
Abstract
Background:
Elbow arthroscopic surgery has been popularized and has made significant progress during the past 3 decades. The elbow joint is relatively small and is in close proximity to many neurovascular structures. These factors make elbow arthroscopic surgery technically demanding and liable to complications.
Purpose:
To evaluate the rate of complications after elbow arthroscopic surgery.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines were followed to perform this systematic review and meta-analysis. PubMed, Web of Science, and Embase were searched up to July 2021. All clinical studies that reported complications after elbow arthroscopic surgery were included; a total of 1208 articles were initially found. Case reports, reviews, abstracts, imaging studies, technique studies, nonclinical studies, and those not reporting postoperative complications were excluded. Complication rates were pooled across studies and reported as percentages. Complications were expressed as weighted proportions with 95% CIs.
Results:
A total of 95 studies (14,289 elbows) were included in the meta-analysis. The overall weighted complication rate was 11.0% (95% CI, 8.8%-13.5%), with postoperative stiffness being the most commonly encountered complication (4.5% [95% CI, 2.1%-7.6%]; 158/8818 procedures). The second most encountered complication was the need for subsequent surgery with a weighted proportion of 4.1% (95% CI, 2.9%-5.6%; 177/8853 procedures) followed by nerve injury with a weighted proportion of 3.4% (95% CI, 2.6%-4.3%; 267/13,725 procedures). The ulnar nerve was the most commonly injured nerve (2.6% [95% CI, 1.9%-3.4%]; 123/6290 procedures).
Conclusion:
The results of this study showed that elbow arthroscopic surgery is a relatively safe procedure with low complication rates.
Elbow arthroscopic surgery was first introduced in 1931 and initially considered as a diagnostic tool for various elbow abnormalities. 70 Nowadays, because of the recent advancements in equipment and improved techniques in elbow arthroscopic surgery, its utilization has gained more popularity and accounts for 11% of all arthroscopic procedures, with a 2-fold increase over the past decade. 10 Elbow arthroscopic surgery has gained popularity as the preferred method to manage several intra- and extra-articular elbow conditions. 10,70 It is widely utilized in loose body extraction, synovectomy, synovial biopsy, osteophyte removal, contracture release, osteochondral defects, and lateral epicondylitis. Additionally, indications have expanded to address complex conditions such as radial head resection, arthroscopically assisted open reduction of intra-articular fractures, total synovectomy, and ligament repair/reconstruction. 8,46,80
Elbow arthroscopic surgery is technically demanding because of the complexity of the elbow joint’s geometry and the proximity of major neurovascular structures. 28 The reported complications for elbow arthroscopic surgery include neurological injuries, postoperative stiffness, infections, wound-healing complications, nerve injuries, subsequent procedures, and instability. Risk factors for complications have also been described, including a history of trauma, prior elbow surgery, inflammatory arthritis, hypercoagulable disorders, and intra-articular corticosteroid injections at the time of surgery. 6,55,86 Identifying risk factors that result in complications, pathological considerations, technical considerations (learning curve), anatomy principles, proper portal selection, and adequate patient positioning are key to reduce further complications. 47,97 However, there are still some concerns regarding the potential complications of elbow arthroscopic surgery, especially regarding nerve injuries and elbow stiffness.
Because the indications and utilization of elbow arthroscopic surgery have increased dramatically, the purpose of this study was to collect all the reported complications of elbow arthroscopic surgery. We hypothesized that elbow arthroscopic surgery would be a relatively safe procedure with low complication rates.
Methods
This review was conducted with adherence to the guidelines of the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses). 61
Eligibility Criteria
The inclusion criteria comprised clinical studies that reported complications of elbow arthroscopic surgery. The exclusion criteria were abstracts, case reports, reviews, nonclinical studies, imaging studies, technique studies, and those not reporting postoperative complications.
Information Sources and Search Strategy
PubMed, Web of Science, and Embase were searched up to July 2021. The search keywords used in each database were (“Elbow”) AND (“Arthroscopy”) NOT (“Shoulder”) NOT (“Wrist”) NOT (“Hip”) NOT (“Knee”) NOT (“Ankle”). Studies were screened by titles and abstracts. A full-text review was performed if a study matched the eligibility criteria. Overall, 2 authors (A.F.A. and O.Z.A.) performed the search independently, and the senior author (B.A.Z.) resolved any disagreement.
