
Abstract
Background:
Injury to the ulnar collateral ligament (UCL) of the elbow can cause chronic pain and loss of throwing ability. Ultrasonic shear wave elastography (SWE) is a new imaging method that can be used for quantitative assessment of tissue elasticity.
Purpose:
To evaluate the properties of the UCL in professional baseball players using SWE.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
This study included 35 professional baseball players (mean age, 23.0 years) without elbow injuries. Both elbows of each player were examined using ultrasound, and comparisons between the dominant and nondominant arms were conducted. The thickness of the anterior bundle of the UCL at its midportion was measured in the resting position on ultrasound. We also measured the difference in the ulnohumeral joint space with and without gravity stress on the forearm. Tissue elasticity was evaluated using a built-in software program. The relationship between UCL elasticity and ultrasound findings was analyzed using the Pearson correlation coefficient.
Results:
The mean ± SD thickness of the UCL was significantly greater in the dominant arm versus the nondominant arm (6.0 ± 1.4 vs 5.3 ± 1.3 mm; P = .004). The mean joint space difference was significantly wider in the dominant arm as compared with the nondominant arm (0.81 ± 0.42 vs 0.52 ± 0.31 mm; P = .002), and the mean UCL elasticity was lower in the dominant arm than in the nondominant arm (34.9 ± 11.6 vs 43.3 ± 10.6 kPa; P = .002). UCL elasticity was negatively correlated with UCL thickness (r = –0.27; P = .02) and joint space difference (r = –0.34; P = .003).
Conclusion:
In professional baseball players, the elbow UCL of the dominant arm demonstrated increased thickness, with a larger joint space gap on gravity stress and lower elasticity in SWE as compared with the nondominant arm. Greater medial joint laxity can be predicted by assessing the elasticity of the UCL using SWE.
Keywords
The ulnar collateral ligament (UCL) is one of the important stabilizers of the medial aspect of the elbow joint. Injury to the UCL can cause chronic pain and loss of throwing ability in athletes, such as baseball players. To prevent throwing injuries, it is important to detect anatomic abnormalities of the UCL before the onset of symptoms. 2 There are several imaging studies related to the elbow UCL. Wright et al 32 used plain elbow radiographs to examine professional baseball pitchers and found that degenerative changes developed over time; however, these changes did not correlate with the time spent on the injured list. UCL abnormalities detected by magnetic resonance imaging are common in asymptomatic professional baseball pitchers. 20 Specifically, increased UCL thickness, signal heterogeneity, or UCL disruptions were present in the pitcher’s dominant arm. Ultrasound imaging is a rapid, cost-effective, and noninvasive tool that can be used to evaluate dominant and nondominant elbows. In addition, valgus stress can be applied during the procedure to provide a more functional assessment of the ability of the UCL to resist joint widening. 12,27 Nazarian et al 24 reported on the usefulness of ultrasound imaging with stress in evaluating the UCL in 26 asymptomatic Major League Baseball professional pitchers. In the pitchers’ dominant elbows, the mean thickness of the anterior band of the UCL was greater; hypoechoic foci inside the UCL bundle were observed, as well as calcification that showed hyperechoic lesions. The ulnohumeral joint widened to a greater degree with valgus stress on the throwing arm.
Ultrasound elastographic techniques have been investigated to quantify the material properties of tissues. 13 Freehand sonoelastography was initially developed to quantify the strain in tissues by measuring displacement under external mechanical compression. 25 Using this technique, previous studies assessed the material properties of the shoulder muscles. 16,23 Although studies have shown good feasibility and reliability of the technique, freehand compression with a consistent load remains a technical challenge, with amplitude and/or velocity of loading compression yet to be established. 5 Shear wave elastography (SWE) is one of the newer imaging techniques based on the following principle: the acoustic radiation force produced by a transducer creates shear waves, and their velocity is then measured as they travel through the tissues. The elasticity of the tissue (Young modulus) is calculated from this velocity. 30 This new imaging method can help in the quantitative assessment of tissue elasticity, and it is different from conventional axial-strain sonoelastography, which requires manual cyclic compression forces to evaluate tissue strain. 21,30 The ability of ultrasonic SWE to measure quantitative values of elasticity has been evaluated using phantoms calibrated for different elasticities, and reliable results were obtained. To date, it has been used successfully for breast cancer diagnosis 3,26 and liver fibrosis staging. 10,33 In addition, quantitative assessments of material properties of muscles have been investigated by in vivo and in vitro studies. 1,17,19,22 Several authors used SWE to evaluate the elasticity of Achilles tendons. 30 These studies concluded that the Achilles tendon in patients with tendinopathy was significantly softer than in those with normal tendons. 30 A study that used SWE on the elbow UCL in healthy volunteers concluded that mean shear wave velocity was similar between dominant and nondominant arms. 11 So far, there have been no reports regarding the use of SWE in baseball players’ elbows.
