
Abstract
Background:
Patellar dislocation is a common injury in children and adolescents. There is a lack of information about concomitant osteochondral lesions in these patients.
Hypothesis:
We hypothesized that the likelihood of chondral or osteochondral lesions would increase with each prior patellar dislocation and that the appearance of lesions in surgically treated children and adolescents would be influenced by age, sex, injury mechanism, and body mass index (BMI).
Study Design:
Case-control study; Level of evidence, 3.
Methods:
Inclusion criteria were (1) age <18 years, (2) surgical treatment with diagnostic arthroscopy of the knee including description of chondral and osteochondral lesions, and (3) maximum time period between the last patellar dislocation and presentation in our department of 6 weeks and maximum of 4 weeks between presentation and surgery. A total of 153 children (173 knees) with a mean age of 13.0 ± 2.1 years were included. All surgical reports and intraoperative arthroscopic imaging were analyzed retrospectively for the location and severity of lesions. The likelihood of lesions was calculated with multiple stepwise regression models regarding injury mechanism, number of dislocations, sex, age, physeal closure, and BMI.
Results:
The regression model to predict femoral lesions was statistically significant (χ2[5] = 26.55; P < .001) and identified male sex, BMI ≥25, traumatic injury mechanism, and physeal closure as independent factors associated with the appearance of femoral lesions. The second regression model predicting the appearance of patellar lesions was also statistically significant (χ2[4] = 26.07; P < .001) and identified the traumatic injury mechanism as a single independent predictor for patellar lesions.
Conclusion:
BMI ≥25, male sex, and physeal closure were factors significantly associated with femoral chondral and osteochondral lesions in our cohort. In case of traumatic lateral patellar dislocation (LPD), the likelihood of patellar and femoral chondral and osteochondral lesions is significantly higher than in nontraumatic LPD. Early magnetic resonance imaging and surgical treatment should be considered in obese patients, male patients, and patients with physeal closure and after traumatic LPD.
Patellar dislocation is a common injury in skeletally immature patients with an incidence of 47 per 100,000. It represents 3% of all knee injuries in both children and adults. 16,17 The incidence of patellofemoral instability peaks between 11 and 14 years of age, 12 and 60% to 70% of patellar dislocations occur during sports. 17 Owing to its multifactorial etiology, treating patellofemoral instability can be challenging for orthopaedic surgeons. 12
Dislocation of the patella not only causes damage of soft tissue structures, but also may lead to chondral and osteochondral defects. 20 In almost all cases, the patellar surface slides over the lateral femoral condyle, leading to consecutive contusion of the medial rim of the patella and/or the lateral femoral condyle. 20 Medial dislocations are rare and mostly iatrogenic. 8
Several clinical studies on recurrent patellar dislocations in skeletally immature patients have been published 1,5,12,16,17 ; these studies focused on a comparison of different surgical techniques and the risk of postoperative redislocation. Currently, there is a lack of information about concomitant osteochondral lesions in these patients. In this study, we retrospectively analyzed surgically treated children and adolescents with lateral patellar dislocation (LPD) regarding chondral or osteochondral lesions. We expected that the likelihood of lesions would be influenced by number of prior dislocations, age, sex, injury mechanism, and body mass index (BMI).
Methods
This study was approved by the local ethics committee. Parents/guardians of all patients provided informed assent and consent. Inclusion criteria were (1) age <18 years, (2) surgical treatment from October 2015 to March 2020 with diagnostic arthroscopy of the knee including description of chondral and osteochondral lesions, and (3) maximum time between the last patellar dislocation and presentation in our department of 6 weeks and maximum of 4 weeks between presentation and surgery.
As von Engelhardt et al 21 showed that the value of precise grading of cartilage lesions on magnetic resonance imaging (MRI) is limited, especially in the femoropatellar joint (FPJ), this study was based only on intraoperative arthroscopically described lesions as the most specific way for describing chondral and osteochondral lesions. In case of a primary patellar dislocation without a concomitant chondral lesion or only a grade 1 lesion on MRI, nonsurgical treatment is recommended in our institution. Thus, these patients were excluded.
A total of 153 children (111 girls and 42 boys, 173 knees) were included with a mean age of 13.0 ± 2.1 years (range, 5-17 years). All operations were performed by 1 of 3 senior pediatric orthopaedic surgeons (including M.R. and O.D.J.) at a single pediatric orthopaedic center. Twelve children (16 knees) with conditions such as trisomy 21, DiGeorge syndrome, Larsen syndrome, or Marfan syndrome and with either chronic LPD or >20 LPDs were analyzed as a separate group due to the differing etiology of LPD and different daily life activity levels compared with idiopathic cases (Figure 1).

