
Abstract
Background:
Injury to the ulnar collateral ligament (UCL) of the medial elbow has been treated successfully with ligament repair augmented with internal brace. Previous work has shown that this procedure does not overconstrain the ulnohumeral joint; however, the procedures were conducted by a single surgeon, which controlled for anchor placement and graft tensioning.
Purpose/Hypothesis:
Our purpose was to evaluate the reproducibility of contact mechanics and joint torque after UCL repair with internal brace as performed by different surgeons compared with repair by a single surgeon. It was hypothesized that there would be no significant difference in elbow contact mechanics, valgus torque, or torsional stiffness between the 2 groups.
Study Design:
Controlled laboratory study.
Methods:
Nine pairs of fresh-frozen cadaveric elbows were tested biomechanically under 3 conditions: UCL-intact (UCL-I), UCL-deficient (UCL-D), and UCL-repaired with internal brace augmentation (UCLR-IB). For each pair, 1 elbow was repaired by a single surgeon, and the contralateral elbow was repaired by 1 of 9 other surgeons. Testing consisted of valgus torsion between 0° and 5° with the elbow positioned at 90° of flexion. Ulnohumeral contact mechanics and overall joint torque and stiffness were measured and compared between surgeon groups.
Results:
There were no statistically significant differences between the single-surgeon and multiple-surgeon groups regarding contact area (P = .83), contact force (P = .27), peak pressure (P = .26), or peak force (P = .30); however, contact pressure was significantly affected (P = .02) by surgeon group. Compared with UCL-I, both UCL-D and UCLR-IB conditions had a significant overall effect on contact area (P = .004) and contact force (P = .05); however, contact pressure (P = .56), peak pressure (P = .27), and peak force (P = .24) were not affected by injury condition. Measurements of elbow torque (P = .28) and stiffness (P = .98) were not significantly different between surgeon groups.
Conclusion:
UCL repair with internal brace provided consistent results among several surgeons when compared with a single surgeon. The procedure did not lead to joint overconstraint while also returning the ligament to near-intact levels of resisting valgus stress.
Clinical Relevance:
UCL repair with internal brace augmentation is a reproducible surgical technique that has good clinical outcomes in the literature.
The elbow is a complex joint that requires a combination of static bony articulation, dynamic muscular control, and ligamentous restraint to allow for stable range of motion. 5 In the context of throwing athletes, the ulnar collateral ligament (UCL) is essential in controlling valgus stress, specifically through 70° and 120° of elbow flexion. The medial elbow ligamentous complex consists of 3 bundles (anterior, posterior, and oblique), with the anterior bundle providing the primary restraint to valgus stress and the target for UCL reconstruction or repair. 5 Injuries to the UCL have increased in the past decade, along with the number of surgical reconstructions and repairs. 2,6 A recent study by Rothermich et al 18 showed that between 49% and 57% of all Division I National Collegiate Athletic Association baseball programs had at least 1 UCL surgery in 2017, 2018, and 2019.
Traditionally, the gold standard UCL reconstruction with autograft has had excellent outcomes in throwing athletes, with 83% returning to the same level of sport or higher after a minimum of 2 years 3 ; however, there has been a resurgence in the orthopaedic literature regarding UCL repair in the setting of partial injury or end avulsion. Part of this resurgence is probably due to the introduction of the internal brace system as an augment to the UCL repair. Both biomechanical 2,10 and outcome 7,14 studies have shown promising results when appropriate indications have been met. The ideal patient is a throwing athlete who sustained an acute injury and has a ligament injury with good intrasubstance ligament tissue quality. Patients that have acute on chronic injuries with poor ligament quality or intraligament bony ossicles or avulsions should be considered for reconstruction rather than repair. 4,7,12
A recent biomechanical cadaveric study reported that UCL repair with internal brace does not overconstrain the ulnohumeral joint 16 ; however, all repairs were performed by a single surgeon, which helped to control for anchor placement and graft tensioning. Overconstraint was a concern, as the repair or reconstruction of the medial ligamentous complex could increase contact pressures across the joint, thus leading to potential range of motion constraints or accelerated articular wear.
