitge, 26 excessive tibiofemoral rotation is a common consequence of increased femoral anteversion. We also found that femoral anteversion was significantly higher in the patients with excessive tibiofemoral rotation (risk group) than in the patients with normal rotation (normal group) (32.5° vs 26.9°, respectively; P = .015), which can help to explain the predictive value of tibiofemoral rotation in MPFL-R failure. Further biomechanical studies are required to understand the underlying mechanisms.
Although an increased tibiofemoral rotation angle may be a reliable predictor of MPFL-R failure in patients with RPDs, little is known about how to surgically correct this kind of rotational deformity in patients with a high risk of failure. Lin et al 14 speculated that it is possible that by surgically re-establishing tension in the MPFL, the increased medialized force vector on the patella exerts enough force to alter the resting rotation of the tibia in relation to the femur. However, there are no studies investigating this phenomenon in the literature. In theory, if increased femoral anteversion is one of the potential causes of abnormal tibiofemoral rotation, does that mean that femoral derotational osteotomy leads to a reduction in the tibiofemoral rotation angle? No study has directly proven or disproven this hypothesis. Tian et al 29 performed 16 femoral derotational osteotomy procedures in patients with RPDs and increased femoral anteversion and found that the TT-TG distance decreased from 15.6 mm preoperatively to 14.7 mm postoperatively. Similarly, in a recent biomechanical study, Kaiser et al 10 found that femoral derotational osteotomy of 5° (toward an absolute norm value of 20°) decreased the TT-TG distance by a factor of approximately 0.6. Derotational osteotomy is performed above the trochlea, and the procedure should not directly change the relationship of the osseous landmarks (trochlear groove and tibial tubercle); therefore, the most plausible explanation is that femoral derotational osteotomy may decrease tibiofemoral rotation and consequently reduce the TT-TG distance. If this hypothesis is confirmed by further clinical studies, femoral derotational osteotomy might be a feasible method to reduce the failure risk of MPFL-R when encountering patients with excessive tibiofemoral rotation, especially considering that these patients usually have increased femoral anteversion (mean, 32.5°).
Given the etiological complexity of RPDs, it is challenging to precisely determine the causes of MPFL-R failure. Currently, technical errors and missed risk factors (eg, trochlear dysplasia, increased femoral anteversion) have been recognized as potential causes of poor outcomes after MPFL-R. 17 The study conducted by Sappey-Marinier et al 18 was the first to collate the relevant factors and systematically evaluate the risk factors associated with MPFL-R failure. The results of their logistic regression analysis highlighted 2 preoperative risk factors for failure: a positive J-sign (OR, 3.9) and patella alta (Caton-Deschamps Index ≥1.3; OR, 4.9). Zhang et al 31 analyzed the risk factors for MPFL graft laxity and found that a preoperative high-grade J-sign and femoral tunnel malposition were associated with graft laxity after MPFL-R. In accordance with these studies, a high-grade J-sign was found to be one of the risk factors for MPFL-R failure in the present study. Therefore, it is crucial to accurately evaluate preoperative patellar tracking, and additional bony procedures should be considered when encountering patients with a high-grade J-sign to guarantee a good clinical outcome. 30,32
The clinical relevance of the present study is as follows: (1) for the first time, this study points out that excessive tibiofemoral rotation was a potential risk factor for MPFL-R failure; (2) the prognostic value of the tibiofemoral rotation angle in MPFL-R was preliminarily confirmed, and excessive tibiofemoral rotation ( ≥12.3°) can predict the failure of primary MPFL-R with a high degree of accuracy, which can help surgeons easily and precisely identify high-risk patients of MPFL-R failure before surgery; (3) the role of a preoperative high-grade J-sign and femoral tunnel malposition in MPFL-R failure was further confirmed; and (4) there is limited evidence about the effect of femoral derotational osteotomy on reducing tibiofemoral rotation, with some evidence suggesting that it might be effective, but it is not conclusive.
Limitations
There are several limitations of this study. First, the retrospective nature of the study design is an inherent limitation. Second, the sample size of the failure group is relatively small (n = 33), which may reduce the power of logistic regression. However, to our knowledge, this is the largest study to systematically analyze the risk factors for MPFL-R failure, including 33 patients in the failure group.
Conclusion
In this study, excessive tibiofemoral rotation, a high-grade J-sign, and a femoral tunnel malposition were identified as risk factors for MPFL-R failure in patients with RPDs. More importantly, excessive tibiofemoral rotation (≥12.3°) may predict the failure of primary MPFL-R, which can help surgeons easily identify high-risk patients of MPFL-R failure before surgery.
Footnotes
Final revision submitted August 3, 2022; accepted September 13, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding for this study was received from the Beijing JST Research Fund (grant QN202202), National Natural Science Foundation of China (grant 82202777), and Capital’s Fund for Health Improvement and Research (grants 2020-1-2071, 2020-2-2075). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Beijing Jishuitan Hospital.