The purpose of this study was to evaluate the UCL in professional baseball players using SWE. Our hypothesis was that UCL elasticity of the dominant arm would be lower with medial elbow joint laxity than that of the nondominant arm.
Methods
A total of 35 new professional baseball players aged 18 to 26 years (mean, 23.0 years) participated in this study between December 2017 and December 2019. The players had played baseball for 8 to 18 years and none of them had a history of elbow joint problems. Institutional review board approval was received, and all participants provided informed consent.
For the ultrasound assessment, the patients were positioned supine with 90° of abduction at the shoulder and 30° of flexion at the elbow. A commercial ultrasound system (Aixplorer; Konica Minolta) was used to perform ultrasound examinations. A 12-MHz liner probe was aligned along the long axis of the anterior oblique band of the UCL. The thickness of the anterior bundle of the UCL at its midportion was measured without stress on the elbow. 2,18 The width of the ulnohumeral joint space at the level of the anterior bundle was measured at rest and under gravity stress (Figure 1A). Measurements were made on the ultrasound screen using electronic calipers, with a precision of 0.1 mm. The joint space difference was calculated as follows: joint space under gravity stress – joint space without gravity stress.
Tissue elasticity was measured using built-in software to obtain the elastic modulus (in kilopascals) for each region (Figure 1B). To minimize any technical variation arising from probe positioning or pressure, SWE values were measured 3 times, as previously described. 14 The mean SWE values were calculated for all regions from these images to obtain the elastic modulus of the UCL region. All measurements were performed by 2 senior orthopaedic surgeons (A.I. and Y.M.) with 8 and 9 years of experience, respectively, in the clinical use of ultrasonography. The intra- and interobserver reliabilities were investigated using ultrasound measurement techniques. For intraobserver calculations, measurements were made 2 hours apart within the same day.

(A) The ulnar collateral ligament (UCL) as shown on B-mode ultrasound. UCL thickness (arrow) and joint space distance (arrowhead) were measured using a digital caliper. (B) Heat map of elasticity distribution on shear wave elastography (SWE) ultrasound.
Correlations were analyzed between UCL elasticity and UCL thickness, as well as UCL elasticity and joint space difference. Correlations were also analyzed between age and UCL thickness, joint space difference, and UCL elasticity.
Statistical Analysis
All data are expressed as mean and standard deviation. Data from the players’ dominant and nondominant arms were compared using paired t tests. The relationship between UCL elasticity and UCL thickness or joint space difference was analyzed using the Pearson correlation coefficient. Statistical significance was set at P < .05. The results were statistically analyzed using SPSS (Version 27.0; IBM) and RStudio (RStudio PBC).
Reliability tests for measurement of the thickness, joint space difference, and elasticity between the examiners were performed using RStudio, and intra- and interobserver reliability was examined using the intraclass correlation coefficient, interpreted as poor (<0.40), moderate (0.40-0.60), good (0.61-0.80), or excellent (>0.80).
Results
Reliability of Ultrasound Measurements
Intraclass correlation coefficients for measurements of UCL elasticity, UCL thickness, and joint space difference were 0.78, 0.99, and 0.98 for intraobserver reliability and 0.71, 0.99, and 0.91 for interobserver reliability, respectively. The results indicated good to excellent intra- and interobserver reliability.
Comparison of Ultrasound Measurements
The mean ± SD thickness of the UCL was significantly greater in the dominant arm versus the nondominant arm (6.0 ± 1.4 vs 5.3 ± 1.3 mm; P = .004) (Figure 2A). The mean joint space difference was significantly greater in the dominant arm than the nondominant arm (0.81 ± 0.42 vs 0.52 ± 0.31 mm; P = .002) (Figure 2B). The mean UCL elasticity was significantly lower in the dominant arm as compared with the nondominant arm (34.9 ± 11.6 vs 43.3 ± 10.6 kPa; P = .002) (Figure 2C).