Data Collection Process and Data Items
The baseline data items that were collected included author(s), study year, level of evidence, age, patient position (prone, lateral, or supine), number of elbow arthroscopic procedures, and elbow complications. The elbow complications were infections, wound-healing complications, nerve injuries, subsequent procedures, instability, and stiffness. Infections were either superficial or deep infections. Wound complications entailed wound dehiscence or drainage. Nerve complications were injuries to the ulnar nerve, radial nerve, posterior interosseous nerve, median nerve, medial antebrachial cutaneous nerve, and lateral antebrachial cutaneous nerve (LABCN) as well as total nerve injuries and unspecific nerve injuries. Again, 2 authors (A.T.H. and A.T.) performed data extraction independently.
Statistical Analysis
A quantitative synthesis was performed using Stata/IC (StataCorp). The continuous variables of baseline patient demographics were reported as means or ranges, whereas categorical variables were reported as unweighted proportions. Complications were expressed as weighted proportions for total complications and for each individual complication with 95% CIs. An arcsine transformation was implemented to compute weighted proportions, which managed variance instability; it is one of the preferred transformation methods in meta-analyses of prevalence. 8
Results
Study Selection
The search strategy resulted in 1208 articles, of which 310 duplicates were removed, thus leaving 898 articles for searching by titles and abstracts. A total of 767 articles were excluded, resulting in 131 articles eligible for full-text reviews. Of the 131 articles, 36 articles were excluded, leaving 95 eligible articles. The exclusions were because of articles being a narrative review (n = 1) or about a surgical technique (n = 35). All 95 eligible studies were included in the quantitative analysis. Overall, 17 studies were level 3 comparative cohort studies, and 78 were level 4 case series. The PRISMA flowchart is displayed in Figure 1.
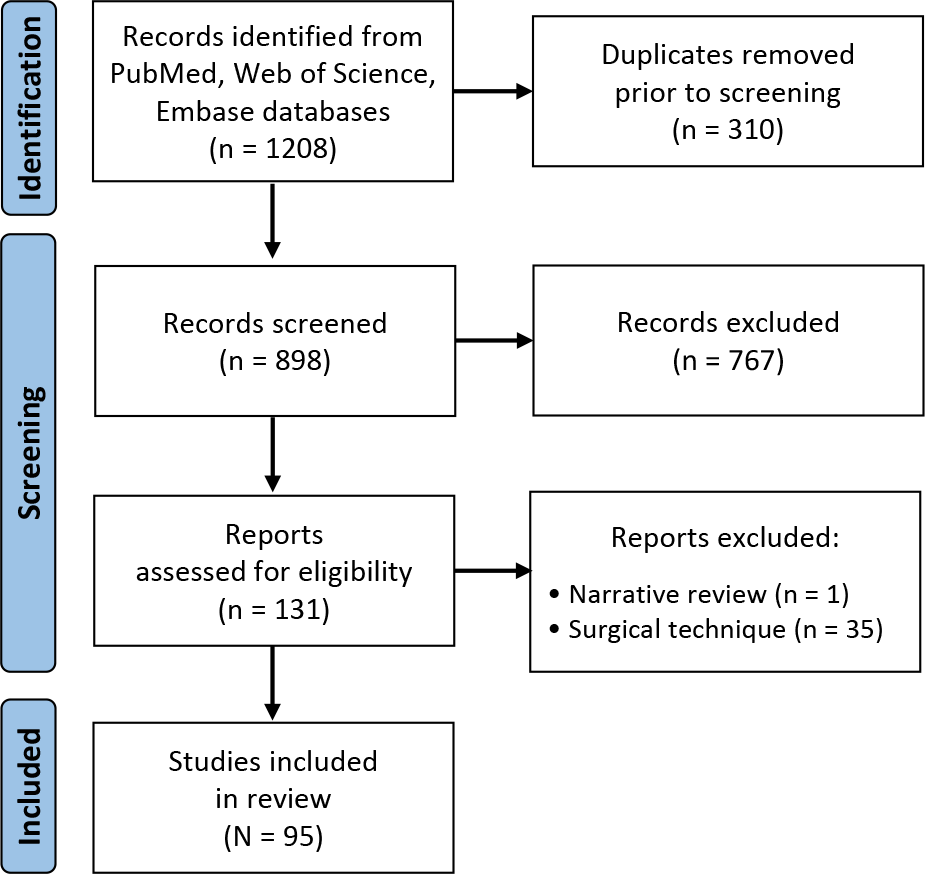
Search strategy flowchart.
