
Abstract
Background:
Whether lateral hinge fracture (LHF) after open-wedge high tibial osteotomy (OWHTO) is associated with the change in tibial posterior slope (PS) has not been determined. Risk factors for PS increase are still unknown.
Hypothesis:
There will be no difference in patient characteristics and radiographic factors when stratified by change in tibial PS (ΔPS).
Study Design:
Cohort study; Level of evidence, 3.
Methods:
We reviewed the records of 148 patients who underwent OWHTO with locking-plate fixation from 2010 to 2016. Included were those with a minimum 2-year follow-up and true lateral radiographs before and at 1 year after surgery. ΔPS was defined as a difference between preoperative and 1-year postoperative PS, with positive values indicating PS increase. ΔPS was classified into <3°, 3° to <6°, and ≥6°. Any LHFs were grouped by Takeuchi classification as stable (type 1) or unstable (types 2 and 3). Risk factors for PS increase were evaluated using ordinal logistic regression analyses. Clinical outcomes according to ΔPS were evaluated using the Hospital for Special Surgery score.
Results:
There were 79 (53.4%) patients with ΔPS <3°, 44 (29.7%) with 3° ≤ ΔPS < 6°, and 25 (16.9%) with ΔPS ≥6°. LHFs were observed in 41 (27.7%) patients: 32 with type 1 and 7 and 2 with types 2 and 3, respectively. Results of the multivariate ordinal logistic regression analysis indicated that ΔPS was associated with unstable LHF (P = .005, exp[β] = 6.34), preoperative PS (P = .028, exp[β] = 0.90), and correction angle (P = .037, exp[β] = 1.09). ΔPS ≥6° was seen in 4 of 9 (44.4%) patients with unstable LHF, 9 of 32 (28.1%) with stable LHF, and 12 of 107 (11.2%) with no LHF (P = .017). The mean correction angle was 11.3° ± 3.6° in patients with ΔPS ≥6°, 9.4° ± 4.6° in cases of 3° ≤ ΔPS < 6°, and 8.8° ± 3.6° in cases of ΔPS <3° (P = .019). Hospital for Special Surgery scores did not differ according to ΔPS.
Conclusion:
LHF type and correction angle were associated with ΔPS after OWHTO, and unstable LHF and large correction angle were risk factors for PS increase. There was no significant difference in clinical outcomes according to ΔPS.
High tibial osteotomy is a reliable treatment option for medial compartment osteoarthritis with varus deformity of the knee joint. 10,11,37 Despite its reproducibility of correction on the coronal plane, medial open-wedge high tibial osteotomy (OWHTO) is often accompanied with an unexpected change on the sagittal plane, such as posterior slope (PS) increase of the tibia. 5,21,25 Several studies have attributed PS increase to the obliquity of the anteromedial tibial cortex. 9,30,34 Accordingly, several technical recommendations have been made to avoid PS increase, mostly regarding the ratio of the anterior osteotomy gap to the posterior. 4,27,31 However, PS increase is still a notable problem in OWHTO.
Because PS increase is simply considered a surgical error that can be prevented by paying attention to the osteotomy gap, risk factors for PS increase have never been identified. Lateral hinge fracture (LHF) is an unexpected complication, with the incidence being higher than previously thought. 12,15,16 Its adverse effects have mostly been investigated in terms of the coronal plane, such as correction accuracy and correction loss. Although stable LHF (type 1 according to Takeuchi classification 33 ) is considered benign and of little clinical importance, a recent study found that a stable LHF could alter the PS. 18 This has raised questions regarding the adverse effect of unstable LHFs (type 2 or 3) and other risk factors for PS increase.
PS increase has biomechanical disadvantages. A cadaveric study proved that PS increase causes an anterior shift in the tibial resting position that is accentuated under axial loads. 8 It is also associated with the increase of anterior cruciate ligament (ACL) strain 6 and the incidence of medial meniscus posterior root tear 28 and other types of medial meniscus posterior horn tear. 24
In this study, we aimed to identify risk factors for PS increase, with a focus on the effect of LHF. It was hypothesized that there would be no difference in demographic and radiographic factors according to the change in PS (ΔPS).