The aims of the current study were to evaluate the reproducibility of consistent contact mechanics and joint torque after UCL repair with internal brace as performed by different surgeons compared with multiple repairs by a single surgeon. It was hypothesized that, by following our reproducible technique, there would be no significant difference in elbow contact mechanics, valgus torque, or torsional stiffness between the multiple- and single-surgeon groups.
Methods
A total of 18 fresh-frozen upper extremity specimens from 9 cadavers were procured for the study (Science Care). Before repair, each specimen was allowed to thaw at room temperature for approximately 24 hours. Specimens were prepared for biomechanical testing as has been done previously. 7 Briefly, the humerus and forearm were transected and soft tissue was excised for purposes of potting the bone in sections of cylindrical acrylic pipe using polymethylmethacrylate. A medial incision was made centered over the medial epicondyle, extending proximally and distally in line with the ulnar nerve. The skin was elevated, and the cubital tunnel was incised to allow for visualization of the UCL. The flexor pronator mass was elevated off of the UCL, and the 2 heads of the flexor carpi ulnaris were split to properly identify the sublime tubercle distally.
Once the UCL was appropriately exposed, the interval between the flexor pronator mass and brachialis was identified and the brachialis was elevated off of the anterior capsule. A 2-cm transverse incision was made just superficial to the ulnohumeral joint, allowing for placement of a K-Scan 6900 pressure sensor (Tekscan). Before potting, the radius and ulna were drilled with a quadricortical screw to maintain full supination. The acrylic pipe was allowed to harden fully before further testing.
The prepared specimens were then loaded into a custom testing fixture that was previously described as appropriate for UCL torque and contact pressure testing. 16 This was mounted into a servohydraulic mechanical test frame (MTS Systems) with torsional capabilities. The elbow joint was distracted minimally in approximately 30° to 45° of flexion to allow for insertion of a single branch of the pressure sensor into the ulnohumeral joint space (Figure 1). The joint was then repositioned to 90° of elbow flexion for the remainder of testing. The intact ligament was tested by internally rotating the humerus on a stationary forearm, creating a valgus force across the medial elbow. For the intact state (UCL-I), 10 cycles of torsion between 0° and 5°, at a rate of 1° per second, were performed as previously described. 16

Pressure sensor positioned within the ulnohumeral joint space of a left elbow.
Once UCL-I testing was complete, a longitudinal split in the UCL was performed, in line with the anterior fibers, to visualize the joint. The distal insertion of the anterior band was then sharply released off of the sublime tubercle, creating a complete distal tear. A distal tear was chosen to replicate the conditions in the study performed by Roth et al. 16 Again, 10 cycles of torsion were performed to evaluate the UCL-deficient (UCL-D) state.
The ligament was then repaired with the internal brace as has been described in previous studies. 7,8,10,12 For each pair, 1 limb was repaired by a single surgeon (J.R.D.) with >20 years of experience; each contralateral limb was repaired by a different surgeon (e.g., S.N.K, M.A.R., E.L.C.). Experience levels in the multiple-surgeon group ranged from postresident fellow to equivalent to that of the single-surgeon group.
The distal insertion of the UCL on the sublime tubercle was identified, approximately 6 to 8 mm distal to the joint, and the 2.7-mm drill bit was used to make the pilot hole, aiming distally and posteriorly to avoid entering the joint. Once drilled, the collagen-coated FiberTape (Arthrex) and No. 0 FiberWire (Arthrex) were loaded into the first 3.5-mm PEEK SwiveLock anchor (Arthrex). The ligament was repaired to its insertion site using the preloaded suture from the SwiveLock anchor with slight varus stress of the elbow in approximately 20° of flexion. Before fully seating the anchor, tension was determined by confirming full range of motion of the elbow as well as ensuring there was no excess slack or gapping of the joint. A small, curved hemostat could be placed between the internal brace and UCL to help prevent overtightening when inserting the second anchor. If there were any concerns at this point for either over- or underconstraint, the anchor could be removed and the FiberTape length could be adjusted to either increase or decrease the amount used in the augmentation.