Study Characteristics
A summary of the included studies is provided in Appendix Table A1. A total of 14,289 elbow arthroscopic procedures were included in this review. In 78 studies, elbow arthroscopic surgery was performed in an adult population, with mean ages ranging from 21.6 to 80 years. Pediatric populations were reported in 14 studies, with mean ages ranging from 4 to 16 years. One study involved patients <20 years and >60 years, and 1 study did not report patient age. Of the studies that reported patient position, the most common patient position was lateral in 65.1% (2959/4547 procedures), followed by prone in 20.8% (945/4547 procedures) and supine in 15.6% (719/4623 procedures). The mean follow-up was variable across studies, ranging from 1 month to up to 13 years. The main diagnoses for elbow arthroscopic surgery were osteochondritis dissecans, primary osteoarthritis, posttraumatic stiffness/arthritis, and loose bodies.
Complications
The total weighted complication rate was 11.0% (95% CI, 8.8%-13.5%; 1136/14,289 procedures). The overall nerve injury rate was reported with a weighted proportion of 3.4% (95% CI, 2.6%-4.3%; 267/13,725 procedures). An ulnar nerve injury was the most common nerve injury with a weighted proportion of 2.6% (95% CI, 1.9%-3.4%; 123/6290 procedures). The second most injured nerve was the LABCN with a weighted proportion of 1.0% (95% CI, 0.6%-1.4%; 12/5178 procedures). The radial nerve was the third most injured nerve with a weighted proportion of 0.9% (95% CI, 0.6%-1.1%; 34/5666 procedures). Injuries to the posterior interosseous nerve had a weighted proportion of 0.6% (95% CI, 0.4%-0.8%; 8/4662 procedures). Both median nerve and medial antebrachial cutaneous nerve injuries had a similar weighted proportion of 0.5% (95% CI, 0.3%-0.7%; 8/5666 procedures). A nonspecific nerve injury was reported with a weighted proportion of 1.0% (95% CI, 0.7%-1.3%; 95/13,490 procedures).
In terms of soft tissue complications, a superficial wound infection was most commonly reported with a weighted proportion of 2.0% (95% CI, 1.5%-2.6%; 109/5805 procedures), whereas a deep wound infection had a weighted proportion of 0.7% (95% CI, 0.5%-0.9%; 21/5729 procedures). Wound-healing complications such as drainage or dehiscence were reported with a weighted proportion of 1.5% (95% CI, 1.0%-2.2%; 47/5718 procedures).
Regarding complications affecting elbow motion, elbow stiffness had a weighted proportion of 4.5% (95% CI, 2.1%-7.6%; 158/8818 procedures), whereas elbow instability had a weighted proportion of 2.6% (95% CI, 1.4%-4.3%; 6/442 procedures). The need for a subsequent surgical procedure after elbow arthroscopic surgery was reported with a weighted proportion of 4.1% (95% CI, 2.9%-5.6%; 177/8853 procedures).
Discussion
The major finding in this meta-analysis of 95 studies with a total of 14,289 elbow arthroscopic procedures was the total complication rate of 11.0%, with the most common complication being elbow stiffness (4.5% [95% CI, 2.1%-7.6%]) and the need for subsequent surgery with a weighted proportion of 4.1% (95% CI, 2.9%-5.6%; 177/8853 procedures), followed by nerve injuries (3.4% [95% CI, 2.6%-4.3%]). An ulnar nerve injury was the most common nerve injury (2.6% [95% CI, 1.9%-3.4%]), followed by an LABCN injury (1.0% [95% CI, 0.6%-1.4%]). To the best of our knowledge, this is the first meta-analysis that focused on pooling complication rates of elbow arthroscopic surgery, and no other analysis had 95 studies. The total complication rate reported in our meta-analysis seems to be similar to prior large case series that focused on complications after elbow arthroscopic surgery. 28,36,63 In a recent case series on 560 elbow arthroscopic procedures by Intravia et al 28 between 2006 and 2014, the overall complication rate was 9%, with a nerve injury being the most common complication with a rate of 3.5%. However, elbow stiffness was not reported because of the short follow-up period. In another series between 1999 and 2012, Nelson et al 63 reported a higher total complication rate of 14% in a case series of 417 procedures, with the most common complications being superficial and deep infections. In an earlier retrospective case series of 473 elbow arthroscopic procedures between 1980 and 1998, Kelly et al 36 reported a total complication rate of 11.7%, with a transient nerve injury being the most encountered complication with a rate of 2.5%.