Methods
The study was approved by our institutional review board. Patients who underwent OWHTO with locking plate fixation from 2010 to 2016 were retrospectively reviewed. The indications for OWHTO were physically active patients who complained of walking pain in the medial compartment of the joint, despite nonsurgical treatments for 3 months. Simple radiography and magnetic resonance imaging were performed preoperatively to confirm that osteoarthritis of the medial compartment was Ahlbäck grade <3 and had not advanced to the lateral compartment. The severity of varus deformity was always evaluated on long-standing hip-to-ankle radiographs. OWHTO was contraindicated in cases with Ahlbäck grade ≥3 medial compartment arthritis, active inflammatory arthritis, lateral compartmental arthritis, severe patellofemoral arthritis, and a flexion contracture >10°.
The following inclusion criteria were applied in this study: primary medial OWHTO using locking plate fixation, a follow-up duration ≥2 years, and true lateral radiographs before and 1 year after surgery to evaluate the ΔPS. Of the 158 consecutive cases, 2 revision OWHTOs, 2 double-level osteotomies, and 6 with insufficient follow-up duration were excluded, leaving 148 patients with a mean ± SD follow-up of 49.7 ± 21.8 months (range, 24-102 months) included in the study (Figure 1).

Flowchart outlining the patient selection process. OWHTO, open-wedge high tibial osteotomy.
Surgical Technique and Rehabilitation
The target correction angle was measured on a long-standing hip-to-ankle radiograph with the patella facing forward, using the method described by Miniaci et al. 23 The target weightbearing point was adjusted from 62.5% from the medial border along the width of the tibial plateau, based on arthroscopic findings regarding the severity of degenerative changes in each compartment of the knee joint. 7
After partial detachment of the semitendinosus and gracilis tendons, the superficial medial collateral ligament was distally released below the osteotomy level. Biplanar osteotomy was performed until 9 mm of the intact lateral hinge remained. The proximal tibia was opened using a laminar spreader under intraoperative fluoroscopy and fixed with TomoFix plate (DePuy Synthes). A distal cortical screw was inserted in full extension of the knee joint. Weightbearing was gradually allowed from toe-touch during the first 2 weeks to full weightbearing at 6 to 8 weeks postoperatively.
Evaluation of the Tibial PS and LHF
The tibial PS was measured on true lateral radiographs that were obtained before and 1 year after surgery. Based on a previously validated method, 35 PS was measured between the medial tibial plateau and a line parallel to the middiaphysis of the tibia. ΔPS was defined as a difference between preoperative and 1-year postoperative values, with positive ΔPS indicating PS increase. Patients were classified into 3 groups: ΔPS <3°, 3° ≤ ΔPS < 6°, and ΔPS ≥6°.
LHF was determined if lateral cortical breakage was detected on any of the following: intraoperative fluoroscopy images, serial postoperative radiographs, and computed tomography scans routinely obtained within a week of surgery. LHFs were categorized with the Takeuchi classification 33 : type 1, LHFs within or just above the proximal tibiofibular joint; type 2, those involving the distal portion of the proximal tibiofibular joint; and type 3, those with intra-articular extension to the lateral tibial plateau. Patients were grouped as having a stable LHF (type 1), unstable LHF (types 2 and 3), or no LHF.
