
Abstract
Background:
In the current literature, studies on the anatomy of the anteromedial region of the knee are scarce. However, the anteromedial structures, especially the longitudinal medial patellar retinaculum (MPR), may play an important role in restraining external tibial rotation.
Purpose:
To conduct a layer-by-layer dissection of the anteromedial side of the knee and describe qualitatively and quantitatively the MPR anatomy pertaining to surgically relevant landmarks.
Study Design:
Descriptive laboratory study.
Methods:
A total of 10 fresh-frozen human cadaveric knees (mean age 81 ± 16.3 years) without history of previous ligament injury were used in this study. A layer-by-layer dissection was performed, and measurements were obtained using a tactile 3-dimensional (3-D) measuring arm to define the anatomy of the MPR in relation to surgically relevant landmarks, such as the superficial medial collateral ligament (sMCL) and medial patellofemoral ligament (MPFL). The 3-D datasets were used for multiplanar reconstruction.
Results:
The tibial and femoral attachment of the MPR were identified in 100% of cases. Layer-by-layer dissection confirmed its close topography to the sMCL. The mean length of the MPR was 84.9 ± 9.1 mm. The average width of the tibial and femoral attachment was 23.8 ± 3.1 mm and 69.2 ± 8.2 mm, respectively. The distance from the midpoint of the MPR tibial attachment to the midpoint of the distal tibial attachment of the sMCL was 27.2 ± 5.8 mm. Femorally, the MPR attached at the anterior border of the MPFL over a mean distance of 52.3 ± 9.4 mm.
Conclusion:
The MPR is a distinct tibiofemoral structure with well-defined tibial and femoral attachments, which could be consistently identified. Layer-by-layer dissection confirmed its close topography to the sMCL and MPFL.
Clinical Relevance:
As injuries to the anteromedial side of the knee may contribute to anteromedial rotational rotatory instability (AMRI), precise knowledge of the underlying anatomy of the MPR may be necessary to perform an anatomic reconstruction of the anteromedial side of the knee.
Keywords
Anterior cruciate ligament (ACL) rupture is a frequent sports-related injury, with consequent ACL reconstruction resulting in good to excellent clinical outcome. ‡ However, reported rates of residual graft laxity and failure after ACL reconstruction remain highly variable, ranging from 4% to 17% of cases. 23,27,32,33,47,48 In addition to psychological factors, tunnel malposition and type of graft used in ACL reconstruction, persistent rotatory knee instability possibly caused by concomitant collateral ligament tears, capsular, or meniscal injuries have been described as common causes for persistent ACL instability. 8,13,16,24,40,44
The concept of anteromedial rotatory instability (AMRI), which may be one reason for these recurrent ACL instabilities, was first introduced by Slocum and Larson in 1968. 39 This was defined as excessive valgus movement with simultaneous external rotation of knee leading to anterior subluxation of the medial tibial plateau relative to the adjacent femoral condyle, 12 which caused accompanying lesions of the medial compartment in approximately 20% to 62% of ACL ruptures cases. 2,11,38,45 In previous studies and anatomical observations, the posterior oblique ligament (POL) was suspected to be a key structure in restraining AMRI. 19 –22,42 However, recent biomechanical studies showed that the major restraint to AMRI is the deep medial collateral ligament (dMCL), superficial medial collateral ligament (sMCL), and the ACL, 4,15,35,44 which functions synergistically to the medial ligament complex to prevent AMRI and is a secondary restraint to valgus stress. 44 Thus, if the medial structures remain compromised, the ACL graft may be exposed to increased loads, which can potentially lead to graft failure. 5,6,28 To understand this relationship, a detailed knowledge of the medial knee anatomy is necessary.
Historically, the medial compartment was divided into 3 layers: fascia (layer 1), sMCL and MPFL (layer 2), and joint capsule (layer 3). 43 However, this qualitative description does not reflect the complexity of the anatomy of the medial side of the knee consisting of several overlapping ligaments, capsular thickenings, tendons, and tendons sheath. Especially, the anatomy of the anteromedial retinacular structures seems to be widely ignored. 6,26,35,36,43,44 Although Ball et al 4 only showed a less than 5% contribution of the medial patellar retinaculum (MPR) in restraining external tibial rotation, data from a study in our laboratory showed a significant contribution of the MPR and the anteromedial fascial structures of more than 20% in 30° and 60° of flexion. 18 Thus, it was speculated that the MPR is an important secondary restraint to AMRI.