The longitudinal split was then repaired with the remainder of the No. 0 suture, in an interrupted simple fashion. The humeral anchor site was drilled at the proximal insertion of the UCL, again, at the anterior aspect of the medial epicondyle. The second anchor was then loaded onto the suture tape ends and inserted into the drill hole with the elbow in slight varus. Before fully advancing the anchor into the bone, tension was assessed by confirming full range of motion of the elbow. The internal brace and ligament were then sutured together with interrupted sutures to create a unified repair (UCLR-IB state) (Figure 2). Range of motion and tension were again assessed confirming appropriate repair with augmentation. The final torsion testing was completed to evaluate the repair.

Left elbow with completed ulnar collateral ligament repair with internal brace augmentation.
Potential differences between the single- and multiple-surgeon groups were assessed using 2-way analysis of variance (ANOVA) with repeated measures (JMP 10.0.0, SAS Institute, Inc). Individual comparisons were made using Tukey honest significant difference post hoc analysis. Significance was set at P ≤ .05.
Results
The contact mechanics after 10 cycles of valgus torsion of UCL specimens were not significantly different between surgeon groups with regard to contact area (P = .83), contact force (P = .27), peak pressure (P = .26), or peak force (P = .30); however, contact pressure was affected significantly by surgeon group (P = .02) (Table 1). The act of creating a defect and subsequently repairing that defect with internal brace augmentation was shown to have a significant overall effect on contact area (P = .004) and contact force (P = .05); however, contact pressure (P = .56), peak pressure (P = .27), and peak force (P = .24) were not affected by injury condition.
Results of UCL Valgus Torsion Test for the Intact, Deficient, and Repaired With Internal Brace Conditions According to Single-Surgeon and Multiple-Surgeon Groups a

a Data are presented as mean ± SEM. Boldface P value indicates statistically significant difference between the single- and multiple-surgeon groups (P ≤ .05; 2-way analysis of variance). UCL, ulnar collateral ligament; UCL-I, UCL-intact; UCL-D, UCL-deficient; UCLR-IB, UCL-repaired with internal brace augmentation.
Measurements of elbow torque at the 10th cycle demonstrated that both surgeon groups returned the overall resistance to valgus angular displacement to near-intact levels (Figure 3), with no overall effect of surgeon group (P = .28; 2-way ANOVA) (Table 1). There was, however, a significant overall effect of injury condition (P < .0001). Pairwise comparisons of injury condition for both groups combined showed a significant decrease in torque in the UCL-D state (P < .0001), followed by a significant recovery from the deficient to the UCLR-IB state (P = .004). Importantly, there was no difference in torque resistance between the UCL-I and UCLR-IB conditions (P = .26).
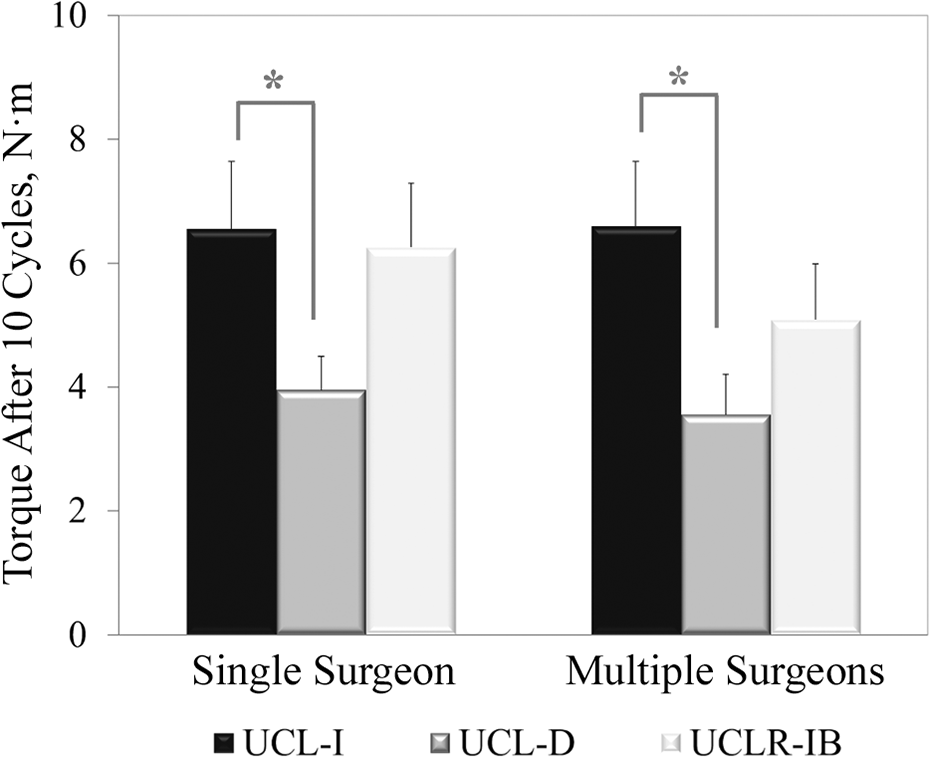
