
Abstract
Background:
Little attention has been paid to playing position as a risk factor for recurrence after arthroscopic Bankart repair (ABR) in soccer players.
Purpose:
To compare return to sport, functional outcomes, and recurrence after ABR between goalkeepers and field position players in soccer.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A retrospective comparative cohort study was performed in soccer players who underwent ABR between January 2017 and December 2019. The minimum clinical follow-up was 2 years. Functional outcomes included the Rowe score, visual analog scale (VAS) for pain, and shoulder-dependent sports ability measured with the Athletic Shoulder Outcome Scoring System (ASOSS). The difference between the post- and preoperative scores was calculated; rate and level of return to sport, recurrent instability, and revisions were also evaluated according to position played.
Results:
A total of 70 position players and 11 goalkeepers met the study criteria. Postoperative functional outcomes were significantly improved in both groups as compared with baseline (P < .001 for both), although the position players achieved significantly greater pre- to postoperative improvement (ΔVAS, –2 vs 0 points [P = .029]; ΔRowe, 45 vs 30 points [P = .046]; ΔASOSS, 45 vs 40 points [P = .028]). While all players returned to soccer, only 55% (n = 6) of goalkeepers returned to the same level versus 93% of field players (P = .003). The overall rate of recurrent instability was 8.6% but was significantly higher among goalkeepers (27.2% vs 5.7%; P = .049), and the odds of goalkeepers having a recurrence were significantly higher than field position players (odds ratio, 8.5 [95% CI, 1.2-57.2]; P = .027).
Conclusion:
Although the results of ABR were generally favorable in all soccer players, goalkeepers had significantly worse functional outcomes, a lower rate of return to the same level of sport, and a higher recurrence rate as compared with field position players.
Soccer is one of the most popular sports, played by >200 million people worldwide. 10 Considering that it is a contact sport, there is a high risk of injury, particularly related to the lower limb. 18 However, modern soccer tactics (ie, higher speeds, pressing, and marking) have resulted in a more physically demanding sport with increased friction between players, which has contributed to higher incidences of upper extremity injuries. 27
The most common upper extremity injuries among soccer players are shoulder injuries. 22 Glenohumeral instability is a frequent upper extremity injury and is of extreme importance, as it has been linked to the longest layoff time among soccer players. 22 An arthroscopic Bankart repair (ABR) is an appropriate surgical approach for the treatment of anterior shoulder instability when the glenoid bone deficit does not exceed 20% to 25%. 36 However, the recurrence rate after ABR varies widely in literature, with rates between 2% and 40%. 20 For this reason, some authors have advocated an open Bankart procedure or a bone-block procedure for athletes involved in collision sports. 16,30
Several risk factors have been associated with a higher risk of recurrence after ABR, such as age, contact/collision sport, and participation in competitive sports. 13,19,21,23,28,37 The position of the soccer player on the field may also be a risk factor for recurrence. 2,33 For example, in rugby, a player’s position has been shown to significantly affect the recurrence rate after ABR. 25 In soccer, goalkeeper roles differ significantly from the other field positions. 10 Whether throwing the ball, reaching overhead, or diving for the ball, goalkeepers are more prone to shoulder injuries. 4 Indeed, it has been reported that goalkeepers have a 5-times higher incidence of sustaining upper extremity injuries as compared with field players. 10 However, little attention has been paid to analyzing soccer players’ on-field position as a potential risk factor for recurrence after ABR.
The purpose of this study was to compare functional outcomes, return to sport, and recurrence after ABR between goalkeepers and field positions in soccer. Our hypothesis was that goalkeepers would have a significantly higher recurrence rate than field positions after ABR. We also hypothesized that, given the higher demand placed on the shoulder in goalkeepers, functional outcomes and return to sport would be different when compared with field players.
Methods
A retrospective comparative cohort study was performed in patients who underwent ABR between January 2017 and December 2019 at a single institution. The study protocol was approved by the ethics committee of our institution, and all patients provided informed consent to participate in this investigation. The study inclusion criteria were recreational or competitive soccer players, at least 1 episode of instability while playing soccer (dislocation or subluxation), and a minimum follow-up of 24 months. Exclusion criteria were as follows: participation in other collision/contact or overhead sports, age >40 years, bony defects >20% on the anteroinferior portion of the glenoid based on preoperative computed tomography scan, 5 engaging Hill-Sachs lesions at 90° of abduction and 90° of external rotation based on arthroscopic examination, 3 HAGL lesions (humeral avulsion of the glenohumeral ligament), associated SLAP lesions (superior labral from anterior to posterior), posterior labral tears, rotator cuff injuries, multidirectional instability, bony Bankart, or previous surgery on the same shoulder.