The aim of the present study was to conduct a layer-by-layer dissection of the anteromedial side of the knee and describe qualitatively and quantitively the MPR anatomy pertaining to surgically relevant landmarks. It was hypothesized that the MPR is a distinct tibiofemoral structure with well-defined attachments.
Methods
Ten fresh-frozen human cadaveric knees from a local tissue bank were used for this study. There were 7 female and 3 male specimens, with a mean age of 81 ± 16.3 years. The knee specimens were dissected under permission of the Law on Corpses, Burials and Cemeteries (Burial Law) of the state of Schleswig-Holstein (section II, §9; February 4, 2005). None of the specimens had a history of previous ligament injuries or osteoarthritis. The dissection and all measurements were performed by the same orthopaedic surgeon, who specializes in knee surgery and acts as a senior consultant.
Dissection Technique
The knee specimens were stored at -20 °C and thawed for 24 hours at room temperature before anatomic dissection. All the knees underwent a layer-by-layer dissection to systematically expose and identify the respective structures of the anteromedial corner of the knee. Dissection was performed at 30° of flexion to ensure a slight prestressing of the structures to be examined. Firstly, all specimens were prepared by cutting the femur and tibia approximately 250 mm from the joint line. After removal of skin and subcutaneous tissue while preserving the fascia and the muscles, the superficial anserine pes and the medial femoral epicondyle were identified as reference points. Between them, a dense layer of the crural fascia was revealed. After its longitudinal incision proximal to the medial femoral epicondyle, the crural fascia was carefully separated anteriorly and posteriorly from the sMCL. Subsequently, the sartorius fascia was dissected sharply at the upper edge of superficial anserine pes. Then, the tendons of the sartorius, gracilis, and semitendinosus muscle were transected at the level of the sMCL posterior border and reflected anteriorly.
After locating the sMCL and POL, the crease of the fusion of layers 1 and 2 was marked as the posterior border of the MPR and it was released from the anterior border of the sMCL. Next, the longitudinal fibers of the MPR were cut horizontally at the level of the joint line towards the patellar tendon. The distal part of the MPR was carefully separated from the joint capsule (layer 3) while preserving the medial patellotibial ligament (MPTL) and dissected distally up to its bony attachment of proximal tibia. After detaching the proximal part of the MPR from the joint capsule proximally and medially, the bony and ligamentous insertion of the MPR at the patella and medial patellofemoral ligament (MPFL) were identified. Finally, the osseous insertion of the MPFL between the medial epicondyle and the adductor tubercule was exposed.
Measurements and Photographic Documentation
Measurements of size, length and width, location of the femoral and tibial attachment, and the distance to other bony landmarks (medial femoral epicondyle, adductor tubercule, gastrocnemius tubercule, and tibial tuberosity) were performed between each step of the dissection in 0° knee flexion. Quantitative measurements of the dissected structures were obtained using a tactile 3-dimensional measuring arm (Absolute Arm 8320-7, Hexagon Metrology GmbH) with an accuracy of ±0.05 mm. Each step of the dissection was documented by a 12-megapixel digital camera (Canon EOS Rebel T5i).
Data Processing and Statistical Analysis
Data analysis was performed using a metrology software (PC-DMIS 2019 R1, Hexagon Metrology GmbH), which can create an x-y-z coordinate system and precisely measure objects in a 3-dimensional (3-D) space. The axes of the coordinate system were defined as the femoral shaft axis (y-axis) and a plane through the femoral epicondyles (x- and z-axes). The bony landmarks, eg, the medial femoral epicondyle, were identified by palpation and inspection and the tips were digitalized by using a touch trigger probe. The digitalized measuring points of the footprints of the ligamentous structures were approximated by the metrology software as an ellipse and the length, width, and area of the footprints were then determined (Figure 1). The calculated centers of the footprints and the tips of the bony landmarks served as the reference to determine the shortest distance between the respective anatomical structures. All measurements were expressed as mean and standard deviation.