The ΔPS and LHF types were independently assessed by 2 orthopaedic surgeons (J.-H.S. and S.-I.B.), and interrater reliability was determined using Cohen kappa (κ), where values were interpreted as poor (<0.20), fair (0.21-0.40), moderate (0.41-0.60), good (0.61-0.80), and very good (>0.80). 1
Statistical Analysis
To investigate risk factors for PS increase, ΔPS was analyzed using ordinal logistic regression analyses. Univariate regression analyses were conducted first, with each demographic and radiographic factor: age, sex, body mass index, preoperative PS, preoperative hip-knee-ankle angle, lateral distal femoral angle, medial proximal tibial angle, correction angle, and LHF type. Based on the results, potential risk factors were selected and included in a multivariate regression analysis. Each risk factor was analyzed according to ΔPS using a chi-square test or analysis of variance. Clinical outcomes according to ΔPS were evaluated using the Hospital for Special Surgery (HSS) score. SPSS Statistics (Version 19.0; IBM) was used for all statistical analyses.
Results
The interrater reliabilities of ΔPS and LHF type were 0.88 and 0.90, respectively, indicating very good agreement levels between the observers. Of the 148 study patients, 79 (53.4%), 44 (29.7%), and 25 (16.9%) were classified as ΔPS <3°, 3° ≤ ΔPS < 6°, and ΔPS ≥6°, respectively. The demographic and radiographic characteristics of the patients are summarized in Table 1.
Demographic and Radiographic Characteristics Overall and According to ΔPS Group a

a Data are reported as mean ± SD unless otherwise indicated. Bold P values indicate statistically significant difference between study groups (P < .05). HKA, hip-knee-ankle angle; LDFA, lateral distal femoral angle; MPTA, medial proximal tibial angle; PS, posterior slope.
b Positive values indicate varus alignment and negative values indicate valgus alignment.
LHFs were observed in 41 (27.7%) patients: 32 had stable LHF (type 1) (Figure 2) and 7 and 2 patients had unstable LHF (type 2 and 3, respectively) (Figures 3 and 4). The mean final HSS scores were 90.6 ± 8.8 in cases of ΔPS ≥6°, 91.1 ± 6.3 in cases of 3° ≤ ΔPS < 6°, and 89.6 ± 7.4 in cases of ΔPS ≥6°, showing no significant difference (P = .805).