The included patients were divided into 2 groups according to player position: goalkeepers and field position players. 15
Surgical Technique
All ABRs were performed in the lateral decubitus position with combined general endotracheal and regional anesthesia by 3 surgeons (M.R., L.A.R., I.T.). A complete mobilization of the labrum was performed beyond the 6-o’clock position, followed by removal of 2 to 3 mm of the anterior glenoid cartilage for subsequent anchor placement. Labral repairs were performed with a knotted anchor technique with simple sliding knots. Typically, 3 anchors single loaded with No. 2 nonabsorbable sutures (CrossFT; ConMed) were placed on the cartilage edge of the glenoid surface (mean, 3.2; range, 2-4). The first was placed in the inferior area of the anterior glenoid rim below the 5-o’clock position. Additional anchors were placed in a similar manner at the 3- and 4-o’clock positions (Figure 1). No patients in this series underwent concomitant posterior-inferior capsulolabral repair, rotator interval closure, SLAP repair, or remplissage.

Arthroscopic view of a right shoulder from the posterior subacromial viewing portal. (A) Bankart lesion at 5 to 6 o’clock. (B) Completed Bankart repair.
Rehabilitation
A standardized postoperative physical therapy and rehabilitation program was used. The arm was supported in a sling for 4 weeks. After 1 week, supervised gentle physical therapy consisting of gradual passive range of motion was initiated. Active-assisted range of motion exercises began 2 weeks after surgery. When the patient could perform active forward elevation above the shoulder level, strengthening was initiated. Running was allowed at 8 weeks. Return to sport was allowed when the patient was pain free without apprehension, full shoulder range of motion had been achieved, and shoulder strength was near the same as before the injury, typically at 4 months postoperatively.
Clinical Evaluation
Pre- and postoperative evaluations consisted of a patient-based questionnaire and a physical examination performed by a shoulder fellow (I.P.) who did not participate in the surgical procedure. The Rowe score was used as a global outcome measure. 31 Shoulder-dependent sports ability was measured with the Athletic Shoulder Outcome Scoring System (ASOSS). 32 We evaluated whether patients achieved the minimal clinically important difference for the Rowe score (ie, an increase from baseline of at least 9.7 points). 24 The difference between the post- and preoperative scores (Δ) was also calculated.
Instability was evaluated with apprehension and relocation tests performed at the preoperative evaluation and the final follow-up. Anterior hyperlaxity was defined as external rotation >90° with arms at the side (reaching the frontal plane), and inferior laxity was determined through use of the Gagey hyperabduction test. 6,11 Radiographs and magnetic resonance imaging were performed in all cases. If, during these studies, bony defects were suspected, computed tomography was ordered to evaluate the magnitude. The preoperative glenoid bone loss was measured with the glenoid index method according to Chuang et al. 5
At the final follow-up, patients were asked if they had been able to return to their previous sports, if they had been able to perform them at the same levels as before the dislocation, and if they decided to change their positions on the field (yes/no responses for all). All surgery revisions were documented. Recurrence was defined as the presence of dislocation, subluxation, or apprehension during the follow-up physical examination that limited daily activities or sports. 20
Statistical Analysis
Continuous variables were summarized as means and standard deviations or medians and interquartile ranges according to distribution, and categorical variables were summarized as absolute and relative frequencies. The t test and Mann-Whitney test were used to compare the means or medians of the quantitative variables between the groups. The chi-square test or the Fisher exact test was used according to its assumptions to compare the proportions of the categorical variables between the groups. A crude and adjusted regression analysis was performed to evaluate the effect of the playing position on recurrence. The adjusted regression model was used to treat potential confounders considered by statistical significance or clinical relevance. The odds ratio (OR) was presented with its 95% CI and P value. A post hoc power analysis showed that the power for detecting a difference in recurrence rates between goalkeepers and field soccer positions was 60%. The statistical analysis was performed using Stata Version 13 (StataCorp) with P <.05 considered statistically significant.