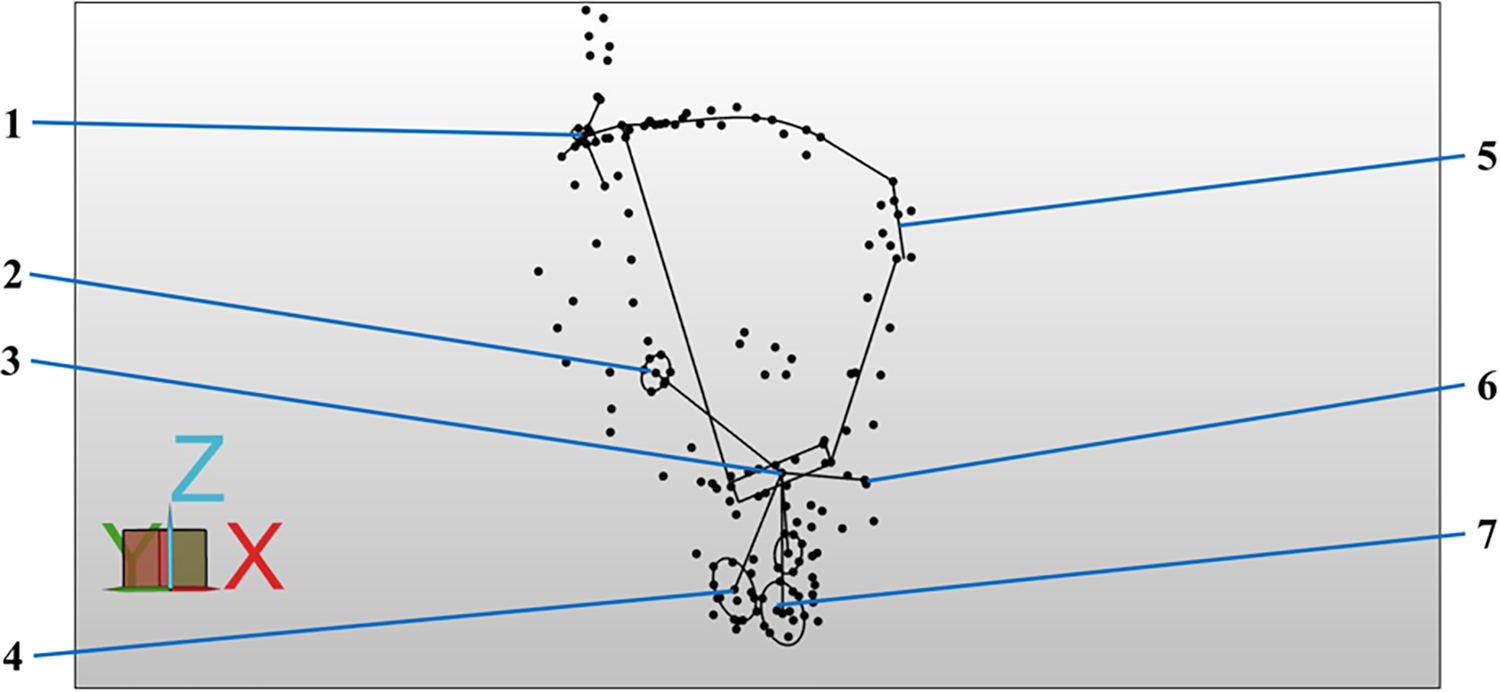
Screenshot of the metrology software from a single specimen while data processing of a left knee. Each dot represents an anatomical landmark, which were digitalized using a touch trigger probe. The boundaries of an anatomical structure were digitalized using multiple measuring points to represent the 3-D shape of each structure in the x-y-z coordinate system. The entirety of measuring points were approximated as a geometric figure, eg, a line or an ellipse, that resembles the in situ shape of each anatomical structure. 1, Femoral attachment of MPFL; 2, proximal tibial attachment of sMCL; 3, tibial attachment of MPR; 4, distal tibial attachment of sMCL; 5, patellar attachment of MPFL; 6, tip of tibial tuberosity; 7, attachment of semitendinosus tendon. 3-D, 3-dimensional; MPFL, medial patellofemoral ligament; MPR, medial patellar retinaculum; sMCL, superficial medial collateral ligament.
Results
Qualitative Approach
After dissection, the MPR was found as a superficial ligamentous structure in all specimens on the anteromedial side of the knee. This structure was located extracapsular in the anterior third of the medial side of the knee and could be distinguished easily from the underlying medial patellotibial ligament (MPTL) and articular capsule.
The most superficial layer was formed by the transverse fibers of the MPR, which covered the entire medial compartment of the knee and blended with the crural fascia and fascia lata (Figure 2A). At the most anterior edge of the medial compartment, a confluence of the transverse and longitudinal fibers of the MPR was found (Figure 2B).