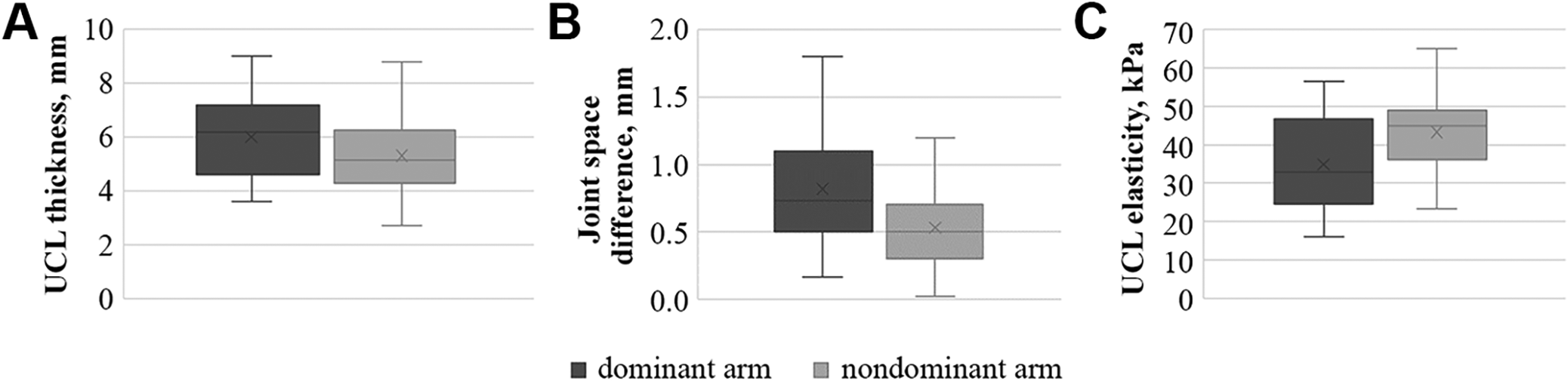
Box plots show (A) UCL thickness, (B) joint space difference, and (C) UCL elasticity between the dominant and nondominant arms. ×, mean value; middle line, median; box, interquartile range; whiskers, 95% CI. UCL, ulnar collateral ligament.
Results of Correlation Analysis
Correlation analysis indicated that UCL elasticity had a significant negative correlation with UCL thickness (r = –0.27; P = .02) (Figure 3A) and joint space difference (r = –0.34; P = .003) (Figure 3B). No significant correlation was found between age and UCL thickness (dominant arm, r = –0.07; P = .65; nondominant arm, r = 0.003; P = .98), joint space difference (dominant arm, r = –0.02; P = .88; nondominant arm, r = –0.15; P = .36), or UCL elasticity (dominant arm, r = –0.02; P = .90; nondominant arm, r = –0.20; P = .22).

Significant correlations were found between (A) UCL elasticity and UCL thickness (r = –0.27; P = .02) and (B) UCL elasticity and joint space difference (r = –0.34; P = .003). UCL, ulnar collateral ligament.
Discussion
The present study investigated the properties of the UCL using SWE in professional baseball players and revealed that the UCL of the dominant arm was thicker (P = .004) and had lower elasticity (P = .002) with a wider joint space difference (P = .002) as compared with the nondominant arm. Moreover, UCL elasticity was negatively correlated with UCL thickness (r = –0.27; P = .02) and joint space difference (r = –0.34; P = .003). These results indicate that larger medial joint laxity can be predicted by assessing the elasticity of the UCL using SWE. To the best of our knowledge, this is the first study to report such properties.
Baseball pitchers have a high risk of UCL injuries because of the tremendous forces imparted on their elbows during the action of throwing. These injuries may occur acutely or as a result of chronic repetitive stress. 4,7 Therefore, prediction of UCL injuries before the onset of symptoms to provide a functional assessment of the UCL. 6,8,27 Ultrasound with valgus stress has demonstrated the importance of the anterior bundle of the UCL and the flexor-pronator mass on ulnohumeral joint stability. 8 Another study involved the application of stress ultrasound on 30 asymptomatic collegiate baseball players. The results of the study showed that the ulnohumeral joint space of the dominant elbow was significantly wider than that of the nondominant elbow and illustrated increased gapping with valgus stress. 27 The B-mode imaging results in the current study were similar. Repetitive stretch stress may lead to minor trauma to the UCL. After remodeling, ligament thickness increases. This might be one of the first changes to develop in young baseball pitchers. 2 Wada et al 31 conducted comparative studies of elbow UCL elasticity using strain elastography, which is another technique to assess the mechanical properties of the UCL. They evaluated baseball players in junior high school, high school, and university, all without any history of a pitching injury. The study using ultrasound strain elastography revealed that elbow UCL elasticity was greater in the pitcher’s dominant arm and decreased with increasing age. Ciccotti et al 6 performed a 10-year prospective stress-ultrasound evaluation of 368 asymptomatic professional pitchers. The authors found that the mean thickness of the UCL was greater in the pitcher’s dominant arm and that the dominant elbow had significantly greater joint gapping with the addition of valgus loads. There was a trend of greater UCL thickness, wider joint space gapping with valgus stress, and an increased proportion of players with hypoechoic foci and calcifications in the UCL-injured cohort as compared with the asymptomatic pitchers. In our study, UCL thickness was greater in the dominant arm with a larger joint space difference under gravity stress. These results are compatible with those of previous reports.