Results
Study Population
A total of 103 soccer players underwent ABR after an instability event during the study period. Of these, 14 patients were excluded because they did not meet inclusion criteria, and 8 were lost to follow-up. Thus, complete follow-up was available in 81 of 89 (91%) patients: 11 in the goalkeeper group and 70 in the field position group (Figure 2). There were no differences in baseline demographics or function between groups (Table 1). Moreover, no differences were found in baseline characteristics among the field positions (defenders, midfielders, and forwards) (Table 2).

Flowchart of the patient-selection process. HAGL, humeral avulsion of the glenohumeral ligament; SLAP, superior labral from anterior to posterior.
Baseline Characteristics by Position Group a

a Data are reported as % (No.) or median (interquartile range) unless otherwise indicated. ASOSS, Athletic Shoulder Outcome Scoring System; VAS, visual analog scale.
b Median (range).
Baseline Characteristics Among Field Position Players (n = 70) a

a Data are reported as % (No.) or median (interquartile range) unless otherwise indicated. ASOSS, Athletic Shoulder Outcome Scoring System; VAS, visual analog scale.
b Median (range).
Functional Outcomes
In both groups, postoperative functional outcomes were significantly improved versus baseline (P < .001 for both), and postoperative improvement in Rowe score exceeded the minimal clinically important difference in all patients. However, the field position group achieved significantly greater pre- to postoperative improvement (ΔVAS, –2 vs 0 points [P = .029]; ΔRowe, 45 vs 30 points [P = .046]; ΔASOSS, 45 vs 40 points [P = .028]). Postoperative functional outcomes by position group are shown in Table 3.
Postoperative Outcomes by Position Group a
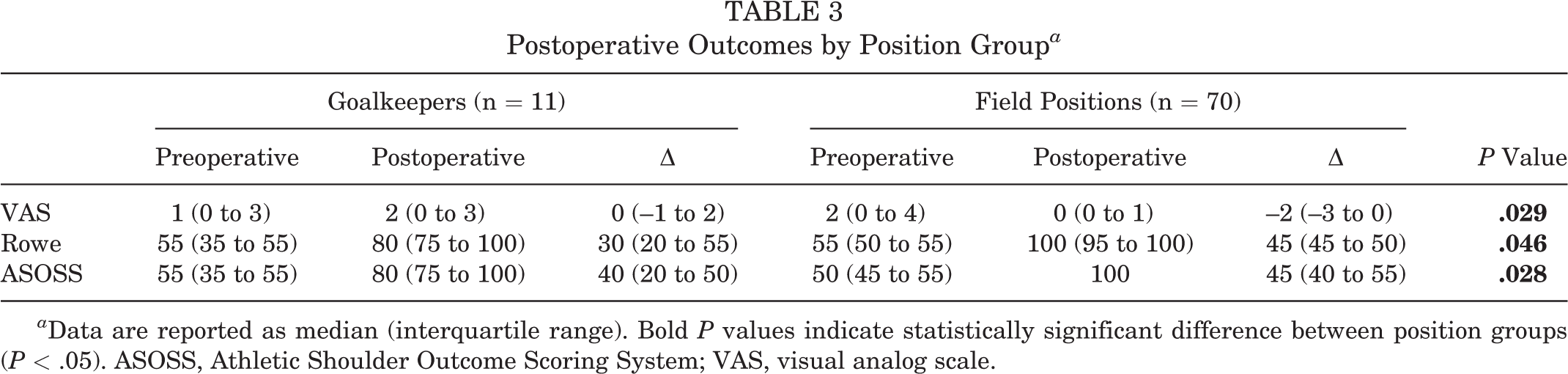
a Data are reported as median (interquartile range). Bold P values indicate statistically significant difference between position groups (P < .05). ASOSS, Athletic Shoulder Outcome Scoring System; VAS, visual analog scale.
Return to Sport
All patients returned to sports at a median 5 months after ABR (interquartile range, 4-6 months). No player changed positions. Overall, 71 players (85.5%) returned at the same level as before the injury. However, the rate of return to the same level of sport was significantly lower in the goalkeeper group versus the field position group (55% vs 93%, P = .003) (Table 4).