Photographs of the medial side of a left knee specimen. After removal of the skin and subcutaneous tissue, the transverse fibers of the medial patellar retinaculum (MPR) could be identified. (A) The forceps is demonstrating the transverse fibers of the MPR. (B) After a longitudinal incision of the transverse fibers, the underlying longitudinal fibers appeared. The forceps is holding the anterior part of the transverse fibers demonstrating the confluence of the transversal and longitudinal fibers at the most anterior edge of the medial compartment. 1, Vastus medialis muscle covered with fascia lata; 2, sartorius fascia; 3, tendon of the sartorius muscle after removal of the sartorius fascia; 4, longitudinal fibers of the MPR; *, patella. MPR, medial patellar retinaculum.
In all specimens, layer-by-layer dissection confirmed its close topography to the sMCL. Anterior to the longitudinal fibers of the sMCL, layers 1 and 2 merged together forming the MPR. In this region, the crease of this merging zone formed the posterior border of the MPR (Figure 3). The oblique longitudinal fibers of the MPR formed a trapezoid-like shape, with its postero-proximal portion bending towards the medial femoral epicondyle (Figure 4).

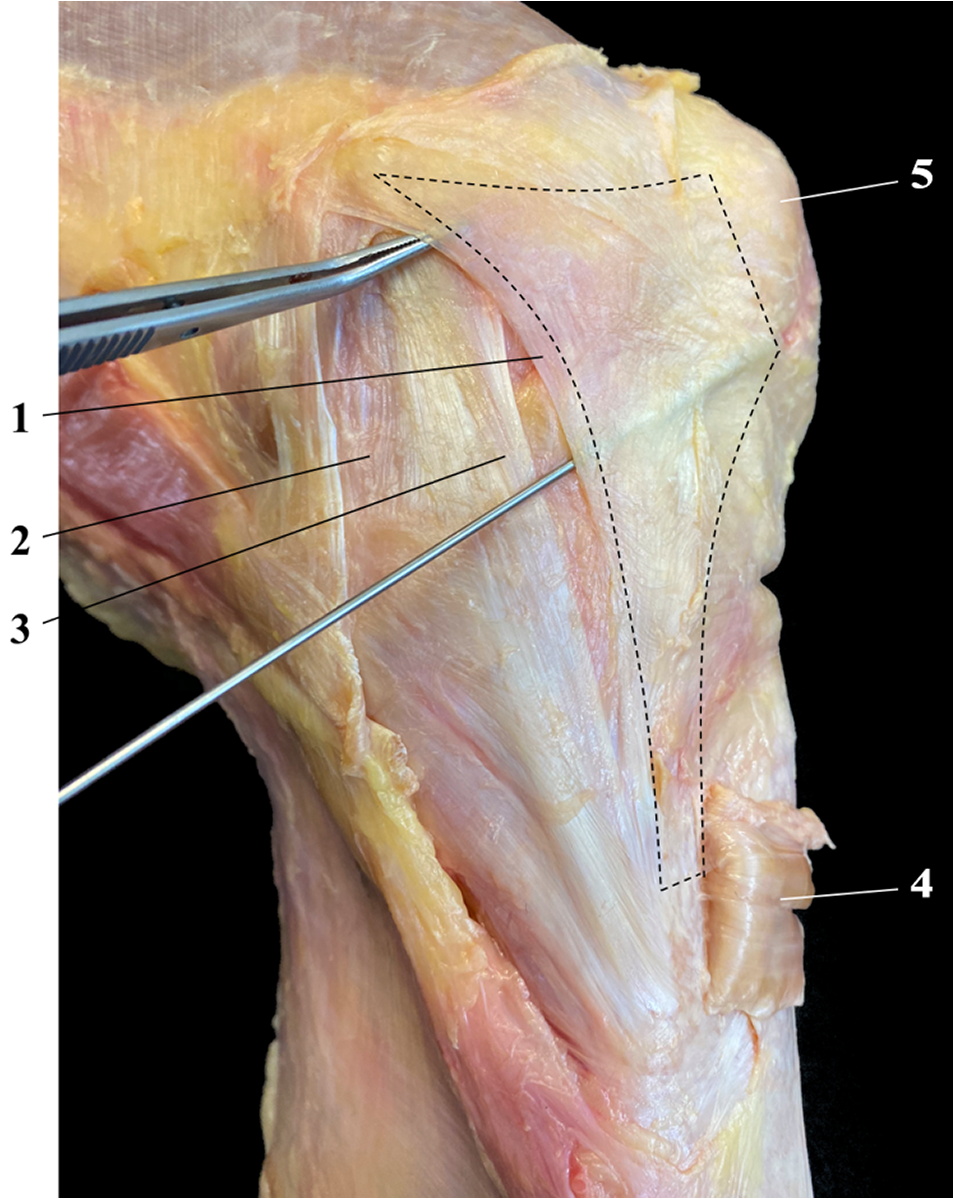
Photograph of the medial side of a left knee specimen. After removal of the sartorius fascia, the crural fascia was longitudinally incised between the medial femoral epicondyle and the superficial anserine pes and separated anteriorly from the sMCL. The forceps is holding the reflected crural fascia demonstrating the merging zone of layer 1 and layer 2 forming the posterior border of the MPR. 1, Crural fascia (layer 1) cut and retracted; 2, crease of the merging zone of layer 1 and layer 2 forming the posterior border of the MPR; 3, longitudinal fibers of the sMCL; 4, sartorius muscle after removal of the sartorius fascia. MPR, medial patellar retinaculum; sMCL, superficial medial collateral ligament.