Elbow stiffness after elbow arthroscopic surgery was the most common finding in this meta-analysis, with a weighted rate of 4.5%. Kelly et al 36 reported a postoperative stiffness rate of 1.5% with a follow-up period of ≥6 weeks in 87.5% of patients. Moreover, the authors attributed the loss of elbow motion to conditions that predispose to stiffness such as inflammatory arthritis, osteoarthritis, osteochondral defects, and osteochondritis dissecans. Nelson et al 63 reported a rate of 2.6% for postoperative elbow stiffness in 417 elbow arthroscopic procedures with a follow-up period of ≤6 weeks. The authors reported stiffness as heterotopic ossification requiring surgical excision and loss of elbow motion requiring manipulation under anesthesia. In a study using the PearlDiver patient record database, Leong et al 50 reported a reoperation rate of 0.63% within 90 days for stiffness among 4127 patients with 6268 elbow arthroscopic procedures. While conducting this meta-analysis, the rate of elbow stiffness was significantly variable in the literature. This is mainly attributed to the short-term follow-up, varying definitions of stiffness, and mixed patient populations such as different diagnoses and procedures.
Given the superficial position and proximity of neurovascular structures about the elbow joint, elbow arthroscopic surgery remains notorious for nerve injuries. This meta-analysis demonstrated that a nerve injury was the third most common complication in elbow arthroscopic surgery, with a weighted proportion of 3.4%. Moreover, an ulnar nerve injury was the most frequently reported of all nerve injuries, with a weighted proportion of 2.6%. Nerve injury rates after elbow arthroscopic surgery have been quite variable in the literature, with a rate ranging between 0% and 14%. In a retrospective review of 560 elbow arthroscopic procedures, Intravia et al 28 found that the nerve injury rate was 3.5%, which was significantly higher in female patients and patients with prior elbow surgery. In a case series on 200 elbow arthroscopic procedures by Elfeddali et al, 22 a history of trauma and prior elbow surgery were predictors of an increased risk of nerve complications. In another study by Kelly et al 36 on 473 elbows, the rate of nerve injuries was 2.5%, with all being transient. Furthermore, the risk of nerve injuries was significantly associated with the diagnosis of rheumatoid arthritis and contracture. In contrast, other studies have found no association of diagnosis or prior surgery with nerve injuries. In a case series of 227 patients with a nerve injury rate of 6.6%, Jinnah et al 31 did not find a significant association between nerve injuries and having prior elbow trauma or surgery. Nelson et al 63 reported a relatively lower nerve injury rate of 1.7% in 417 elbow arthroscopic procedures, with all nerve injuries being transient. Moreover, the authors did not report significant differences between increasing surgery complexity and the rate of nerve injuries.
An infection is a serious complication after elbow arthroscopic surgery. In a study on 2704 patients with Medicare, Camp et al 13 reported a postoperative infection rate of 1.55%. In addition, several variables were identified as independent risk factors for infections such as age ≥65 years, body mass index >40, smoking, alcohol intake, diabetes mellitus, inflammatory arthritis, hypercoagulable disorders, and intra-articular corticosteroid injections at the time of surgery. Nelson et al 63 reported following 417 elbow arthroscopic procedures, with infection rates of 6.7% and 2.2% for superficial and deep infections, respectively. The higher infection rates were attributed to the frequent use of intra-articular corticosteroids at the time of surgery (P < .0001). In contrast, Intravia et al 28 did report a significant association between intra-articular corticosteroid use and infection rates; however, infection rates were significantly higher by 4-fold in patients with elevated blood sugar at the time of surgery.
Limitations
This study had several limitations that should be acknowledged. Most studies included in this meta-analysis were level 4 case series, with a minority being level 3 cohort studies; thus, the level of evidence in this meta-analysis was low. Although 2 authors independently performed the search, some studies could have been missed, leading to potential selection bias. Because of the complexity of elbow conditions, we found that studies’ demographics would be categorized by diagnoses (single diagnosis or a combination), case complexity codes, or procedure type. This led to significant limitations that prevented us from performing a metaregression and identifying risk factors that would predict specific complications such as diagnosis, case complexity, and procedure type. In addition, the definition of a complication was not uniform across studies, including specifying the severity and duration of certain complications. This could have led to the underestimation or overestimation of certain complication rates.