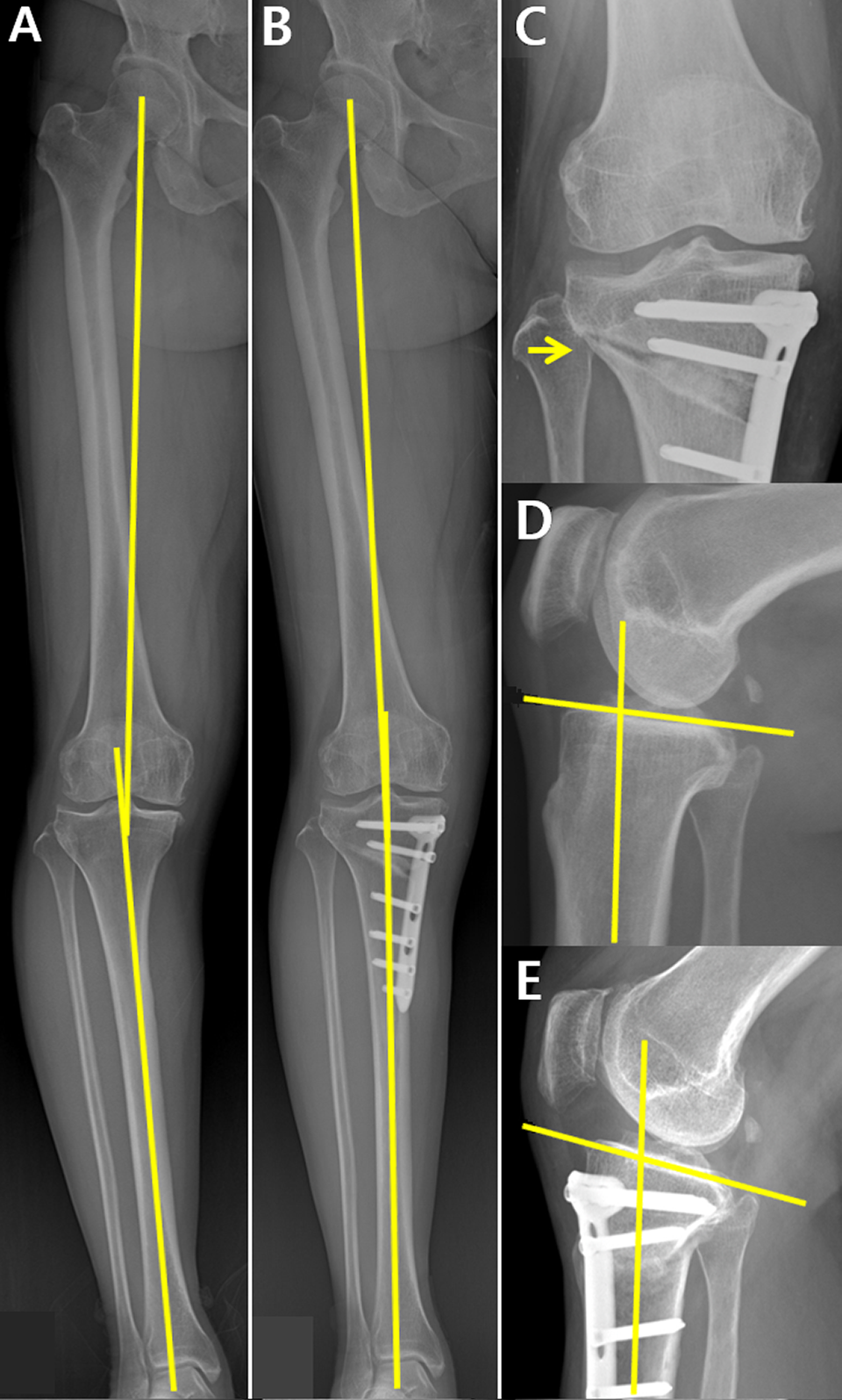
PS increase in the right leg of a patient with type 1 LHF (stable) after open-wedge high tibial osteotomy, with a correction angle of 11°. (A) Preoperative 8° varus alignment was corrected to (B) postoperative 3° valgus alignment. (C) Type 1 LHF (arrow) was noted on a postoperative radiograph. The PS increased from (D) 3° preoperatively to (E) 10° postoperatively. LHF, lateral hinge fracture; PS, posterior slope.

PS increase in the left leg of a patient with type 2 LHF (unstable) after open-wedge high tibial osteotomy, with a correction angle of 8°. (A) Preoperative 7° varus alignment was corrected to (B) postoperative 1° valgus alignment. (C) Type 2 LHF (arrow) was noted on a postoperative radiograph. The PS increased from (D) 14° preoperatively to (E) 16° postoperatively. LHF, lateral hinge fracture; PS, posterior slope.

PS increase in the left leg of a patient with type 3 LHF (unstable) after open-wedge high tibial osteotomy, with a correction angle of 15°. (A) Preoperative 7° varus alignment was corrected to (B) postoperative 8° valgus alignment. (C) Type 3 LHF (arrow) was noted on a postoperative radiograph. The PS was increased from (D) 15° preoperatively to (E) 21° postoperatively. LHF, lateral hinge fracture; PS, posterior slope.
Risk Factors for PS Increase
A multivariate regression analysis was performed with related factors that were confirmed by univariate regression analyses (Table 2). It found that unstable LHF (P = .005, exp[β] = 6.34), preoperative PS (P = .028, exp[β] = 0.90), and correction angle (P = .037, exp[β] = 1.09) were associated with ΔPS. Preoperative PS had a negative correlation with ΔPS. Four of 9 patients (44.4%) with unstable LHF, 9 of 32 (28.1%) with stable LHF, and 12 of 107 (11.2%) with no LHF showed ΔPS ≥6° (P = .017, chi-square test) (Table 3). The mean correction angle was 11.3° ± 3.6° in cases of ΔPS ≥6°, 9.4° ± 4.6° in cases of 3°≤ ΔPS <6°, and 8.8° ± 3.6° in cases of ΔPS <3° (P = .019, analysis of variance).