Photograph of the medial side of a left knee specimen. After removal of the crural and sartorius fascia, and transection of the superficial anserine pes, the trapezoid-like shape of the MPR (dashed lines) is outlined. The forceps is demonstrating the crossing of the posterior border of the MPR superficial to the sMCL. 1, Posterior border of the MPR; 2, POL 42 ; 3, longitudinal fibers of the sMCL; 4, superficial pes anserine reflected; 5, patella. MPR, medial patellar retinaculum; POL, posterior oblique ligament; sMCL, superficial medial collateral ligament.
Tibial Attachment
In all specimens, the longitudinal fibers attached to the bone close to the distal tibial attachment of the sMCL. The footprint of the tibial attachment formed an elongated oval shape and converged with the distal tibial attachment of the sMCL (Figure 5A). The tibial attachment extended anteriorly from the sMCL towards the tibial tuberosity (Figure 5B).

Photographs of the medial side of a left knee specimen. After a horizontal incision of the longitudinal fibers of the MPR toward the patellar tendon at the level of the joint line, the distal part of the MPR was separated from the joint capsule (layer 3). The MPTL was preserved and dissected distally up to its bony attachment of the proximal tibia. (A) The forceps are demonstrating the distal portion of the MPR. 1, Tibial attachment of the longitudinal fibers; 2, merging zone (white circle) of the distal tibial attachment of the sMCL and tibial attachment of the MPR; 3, distal tibial attachment of the sMCL. (B) Distal portion of the MPR is reflected distally. 4, MPTL; 5, anteromedial tibia; 6, tibial attachment of the MPR. The white circle demonstrates the close topography between the tibial attachment of the MPR and sMCL. MPR, medial patellar retinaculum; MPTL, medial patellotibial ligament; sMCL, superficial medial collateral ligament.
Femoral Attachment
The femoral attachment of the MPFL was found in a groove between the medial femoral epicondyle (ME), the adductor tubercule (AT), and the gastrocnemius tubercule (GT). In all dissected specimens, the longitudinal fibers attached indirectly via the medial patellofemoral ligament (MPFL) on the distal femur, on the vastus medialis obliquus muscle (VMO), and on the patella (Figure 6A). Femorally, the longitudinal fibers of the MPR merged with the transverse fibers of the MPFL in criss-cross pattern. When dividing the MPFL into thirds, the MPR inserted at the anterior two-thirds of the MPFL. The boundary between the MPR and the MPFL was defined macroscopically based on the different orientation of fibers. The most posterior insertion of the MPR was at the level of the anterior border of the sMCL, therefore the MPR covered nearly the whole anteromedial side of the knee (Figure 6B).