In both the single-surgeon and the multiple-surgeon groups, the mean elbow torque after 10 cycles of valgus torsion was significantly lower in the UCL-D condition when compared with the UCL-I condition. Mean elbow torque in the UCLR-IB condition was not significantly different between surgeon groups. *P < .05. UCL, ulnar collateral ligament; UCL-I, UCL-intact; UCL-D, UCL-deficient; UCLR-IB, UCL-repaired with internal brace augmentation.
Likewise, UCL repair performed by both the single- and multiple-surgeon groups returned torsional stiffness to levels similar to the UCL-I state. Two-way ANOVA revealed a significant overall effect of injury condition (P = .0005) but not surgeon group (P = .98). Pairwise comparisons of injury condition for both groups combined showed a significant decrease in stiffness from the UCL-I to the UCL-D state (P = .001), followed by a significant recovery from UCL-D to UCLR-IB condition (P = .002). As with torque, there was no difference in stiffness between the UCL-I and UCLR-IB conditions (P = .98).
Discussion
The results of the current study confirm that multiple surgeons can reproducibly achieve good restoration of joint stability without overconstraint. This study was initiated as a follow-up to a previous biomechanical study by Roth et al 16 that demonstrated that UCL repair with internal brace did not overconstrain the ulnohumeral joint. Roth et al also showed that repair of the ligament restored joint torque and stiffness to near-intact (not statistically different) levels from the intact state.
UCL repair has been increasing in volume recently despite having a poor early history and excellent outcomes with reconstruction. Primary UCL repair initially had poor outcomes, with no better than 63% of athletes returning to their previous level of play 12 ; however, these results were published before the advent of modern anchor technology, high-strength suture, and advanced rehabilitation programs. As a result, the UCL reconstruction, pioneered by Jobe et al, 9 became the gold standard for the treatment of all UCL injuries; however, despite excellent outcomes, the recovery was quite long, with return to full throwing and pitching at approximately 12 months after surgery. 3,23 Second, revision after traditional reconstruction has inferior outcomes, with only 50% of baseball players returning to previous level of play. 1 This led to renewed interest in alternative surgical options that could potentially offer faster recoveries and still allow for revision surgery in the future. Dugas et al 7 described a technique of repairing a torn UCL with suture tape (now called internal brace) augmentation. There have been other techniques described, 13,14,19 –22 all with the same indications of acute UCL injury with good ligamentous quality. In a study by Rothermich et al 18 of Division 1 National Collegiate Athletic Association baseball players who underwent UCL surgery, the proportion of patients who underwent UCL repair increased each year, from 10% in 2017, to 20% in 2018, and 25% in 2019.