Return-to-Sport Outcomes by Position Group a
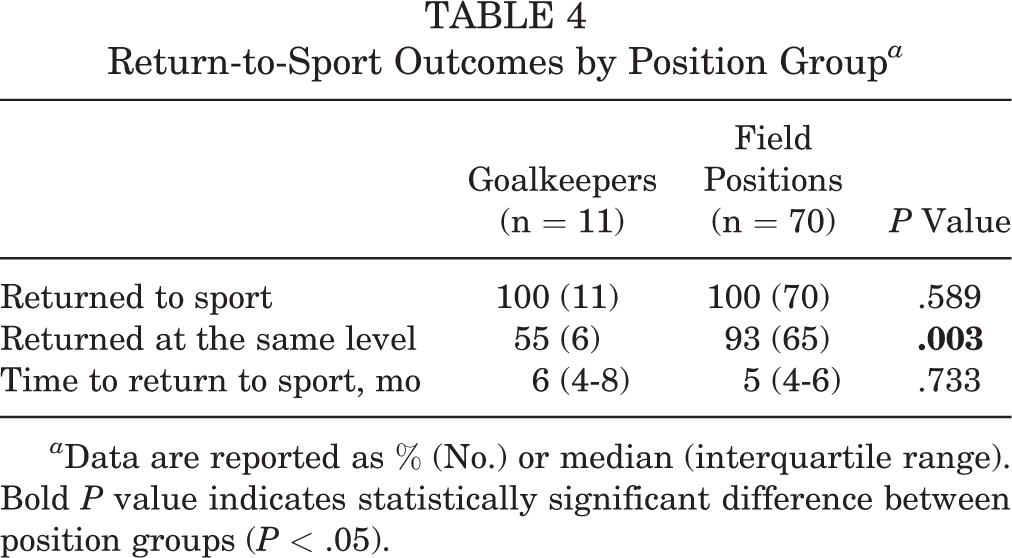
a Data are reported as % (No.) or median (interquartile range). Bold P value indicates statistically significant difference between position groups (P < .05).
Recurrence and Revision
The overall recurrence rate was 8.6%, with all recurrences attributed to traumatic episodes during soccer competition or training. The rate of recurrence was significantly higher in the goalkeeper group versus the field position group (27.2% vs 5.7%, respectively; P = .049). Moreover, the odds of recurrence were significantly higher in goalkeepers (crude OR, 6.1 [95% CI, 1.1-32]; P = .032; adjusted OR, 8.5 [95% CI, 1.2-57.2]). The type of athlete, age, and follow-up were considered for the adjusted model as potential confounders. Overall, 4.9% of players (n = 4) underwent revision surgery, with no differences between position groups (goalkeepers, 9% [n = 1]; field players, 4.2% [n = 3]; P = .449).
Discussion
The primary finding of this study was that goalkeepers had worse outcomes than field position soccer players after ABR. Goalkeepers were 8.5 times more likely to sustain recurrent instability, and they had significantly worse postoperative functional scores and returned to sport at a lower level than position players. These findings have important implications for the management of anterior glenohumeral instability based on position in soccer.
Unlike field position players, goalkeepers stop high-velocity shots with their hands, dive with outstretched arms, and forcefully throw balls, all of which puts them at increased risk of shoulder injury. 14 Several authors have reported that goalkeepers have a higher risk of injury than other positions. 7,10,14,22 For instance, Ekstrand et al 10 stated that goalkeepers had a 5-times increased risk of experiencing an upper extremity injury as compared with field position players. Similarly, Goodman et al 14 found that goalkeepers are 21.3 times more likely to sustain shoulder and elbow injuries during practice than other field position players. The authors noted that the characteristics of the injuries in goalkeepers were different. Specifically, they were more likely to be injured when impacting an object such as the goalposts and sustained noncontact injuries at a higher rate than other positions. Given these unique functions and risk of injury, we believe that goalkeepers should be evaluated separately from other soccer positions.
Recurrence rates after ABR in contact sport athletes vary between 4% and 49%. 20,32,35 Some authors have cited specific recurrence rates in soccer players. Alentorn-Geli et al 1 analyzed 57 male soccer players after ABR using knotless suture anchors and found a 10.5% rate of recurrence during soccer or other unrelated activities. Similarly, Gibson et al 12 reported a recurrence rate of 9% in 34 professional soccer players. Our overall recurrence rate of 8.6% after ABR is thus consistent with the literature. However, we observed substantial differences based on position. Considering the higher frequency of impacts and blows that goalkeepers endure, as well as the greater demands to which they are exposed as compared with field players, we believe that this is the main reason for a higher rate of recurrence episodes in goalkeepers. This is also supported by the fact that all recurrence episodes were traumatic. Moreover, the type of injury and risk factors present in each group, such as age, number of previous dislocations, number of anchors, type of sport, and previous competitive level, were similar between the groups.