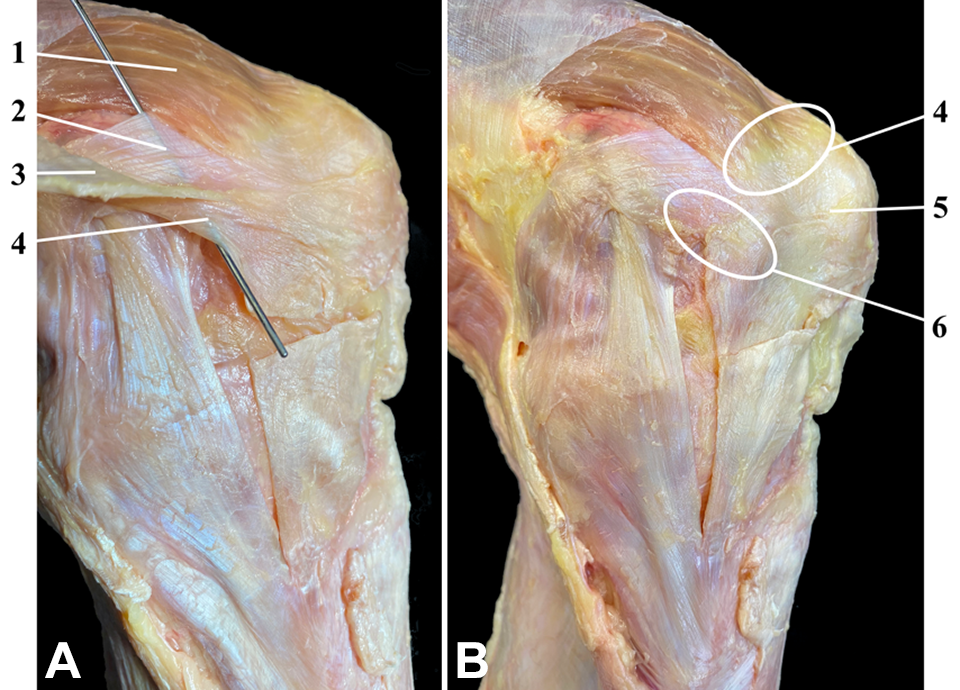
Photographs of the medial side of a left knee specimen. The fascia lata was dissected from the quadriceps muscle and reflected medially to identify the MPFL. The probe is demonstrating the femoral attachment of the longitudinal fibers of the MPR into the MPFL. (A) Proximal portion of the MPR. 1, VMO muscle; 2, MPFL; 3, fascia lata retracted; 4, posterior proximal fibers of the MPR crossing the sMCL. (B) Overview of the entire longitudinal fibers of the MPR. The circles highlight the merging zones of the VMO, MPFL, and MPR. 4, Insertion of the VMO in the MPFL, while the white circle highlights the attachment of the VMO and MPFL at the proximomedial apex of the patella; 5, patellar attachment of the MPFL; 6, attachment of the longitudinal fibers of the MPR into the MPFL. MPFL, medial patellofemoral ligament; MPR, medial patellar retinaculum; MPTL, medial patellotibial ligament; sMCL, superficial medial collateral ligament; VMO, vastus medialis obliquus.
Quantitative Approach
The mean length (proximal to distal) and width (medial to lateral) of the tibial footprint of the MPR (TFMPR) was 23.8 ± 3.1 and 4.5 ± 1.0 mm, respectively. The mean area of the TFMPR was 106.7 ± 22.2 mm2. The measurements confirmed the close topographical proximity between the tibial attachment of the sMCL and the MPR. The mean distance between the center of the sMCL and MPR tibial footprint was 27.2 ± 5.8 mm. The distance between the center of the TFMPR and the tip of the tibial tuberosity was 28.4 ± 5.2 mm. Thus, it attached midway between sMCL and tibial tuberosity.
The mean length and width of the femoral footprint of the MPFL (FFMPFL) was 8.8 ± 1.3 and 4.2 ± 1.4 mm, respectively. The mean area of the FFMPFL was 87.1 ± 19.9 mm2. The width of the MPFL increased as it coursed from the femoral attachment site to the medial border of the patella. The mean width and length of the patellar attachment of the MPFL was 21.7 ± 3.1 and 3.5 ± 1.3 mm, respectively. Similarly, the mean area of the patellar footprint of the MPFL was 91.9 ± 23.5 mm2. In addition, the MPFL had firm insertions into the VMO and the MPR. The attachment of the MPR on the MPFL occurred with a mean distance from the center of the FFMPFL of 11.3 ± 3.9 mm. The average length of the MPR attachment on the MPFL was 52.3 ± 9.4 mm.
Measurements of the Attachments of the MPR and the MPFL After Anatomical Dissection a

a The mean distances of the anatomical structures were determined between the centers of the attachments and the tip of the bony landmark. Length, width, and distance are measured in millimeters; area is measured in mm2. AT, adductor tubercle; FFMPFL, femoral footprint MPFL; GT, gastrocnemius tubercule; ME, medial femoral epicondyle; MPFL, medial patellofemoral ligament; MPR, medial patellar retinaculum; PBMPR, posterior border MPR; PFMPFL, patellar footprint MPFL; semiT, semitendinosus; sMCL, superficial medial collateral ligament; TFMPR, tibial footprint MPR; TT, tibial tuberosity.