Conclusion
This study highlights that elbow arthroscopic surgery is a relatively safe procedure with low complication rates. This meta-analysis provides an overview of complication rates after elbow arthroscopic surgery, thus aiding surgeons in counseling patients. It should be emphasized to patients that the most common complications of elbow arthroscopic surgery are stiffness, the need for subsequent surgery and nerve injuries, especially ulnar nerve neuropathy. It is important to understand the anatomy of the elbow in 3 dimensions, learn the appropriate techniques, and comprehend the pathology before attempting elbow arthroscopic surgery. In addition, surgeons should be knowledgeable of the necessary measures to decrease nerve injuries such as joint distension and portal position. Experienced arthroscopic skills are necessary to prevent minor and major complications as the numbers of elbow arthroscopic procedures increase.
Footnotes
Final revision submitted August 8, 2022; accepted August 30, 2022.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
This article does not contain any studies with human participants performed by any of the authors.
APPENDIX
Characteristics of Included Studies a

| Lead Author (Year) | Country | LOE | No. of Patients | Age, y | Surgical Position, n | Follow-up, mo | ||
|---|---|---|---|---|---|---|---|---|
| Prone | Lateral | Supine | ||||||
| Schreiner 80 (2020) | Germany | 4 | 44 | 40.8 | 44 | 0 | 0 | 37.2 |
| Kwak 46 (2020) | Republic of Korea | 4 | 65 | 52 | 0 | 65 | 0 | 32.9 |
| Intravia 28 (2020) | USA | 4 | 556 | 38.6 | 367 | 178 | 11 | 12 |
| Matsuura 55 (2020) | Japan | 4 | 23 | 14.7 | 0 | 0 | 23 | 138 |
| Bachman 6 (2020) | USA | 3 | 41 | 32 | 0 | 41 | 0 | 16 |
| Temporin 86 (2020) | Japan | 4 | 10 | 51.9 | 10 | 0 | 0 | 24 |
| Yang 97 (2020) | China | 4 | 101 | 38.6 | 0 | 101 | 0 | 21 |
| Kwak 47 (2019) | Republic of Korea | 3 | 13 | 39 | 0 | 13 | 0 | 26.5 |
| Pederzini 69 (2019) | Italy | 4 | 9 | 22.4 | 0 | 9 | 0 | 48 |
| Rai 73 (2019) | China | 4 | 143 | 33 | 0 | 0 | 143 | 44 |
| Kwak 45 (2019) | Republic of Korea | 3 | 52 | 52.4 | 0 | 52 | 0 | 35.4 |
| Carlier 14 (2019) | France | 3 | 87 | 49.8 | NR | 6 | ||
| Karelson 34 (2019) | Finland | 4 | 63 | 44.6 | NR | 72 | ||
| Jhan 30 (2018) | Taiwan | 4 | 15 | 27 | 0 | 15 | 0 | 31.2 |
| Andelman 3 (2018) | USA | 4 | 29 | 12.7 | 0 | 0 | 29 | 15.8 |
| Zhu 99 (2018) | China | 4 | 11 | 41.7 | NR | 65 | ||
| Nowotny 66 (2018) | Germany | 4 | 27 | 14 | 0 | 27 | 0 | 45.6 |
| Lubiatowski 52 (2018) | Poland | 4 | 54 | 37 | 0 | 0 | 54 | 24 |