Results of Ordinal Logistic Regression Analysis Regarding PS Increase a
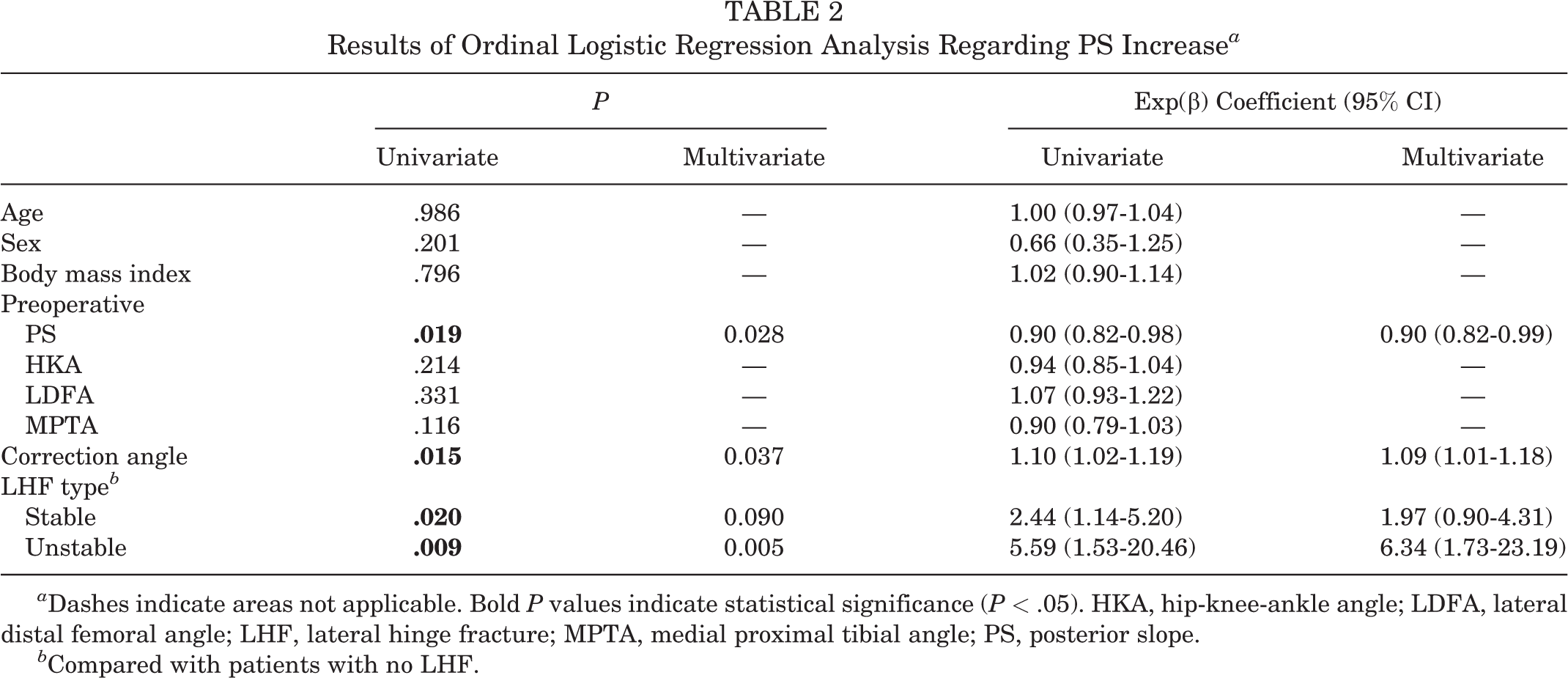
a Dashes indicate areas not applicable. Bold P values indicate statistical significance (P < .05). HKA, hip-knee-ankle angle; LDFA, lateral distal femoral angle; LHF, lateral hinge fracture; MPTA, medial proximal tibial angle; PS, posterior slope.
b Compared with patients with no LHF.