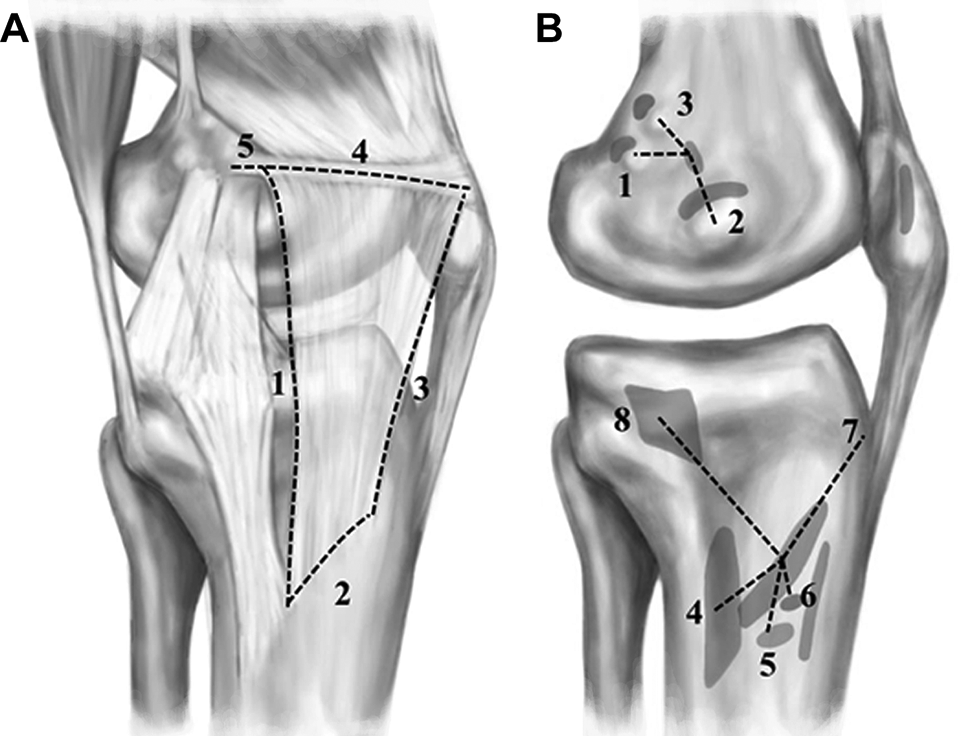
Illustration of the anatomy of the MPR. Measurement values are from Table 1. (A) Topographical proximity between the MPR, sMCL, and MPFL: 1, length of the posterior border (84.9 ± 9.1 mm); 2, length of the TFMPR (23.8 ± 3.1 mm); 3, length of the anterior border (52.8 ± 5.3 mm); 4, length of the upper border (52.3 ± 9.4 mm); 5, distance between FFMPFL and MPR insertion on the MPFL (11.3 ± 3.9 mm). (B) Tibial and femoral attachments of the medial structures of the knee: 1, distance between FFMPFL and gastrocnemius tubercle (11.7 ± 4.2 mm); 2, distance between FFMPFL and adductor tubercle (9.7 ± 3.1 mm); 3, distance between FFMPFL and medial epicondyle (13.7 ± 4.3 mm); 4, distance between TFMPR and distal tibial attachment of the sMCL (27.2 ± 5.8 mm); 5, distance between TFMPR and attachment of the semitendinosus tendon (24.6 ± 6.2 mm); 6, distance between TFMPR and attachment of the gracilis tendon (18.6 ± 6.2 mm); 7, distance between TFMPR and tibial tuberosity (28.4 ± 5.2 mm); 8, distance between TFMPR and proximal tibial attachment of the sMCL (46.2 ± 9.7 mm). FFMPFL, MPFL femoral footprint; MPFL, medial patellofemoral ligament; MPR, medial patellar retinaculum; MPTL, medial patellotibial ligament; sMCL, superficial medial collateral ligament; TFMPR, tibial footprint of the MPR.
Discussion
The most important finding of the present study was that the MPR is a distinct tibiofemoral structure with well-defined tibial and femoral attachments, which could be identified consistently. Layer-by-layer dissection confirmed the close topographical proximity between the tibial attachments of the sMCL and MPR. Tibially, the MPR attached anterior to the sMCL directly to the bone, while firm fibers of the sMCL and MPR merged together. At the femoral insertion site, the MPR attached indirectly via the MPFL to the distal femur and the vastus medialis obliquus muscle, forming a dynamic stabilizer on the anteromedial side of the knee.