Study flowchart. LPD, lateral patellar dislocation.
All surgical reports and intraoperative arthroscopic imaging were analyzed retrospectively to determine the location and severity of chondral lesions. The Outerbridge classification was used by the operating surgeon to describe the intraoperative findings. 18 All lesions detected were included in the analyses. The femoral localization was documented according to Cahill and Berg 1 (Figure 2A), and we used our own classification for localization of patellar lesions (Figure 2B). Some variables were grouped into categories for inclusion in the statistical model. Clinical cutoff values were used when available. BMI was divided into 2 groups for the regression model, based on the common World Health Organization classification of <25 representing normal weight and ≥25 representing patients with (pre)obesity. 22 The variables of patient age and number of previous dislocations were treated as continuous variables because no evident clinical cutoff values were available to depict correlations with Outerbridge grading. Injury mechanism was indicated as either traumatic or atraumatic. Bone age was operationalized by a binary variable characterizing physeal closure or an open physis.

Location documentation of (A) femoral condyle lesions according to Cahill and Berg 1 and (B) patellar lesions.
Sample Size Calculation
The sample size for the regression analysis was calculated a priori considering the expected effect size, power, and design effect with G*Power (Version 3.1.9.2; Heinrich Heine University). Based on missing research results to date, a small to medium effect of f 2 = 0.1 was assumed. With an alpha risk of .05 and a statistical power of 0.8, a sample size of 143 was required to calculate a regression model with 6 independent predictors.
Statistical Analysis
Descriptive statistics were used to summarize the demographics and clinical characteristics of patients included. Continuous variables are expressed as mean ± SD, whereas categorical variables are expressed as number and percentage. To determine whether the severity of osteochondral lesions (defined by the Outerbridge grade) can be predicted by age, sex, BMI, injury mechanism, number of dislocations, and physeal closure, a multiple and stepwise regression analysis was performed. In total, 2 regression analyses were performed: a risk factor model to determine the cartilage defects of the femur and another risk factor model to determine the cartilage defects of the patella. After the regression analyses, odds ratios (ORs) with 95% CIs were calculated for significant predictors. For computation of the ORs, the Outerbridge grade was regrouped into grades 0 to 2 versus grades 3 to 4. A P value <.05 was deemed significant. Statistical analyses were performed using SPSS statistical software (Version 27.0; IBM SPSS Statistics).
Results
In our cohort of 157 knees, the mean number of dislocations was 3.9 ± 3.2 (range, 1-10) and the mean BMI was 21.6 ± 5.1 (range, 14.7-33.4). A total of 76 knees had a closed physis and 81 knees had an open physis. We defined 70 dislocations as traumatic, caused by knee distortion during sports or a fall from a scooter or bicycle.
A total of 41 knees had only 1 dislocation but a chondral lesion of Outerbridge grade ≥2 on MRI, an indication for diagnostic arthroscopy; 43 knees had 2 dislocations; and 73 knees had >2 dislocations and therefore met the indication for surgical treatment.
Children with an open physis were treated with soft tissue patellar tendon transfer (Goldthwait procedure) and medial repair (n = 69) as the preferred method in the study clinic. In case of physeal closure and a pathological tibial tubercle–trochlear groove (TT-TG) distance of >15 mm, a medialization of the tibial tubercle (Elmslie-Trillat procedure) and medial repair was performed (n = 58) (Figure 3). In case of physiologic TT-TG distance, reconstruction of the medial patellofemoral ligament was the surgical procedure of choice (n = 18) (Figure 4). Arthrotomy and open refixation of an osteochondral lesion had to be performed in 12 knees.

Preoperative, intraoperative, and postoperative images from a 14-year-old girl (body mass index, 27.3) with a grade 4 osteochondral lesion of the lateral femoral condyle after an Elmslie-Trillat procedure (using 4.8-mm absorbable magnesium screws) and refixation of an osteochondral fragment of the lateral femoral condyle (using 2.0-mm absorbable magnesium pins). MRI, magnetic resonance imaging; postop, postoperative.

(A) Preoperative knee magnetic resonance imaging (MRI) from an 11-year-old boy with an osteochondral tear of the medial patellofemoral ligament after lateral patellar dislocation (arrow). (B) postoperative MRI after refixation with 2.4-mm absorbable magnesium screws.
In the 41 primary dislocations, the indication for surgery was the cartilage lesion. Of the remaining 116 knees with >1 dislocation, there were chondral or osteochondral lesions in 52 knees (45%). Among the 157 knees, 22 had isolated patellar lesions, 26 had isolated femoral lesions, and 45 had both femoral and patellar lesions. A total of 138 lesions were detected (Outerbridge classification: n = 36, grade 1; n = 51, grade 2; n = 11, grade 3; n = 40, grade 4). Of these 138 lesions, 12 (9%) were osteochondral lesions that required fixation with magnesium-based absorbable implants, 28 lesions (20%) required microfracturing, 62 lesions (45%) required chondroplasty, and 26% of the lesions required no surgical treatment. The locations of the chondral and osteochondral lesions are listed in Table 1. Most lesions were in areas 5A and 5B and in areas 6b and 6c. No osteochondral lesions were seen in areas 1 to 3 or 7 (Table 1).
Lesion Location and Grade a