LHF According to ΔPS Group a

a LHF, lateral hinge fracture; PS, posterior slope.
b Chi-square test (P < .05).
Discussion
The most important finding of the present study was that unstable LHF and large correction angle were risk factors for PS increase after OWHTO. Stable LHF had a significant association with ΔPS; however, its effect was offset when considered with the correction angle. Preoperative PS was negatively correlated with ΔPS, which meant that it did not have much effect on the consequential PS. Despite the biomechanical and clinical significances of the PS, HSS scores did not significantly differ according to PS increase.
Radiographic outcomes of OWHTO have mostly been evaluated in terms of the coronal plane because the purpose of osteotomy is realignment of the limb on the coronal plane. The sagittal alignment that can be represented as the PS is expected to remain unchanged with the standard surgical technique. 9,27 A systemic review showed a surprisingly low accuracy of OWHTO. 36 Numerous recent studies have identified risk factors for inaccurate correction in an effort to improve the surgical outcome. 12,14,32 However, few studies have investigated risk factors for PS increase. The present study found that a large correction angle was associated with PS increase. This implied a trade-off of the alignment change between the planes. 2 Thus, the coronal and sagittal planes should be considered together in evaluation of the postoperative change in OWHTO. Previous studies have shown that the hinge position 22,25 and the sagittal osteotomy inclination 19,26 affect the postoperative PS. To avoid the change in PS, the sagittal osteotomy inclination should be parallel to PS. Because posterolateral hinge location can cause PS increase, sufficient osteotomy of the posterior cortex should be achieved.
Surgical recommendations regarding the anterior and posterior osteotomy gaps in maintaining the PS are based on the premise that the lateral hinge is intact. 20,27 Lee et al 18 reported that stable type 1 LHF was a risk factor for PS increase. The present study showed that unstable LHF was a risk factor for PS increase; however, stable LHF had a significant association with ΔPS only in a univariate analysis. Previous studies have found that a large osteotomy gap is associated with LHF. 16,17 Because of the correlation between the osteotomy gap (correction amount) and stable LHF, the adverse effect of a stable LHF on PS increase was not evaluated in this study. Recent studies have reported that LHF caused several problems in OWHTO, including inaccurate correction and correction loss. 16,32 The results of the present study add 1 more reason why surgeons should pay extra caution to avoid LHF.
The clinical relevance of PS increase after OWHTO was underestimated because the ACL was expected to resist against the tibial anterior translation. 29 Indeed, this study did not find a significant difference in HSS scores according to ΔPS. However, the adverse effects of such biomechanical changes are accumulated on the ACL and the medial meniscus posterior horn, which could cause resultant ACL degeneration 3,13 or medial meniscus posterior horn tear. 24,28 The effects of PS increase need to be evaluated in the long term.
Limitations
Some limitations should be noted. First, there may be selection bias attributed to the retrospective nature of this study. Second, already known factors that can affect the postoperative PS were not investigated, such as the hinge position 22,25 and the sagittal osteotomy inclination. 19,26 These factors would reflect the change in PS more directly. Third, there were not enough cases of type 3 LHF, so we had to put type 2 and 3 LHFs together into a single unstable LHF category. This category is based on the original report of Takeuchi et al, 33 which stated that type 2 and 3 LHFs were different from type 1 LHF in terms of stability. Fourth, the clinical disadvantages caused by PS increase could not be demonstrated. A longer-term study is expected to prove that.
Conclusion
LHF type and correction angle were associated with ΔPS after OWHTO. Unstable LHF and large correction angle were risk factors for PS increase. There were no significant differences in clinical outcomes according to ΔPS.
Footnotes
Final revision submitted July 25, 2022; accepted August 30, 2022.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Asan Medical Center (No. 2020-0942).