The medial side of the knee plays an important role in maintaining coronal stability and restraining rotatory instability, especially in the presence of concomitant ACL injuries. Even though Müller 30 described the longitudinal MPR as a dynamic anteromedial stabilizer in 1982, the anatomy of the anteromedial retinacular structures seemed to be widely ignored in recent biomechanical studies. 6,26,35,36,43,44 Jagodzinski et al 22 showed that the longitudinal fibers of the MPR attached to the proximal tibia anteriorly and proximally to the distal tibial attachment of the sMCL. This is confirmed by the results of the present study, which outlined the close topographical proximity between the centers of the tibial attachments of the longitudinal MPR and the sMCL (distance from MPR to sMCLdistal = 27.2 ± 5.8 mm). It could also be shown, that the MPR consistently emerged from the anterior edge of the sMCL, covering the anteromedial half of the knee in its further course, like a distinct ligament. The tibial attachment of the longitudinal MPR also lies on the Burmester curve, which represents circular arcs of quasi-isometric ligaments, to guarantee stability during the full range of motion. 29 This fact may emphasize the importance of the MPR in restraining medial knee instability.
In contrast to the bony tibial attachment of the MPR, several authors showed that the longitudinal fibers further coursed femorally into the fascia lata and quadriceps tendon without a distinct attachment on the distal femur. 9,22,25,43 As a new aspect, the present study found an attachment on the anterior 3 thirds of the MPFL. Due to this indirect attachment on the femur and the patella via the MPFL, the trapezoid-like shape, and the possible dynamization from the quadriceps muscle, the MPR may act as a dynamic anteromedial stabilizer, as already speculated by Müller 30 .
The main trauma mechanism of an ACL rupture can lead to accompanying injuries of the medial compartment of the knee. The most common are the sMCL and dMCL, which occur with an incidence varying from 20% to 62%. 2,7,11,38,45,49 Even though the sMCL and dMCL are important restraints to external tibial rotation, 44,46 the overlying MPR has also been shown to contribute more than 20% in restraining external tibial rotation at 20° and 30° knee flexion in an laboratory study. 18 The posteromedial structures, such as the POL, however, had no significant contribution in restraining AMRI in recent biomechanical studies. 46 Thus, it seems logical that a combined sMCL and anteromedial reconstruction may better restore anteromedial knee kinematics than a combined sMCL and POL reconstruction. Therefore, it is important to evaluate the anatomy of these anteromedial structures, such as the MPR, to develop suitable reconstructions. This assumption is supported by a recent biomechanical study by Willinger et al 46 , which evaluated the dMCL as a potential structure for anteromedial reconstruction.
Limitations
The present study had some limitations inherent to anatomical studies. The mean age of the specimens was 81 ± 16.3 years, which does not reflect the typical patient for a medial knee injury, whereas the occurrence of AMRI has been described in younger, athletic population. Furthermore, previous to anatomic dissection the femur and tibia were cut, which may have changed the measurements due to loss of tension of the MPR. In addition, the present study mentioned only the MPTL, whereby additional medial patellar ligaments, like the medial quadriceps tendon femoral ligament (MQTFL) and medial patellomeniscal ligaments (MPML), were identified. 9,25,41 However, the MQTFL and MPML course transversely and obliquely, respectively, through the anteromedial side of the knee, which ruled out a confusion with the longitudinal fibers of the MPR. The dissection and measurements were performed by a single surgeon. Thus, the variability of our results, which might be expected if another investigator were to repeat these measurements, was not assessed. Nevertheless, a strength of this study is the precise quantitative and qualitative identification of the tibial and femoral attachments of the MPR in all specimens.
Conclusion
The MPR is a distinct tibiofemoral structure with well-defined tibial and femoral attachments, which could be identified consistently. Layer-by-layer dissection confirmed its close topography to the sMCL and the MPFL. As injuries to the anteromedial side of the knee may contribute to AMRI, precise knowledge of the underlying anatomy of the MPR is necessary to develop suitable reconstructions of the anteromedial side of the knee.
Footnotes
Acknowledgment
The authors thank Jens Wermers, MSc, for his contribution to the study conception and acquisition of data as well as Leslie von Hegedorn for illustrating the graphics.
Notes
Final revision submitted July 7, 2022; accepted August 12, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: the authors acknowledge financial support from the Open Access Publication Fund of the University of Münster. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.