| Kim 38 (2018) | Republic of Korea | 3 | 34 | 49 | 34 | 0 | 0 | 24 |
| Jinnah 31 (2018) | USA | 4 | 227 | 39 | 0 | 227 | 0 | 1 |
| Noticewala 65 (2018) | USA | 4 | 530 | 45.6 | NR | NR | ||
| Mardani-Kivi 54 (2018) | Iran | 4 | 18 | 36.1 | 0 | 18 | 0 | 12 |
| Koh 42 (2018) | USA | 4 | 36 | 32 | 36 | 0 | 0 | 51 |
| Willinger 94 (2018) | Germany | 4 | 42 | 41 | 0 | 42 | 0 | 28.3 |
| Matsuura 56 (2017) | Japan | 4 | 15 | 15.7 | 0 | 15 | 0 | 26.7 |
| Andelman 2 (2017) | USA | 4 | 64 | 11.8 | 0 | 0 | 64 | 10.3 |
| Kim 40 (2017) | Republic of Korea | 4 | 43 | 37.6-42.5 | 0 | 43 | 0 | 55.4-62.2 |
| Arrigoni 4 (2017) | Italy | 3 | 35 | 47.1 | 0 | 35 | 0 | 24 |
| Chen 16 (2017) | China | 3 | 32 | 34.3 | 0 | 0 | 32 | 17.1 |
| Kwon 48 (2017) | Republic of Korea | 3 | 30 | 49.3 | 0 | 30 | 0 | 31 |
| Werner 92 (2016) | USA | 3 | 1265 | <65 y: 48.5%; 65-80 y: 47.8%-48.2%; >80 y: 3.3%-3.8% | NR | 3 | ||
| Vavken 90 (2016) | Switzerland | 4 | 50 | 13.6 | 0 | 0 | 50 | 12 |
| Soeur 82 (2016) | France | 4 | 35 | 48 | 0 | 35 | 0 | 48 |
| van Rheenen 89 (2015) | Netherlands | 4 | 1004 | NR | NR | 12 | ||
| Dilokhuttakam 20 (2015) | Thailand | 4 | 49 | 42 | 0 | 49 | 0 | 1.5 |
| Leong 50 (2015) | USA | 4 | 6268 | <20 y: 25%; 20-39 y: 25%; 40-59 y: 47%; ≥60 y: 6% | NR | NR | ||
| Wu 95 (2015) | China | 4 | 34 | 39.6 | 0 | 0 | 34 | 12 |
| Yoon 98 (2015) | Republic of Korea | 4 | 45 | 45.9 | 45 | 0 | 0 | 26.9 |
| Rajeev 74 (2015) | UK | 4 | 121 | 38 | NR | 12 | ||
| Merolla 57 (2015) | Italy | 3 | 48 | 48.1 | 0 | 48 | 0 | 44 |
| Temporin 85 (2015) | Japan | 4 | 9 | 6.6 | 0 | 9 | 0 | 14.7 |
| Ertem 23 (2015) | Turkey | 4 | 28 | 46 | 28 | 0 | 0 | 20.5 |
| Uchida 88 (2015) | Japan | 4 | 18 | 14.2 | 0 | 0 | 18 | 36 |
| Oki 68 (2014) | Japan | 4 | 23 | 49 | 0 | 23 | 0 | 24 |
| Moon 62 (2014) | Republic of Korea | 4 | 11 | 45 | 0 | 11 | 0 | 30 |
| Pederzini 70 (2014) | Italy | 4 | 212 | 41-43 | 212 | 0 | 0 | 58 |
| Nelson 63 (2014) | USA | 4 | 417 | 43.4 | 0 | 417 | 0 | 0.5-1.5 |
| Miyake 60 (2014) | Japan | 4 | 20 | 38 | 20 | 0 | 0 | 25 |
| Lim 51 (2014) | Republic of Korea | 4 | 43 | 51.4 | 0 | 43 | 0 | 38 |
| Babaqi 5 (2014) | Egypt | 4 | 33 | 33.7 | 0 | 33 | 0 | 14.4 |
| Kniesel 41 (2014) | Germany | 3 | 25 | 46 | 25 | 0 | 0 | 24 |
| Blonna 11 (2014) | USA | 3 | 235 | 41 | 0 | 235 | 0 | NR |
| Rhyou 76 (2013) | Republic of Korea | 3 | 39 | 46-47 | NS (either prone or lateral) | 46 | ||
| Elfeddali 22 (2013) | UK | 4 | 200 | 37 | 0 | 200 | 0 | 2 |
| MacLean 53 (2013) | UK | 4 | 21 | 42 | 0 | 21 | 0 | 65.9 |
| Wijeratna 93 (2012) | UK | 4 | 15 | 49.6 | 0 | 15 | 0 | 20 |