A few small series have evaluated the surgical outcomes of goalkeepers. In a series of 19 professional goalkeepers treated with a combination of techniques, Castagna et al 4 reported that while 95% returned to play, 21% had persistent symptoms after surgical stabilization. Terra et al 34 evaluated 12 goalkeepers treated arthroscopically and observed a recurrence rate of 20% after ABR for a first dislocation and 42.8% after ABR for recurrent instability. One limitation of these studies is that neither had a control group, so it is difficult to tell if outcomes were related to other factors, such as surgical technique. On the contrary, with the use of a control group with a consistent surgical technique, we observed that goalkeepers were 6.1 times more likely to experience recurrence than field position players. In light of this, we believe that shoulder surgeons should consider other surgical approaches for goalkeepers, such as remplissage or Latarjet. 8,17,29,30 A recent study compared ABR and Latarjet procedures for competitive rugby players with glenohumeral instability and <20% glenoid bone loss. 30 The authors stated that the ABR and the Latarjet procedure produced excellent functional outcomes, with most athletes returning to sport at the same level that they had before the injury. However, the Bankart procedure was associated with a significantly higher rate of recurrence (20% vs 4%) and reoperation (16% vs 4%) than the Latarjet procedure.
Another alternative that has proven to be effective in reducing the percentage of recurrences is remplissage associated with Bankart repair. In a recent systematic review, Hurley et al 17 reported that ABR with remplissage was associated with a lower rate of recurrent instability when compared with ABR alone in patients with Hill-Sachs lesions and subcritical glenoid bone loss. However, further research is needed to determine whether remplissage may be an effective treatment option for collision athletes without engaging Hill-Sachs lesions.
Overall, functional outcomes and rate of return to sport after ABR in soccer players are high. 1,26 Alentorn-Geli et al 1 cited a return-to-sport rate of 86%, with 73% of players returning to their preinjury levels at a median 4 months postoperatively. Our findings are similar: 100% of patients returned to soccer and 85.5% returned to the same levels of play at a median 5 months postoperatively. To date, however, return to sport based on soccer position has not been reported. Whereas 93% of field position players returned to the same levels of play, only 55% of goalkeepers did so. Similarly, we observed overall excellent postoperative outcomes but less improvement in goalkeepers versus field position players. These results once again highlight the importance of a position-specific treatment approach and/or postoperative rehabilitation program. 9
Limitations
This study presents some limitations that should be mentioned. First of all, given the small sample size in goalkeepers, there is a possibility of a type 1 error. Additionally, since multiple comparisons were conducted, a corrected P value may be required. The correction should be based on functional outcomes, return to sport, and recurrences (P = .05/3). As a consequence, only our findings on return to the same level would remain statistically significant. Second, as a retrospective study, it has all the limitations inherent to this design. Third, although the main objective was to demonstrate that goalkeepers are at greater risk of recurrence than other on-field players, we were not able to analyze the risk of recurrence according to each playing position (goalkeepers, defenders, midfielders, forwards) because of the low sample size. However, we evaluated preoperative characteristics among the 3 field positions to generate 2 comparable groups to help avoid potential confounders in the study. Further analysis could be considered in future work. Fourth, we did not compare outcomes based on treatment approach. Other approaches, such as remplissage or Latarjet, may lead to improved outcomes in goalkeepers. Finally, evaluation of “subcritical bone loss” and the size of the Hill-Sachs lesion were not performed.
Conclusion
Although the results of ABR were generally favorable in all soccer players, goalkeepers had significantly worse functional outcomes, a lower rate of return to the same level of sport, and a higher recurrence rate when compared with field position players. This information may be useful for preoperative counseling and modifying treatment approaches based on position in soccer.
Footnotes
Final revision submitted August 21, 2022; accepted August 30, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: P.J.D. has received consulting fees and royalties from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Hospital Italiano de Buenos Aires (No. 6738).