SWE can analyze the mechanical properties of tissues or organs in a noninvasive manner. 26,30,34 The reliability and validity of elastographic measurements have been investigated in several studies. 26,34 Hatta et al 13 reported that SWE measurements might provide reliable material property measurements by aligning the transducer imaging plane with the muscle fiber orientation. Several studies involving SWE on human tendons 9,29,30 and muscles 15,17,28 suggested that shear waves propagate faster in (1) healthy tendons versus those inflicted with tendinopathy and (2) contracted tendons and muscles versus those that are relaxed. The Achilles tendons with tendinopathy or torn tendons had significantly lower shear wave velocity than the normal tendons. Since shear wave velocity positively correlated with tissue stiffness, these studies demonstrated that the healthy tendons may be stiffer than the pathological ones. 30 Wu et al 33 evaluated the thickness and elasticity of the coracohumeral ligament (CHL) in healthy participants and in patients with a clinical diagnosis of unilateral adhesive capsulitis of the shoulder. The authors reported that increased thickness and stiffness of the CHL were observed in the symptomatic shoulder versus the unaffected side. The authors suggested that the increased stiffness of the CHL in patients with adhesive capsulitis may be associated with a limited range of motion during external rotation of the glenohumeral joint. In a study that performed SWE on the elbow UCL, 11 healthy volunteers underwent ultrasound examination, and the shear wave velocity was compared between the dominant and nondominant arms; the mean shear wave velocity of the elbow UCL was similar between them. 11 In the present study, we performed an analysis on professional baseball players with a playing career of 8 to 18 years. The results of our study showed that the UCL of the dominant arm was thicker and had lower elasticity with a wider joint space difference. There were weak negative correlations between UCL elasticity and joint space difference or UCL thickness. Repetitive stress on a baseball pitcher’s throwing elbow was considered to decrease ligament elasticity and increase UCL thickness and joint laxity of the medial aspect (ie, a wider joint space difference without symptoms). The results indicated that greater laxity of the medial joint can be easily predicted by measuring elasticity of the UCL using SWE without measurements of joint space difference, which may lead to the prediction of UCL injuries before the onset of symptoms.
Limitations
This study has several limitations. First, a standardized method for assessing ligament or tendon elasticity has not been developed. Musculoskeletal elastography remains in its infancy, and there are limited and sometimes conflicting data regarding normative values for elasticity in ligaments and tendons. As we do not have a musculoskeletal ultrasound technician or musculoskeletal radiologist in our hospital, 2 orthopaedic surgeons skilled in musculoskeletal ultrasound (A.I. and Y.M.) conducted the ultrasound examinations in the present study, which resulted in high intra- and interobserver reliability. However, another study reported poor repeatability. 11 In addition, tissue elasticity measurements by elastography can be made only during the examination, before image storage. Second, although SWE is widely used to analyze musculoskeletal conditions, no cadaveric study has analyzed the relationship between SWE findings and the mechanical properties of elbow ligaments. Finally, this study focused on new professional baseball players with no symptoms at the initiation medical checkup. Therefore, we will clarify the significance of using SWE for the UCL by conducting ongoing medical checkups and examinations of UCL-injured players.
Conclusion
In professional baseball players, the UCL of the dominant arm demonstrated increased thickness with a larger joint space gap on gravity stress and lower elasticity in SWE as compared with the nondominant arm. Our results suggest that greater medial joint laxity can be predicted by measuring the elasticity of the UCL using SWE. It is hoped that SWE can be used to predict UCL injury and help guide treatment decisions.
Footnotes
Acknowledgment
The authors thank Editage for the English-language editing.
Final revision submitted August 29, 2022; accepted September 8, 2022.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Kobe University Graduate School of Medicine (No. B210009).