Multiple biomechanical studies have followed these techniques to provide data regarding their constraint of the elbow joint after UCL repair. Dugas et al 8 demonstrated that UCL repair with augmentation had equal time-zero strength and ultimate failure loads when compared with reconstruction. A follow-up study demonstrated that UCL repairs with augmentation had significantly less gap formation at time zero as well as at the 100th and 500th cycles when compared with reconstruction. 10 Bachmaier et al 2 published a biomechanical study comparing UCL repair alone, UCL repair with internal brace augmentation, and UCL reconstruction with palmaris graft, finding that the UCL repair with augmentation provided statistically improved torsional resistance, loading capability, and decreased gap formation when compared with reconstruction and repair alone. Melbourne et al 11 compared internal brace augmentation with both UCL repair and UCL reconstruction and found that augmentation resulted in greater torque to failure in both procedures, with augmented stiffness values being similar to the native condition. Even more recently, Romeo et al 15 showed increased stiffness in augmented UCL repairs compared with 2 variations of repair alone but also showed it to be greater than the intact state.
In 2019, Dugas et al 7 published a study prospectively evaluating 111 overhead athletes ≥1 year after repair of the UCL with augmentation and found that athletes were able to return to competition at a mean time of 6.7 months. In 2020, Paletta and Milner 14 reported a 94% return to play at a mean time of 7.5 months in a cohort of 78 high school and college baseball players. Dugas et al 7 reported 5 complications from their cohort of 111 patients, with 3 related to either ulnar neuritis or instability, 1 due to heterotopic ossification, and 1 due to painful retained suture. A cohort of 40 nonprofessional overhead athletes with mean follow-up of 23.8 months were found to have a 92.5% return to play and mean Kerlan-Jobe Orthopaedic Clinic score of 92.6 after undergoing UCL repair by O’Connell et al. 13
Patients undergoing UCL repair have much shorter rehabilitation times, with most throwing athletes returning to competition by as early as 5 months postsurgery. 23 A 2021 study by Rothermich et al 17 reviewed 353 patients who underwent a UCL repair with the above-mentioned technique and found that 11.9% reported minor complications and only 3.4% required a return to the operating room for ulnar nerve debridement/exploration, primary ulnar nerve transposition, or heterotopic ossification excision. With the addition of this paper, we can conclude that the technique is reproducible in restoring elbow function without overconstraint.
Limitations
This study has some noteworthy limitations. We reproduced the same technique as a previous study 16 and positioned the elbows in 90° of flexion and full supination. Future consideration of testing the joint at other angles may provide further insight on the overall stability of the elbow during the throwing motion. The ligament was also “torn” from the distal insertion, where future studies could evaluate proximal or even midsubstance tears. Second, as the study was performed on cadaveric tissue, we are testing time-zero repair characteristics, rather than after allowing for healing and rehabilitation before stressing the repair, as in the normal patient postoperatively. Third, this study focuses on a specific repair technique that has been repeated by all the surgeons in the study group. As a result, our findings and conclusions may not extrapolate to all types of UCL repair techniques. Future studies may benefit from attempting to overconstrain the joint during the repair, or altering the anchor placement, to see whether variations in surgical technique can lead to unrecognized biomechanical changes to the joint.
Conclusion
UCL repair with internal brace is a reproducible procedure that provides consistent results among several surgeons when compared with a single surgeon. We also confirmed that the procedure does not lead to joint overconstraint while also returning the ligament to near-intact levels of resisting valgus stress. These findings, along with multiple biomechanical and outcome studies, help confirm that UCL repair is an excellent surgical option for throwing athletes with acute UCL injuries and good tissue quality.
Footnotes
Acknowledgment
The authors gratefully acknowledge Benton Emblom, Taylor Harris, Christian Merrill, Andrew Mundy, Zach Pharr, and John Ruder for their surgical contributions to this study.
Final revision submitted July 26, 2022; accepted August 30, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was sponsored by Arthrex in the form of direct funding as well as in-kind donations of cadaveric specimens and surgical products used in the completion of the study aims. S.N.K. has received grant support from Arthrex and education payments from Smith & Nephew. M.A.R. has received grant support from Arthrex and education payments from Smith & Nephew. J.R.D. has received consulting fees from Arthrex and DJO, nonconsulting fees from Arthrex, and royalties from Arthrex and In2Bones USA. E.L.C. has received education payments from Prime Surgical; consulting fees from Arthrex, DJO, and Zimmer Biomet; and nonconsulting fees from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.