| Dzugan 21 (2012) | USA | 4 | 7 | 40.7 | 7 | 0 | 0 | 12-24 |
| Wulf 96 (2012) | USA | 4 | 10 | 13.9 | 10 | 0 | 0 | 42 |
| Kovachevich 43 (2012) | USA | 4 | 15 | 51 | 0 | 15 | 0 | 12 |
| Cefo 15 (2011) | Netherlands | 4 | 27 | 42 | 0 | 27 | 0 | 24 |
| Blonna 12 (2010) | USA | 4 | 26 | 38 | NR | 33 | ||
| Schoch 79 (2010) | USA | 4 | 13 | 16 | NS (either prone or supine) | 43.2 | ||
| Kang 33 (2010) | Republic of Korea | 4 | 26 | 45.5 | 0 | 26 | 0 | 33.9 |
| Rahusen 72 (2009) | Netherlands | 4 | 16 | 29 | 0 | 16 | 0 | 38 |
| Grewal 24 (2009) | Canada | 4 | 36 | 45.3 | 0 | 36 | 0 | 42 |
| Hausman 25 (2008) | USA | 4 | 4 | 42.8 | 0 | 0 | 4 | 12 |
| Adams 1 (2008) | USA | 4 | 42 | 52.8 | 0 | 42 | 0 | 24 |
| Michels 59 (2007) | Belgium | 4 | 14 | 37.5 | 14 | 0 | 0 | 67.2 |
| Krishnan 44 (2007) | USA | 4 | 11 | 36 | 11 | 0 | 0 | 26 |
| Kelly 35 (2007) | USA | 4 | 25 | 51 | 0 | 25 | 0 | 33.8 |
| Hausman 26 (2007) | USA | 4 | 6 | 4 | 0 | 0 | 6 | 52 |
| Schubert 81 (2007) | Belgium | 4 | 24 | 38.4 | 0 | 24 | 0 | 24 |
| Cummins 19 (2006) | USA | 4 | 18 | 43.2 | 0 | 18 | 0 | 21.6 |
| Nguyen 64 (2006) | Canada | 4 | 22 | 42 | 0 | 22 | 0 | 25 |
| Spahn 83 (2006) | Germany | 3 | 21 | 34 | 21 | 0 | 0 | 30 |
| Tanaka 84 (2006) | Japan | 3 | 11 | 51 | 0 | 11 | 0 | 156 |
| Kim 37 (2006) | USA | 4 | 12 | 21.6 | 0 | 0 | 12 | 33.8 |
| Ball 7 (2002) | USA | 4 | 14 | 36.9 | 0 | 14 | 0 | 12-29 |
| Horiuchi 27 (2002) | Japan | 4 | 29 | 51.2 | 0 | 29 | 0 | 97 |
| Micheli 58 (2001) | USA | 4 | 49 | 14 | 0 | 0 | 49 | 56.4 |
| Clasper 17 (2001) | UK | 4 | 57 | 41.4 | 0 | 57 | 0 | 27 |
| Kelly 36 (2001) | USA | 4 | 473 | 36 | 0 | 473 | 0 | 42 |
| Cohen 18 (2000) | USA | 3 | 26 | 46 | NR | 35.3 | ||
| Reddy 75 (2000) | USA | 3 | 181 | 30 | 13 | 74 | 94 | 42.3 |
| Savoie 78 (2009) | USA | 4 | 24 | 59 | 24 | 0 | 0 | 32 |
| Ruch 77 (1998) | USA | 4 | 12 | 14.5 | 12 | 0 | 0 | 48 |
| Baumgarten 9 (1998) | USA | 4 | 17 | 13.8 | 0 | 0 | 17 | 32.4 |
| Jerosch 29 (1998) | Germany | 4 | 103 | 29 | NR | 74.4 | ||
| Phillips 71 (1998) | USA | 4 | 25 | 31.6 | 0 | 0 | 25 | 18 |
| Lee 49 (1997) | USA | 4 | 14 | <65 | NR | 42 | ||
| Kim 39 (1995) | Republic of Korea | 4 | 26 | 34 | NS (either prone or supine) | 25 | ||
| Timmerman 87 (1994) | USA | 4 | 19 | 36 | 0 | 0 | 19 | 29 |
| Ward 91 (1993) | USA | 4 | 35 | 29 | 0 | 0 | 35 | 24 |
| Jones 32 (1993) | USA | 4 | 12 | 38 | 12 | 0 | 0 | 21.8 |
| O’Driscoll 67 (1992) | USA | 4 | 70 | 34 | Initial cases were supine; later in the study, a lateral position was used | 34 | ||
a Data are reported as means or ranges. LOE, level of evidence; NR, not reported; NS, not specified.