a LFC, lateral femoral condyle.
b According to Outerbridge classification: grade 1, smooth cartilage surface; grade 2, partial-thickness defect ≤50% of cartilage thickness; grade 3, defect >50% of cartilage thickness; grade 4, full-thickness defect and osteochondral defect.
In the separate cohort of 12 children (16 knees) with congenital syndromes (n = 8, trisomy 21; n = 2, DiGeorge syndrome; n = 1, epiphyseal dystrophia; and n = 1, arthrogryposis multiplex congenital), the mean age was 6.5 years (range, 2-17 years). No chondral or osteochondral lesions were detected in this group.
Factors Associated With Chondral and Osteochondral Lesions
Stepwise logistic regression analyses were performed on all 157 knees to ascertain the effects of age, sex, BMI, traumatic mechanism, number of prior dislocations, and whether physis was open or closed on the likelihood of chondral and osteochondral lesions of the femur or patella. The regression model to predict femoral lesions was statistically significant (χ2[5] = 26.55; P < .001) and identified male sex, BMI ≥25, primary traumatic mechanism, and physeal closure as independent predictors associated with the appearance of femoral lesions. The data for number of dislocations were excluded from the overall model by stepwise regression due to a bimodal distribution. Traumatic injury mechanism increased the appearance of a femoral Outerbridge grade 3 or 4 chondral and osteochondral defect by a factor of 7 (95% CI, 1.8-31.9). In addition, physeal closure had a significant influence and increased the odds for femoral lesions by a factor of nearly 4 (OR = 3.9; 95% CI, 1.2-11.2) (Table 2).
Logistic Regression for Independent Predictors of the Appearance of Cartilage Defects of the Femur a
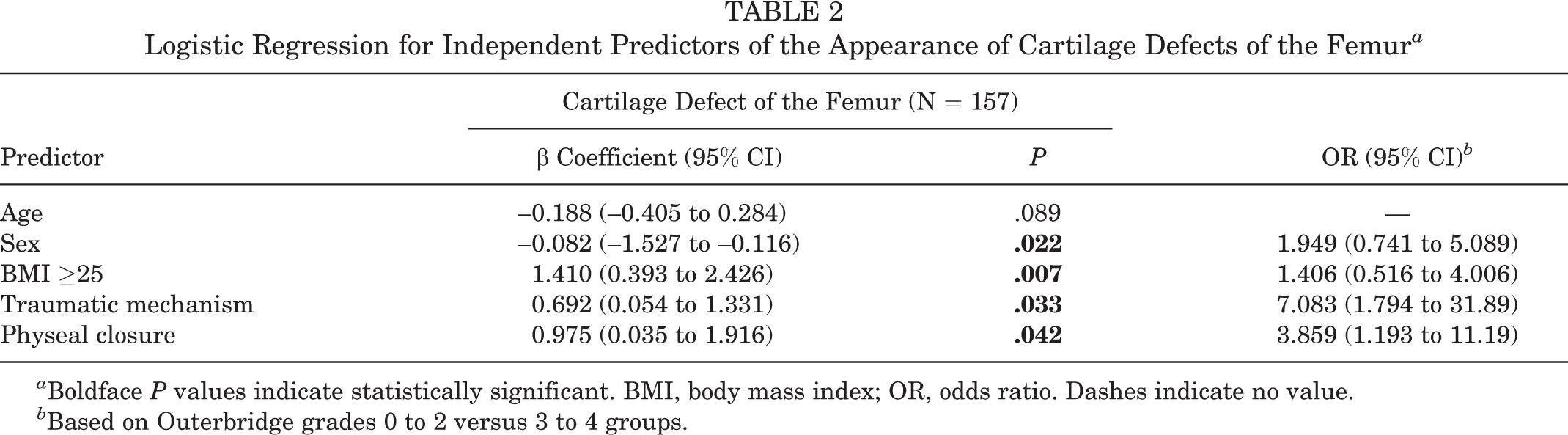
a Boldface P values indicate statistically significant. BMI, body mass index; OR, odds ratio. Dashes indicate no value.
b Based on Outerbridge grades 0 to 2 versus 3 to 4 groups.
The second regression model predicting the appearance of patellar lesions was also statistically significant (χ2[4] = 26.07; P < .001) and identified traumatic injury mechanism as the single independent factor for patellar lesions. The variables BMI, bone age, and number of dislocations were excluded by the stepwise regression for patellar lesions, whereas patient age and sex were nonsignificant in the overall model. Traumatic injury mechanism was a highly significant predictor for patellar cartilage lesions and increased the risk by a factor of 42 (95% CI, 6.6-437.5) (Table 3).
Logistic Regression for Independent Predictors of the Appearance of Cartilage Defects of the Patella a
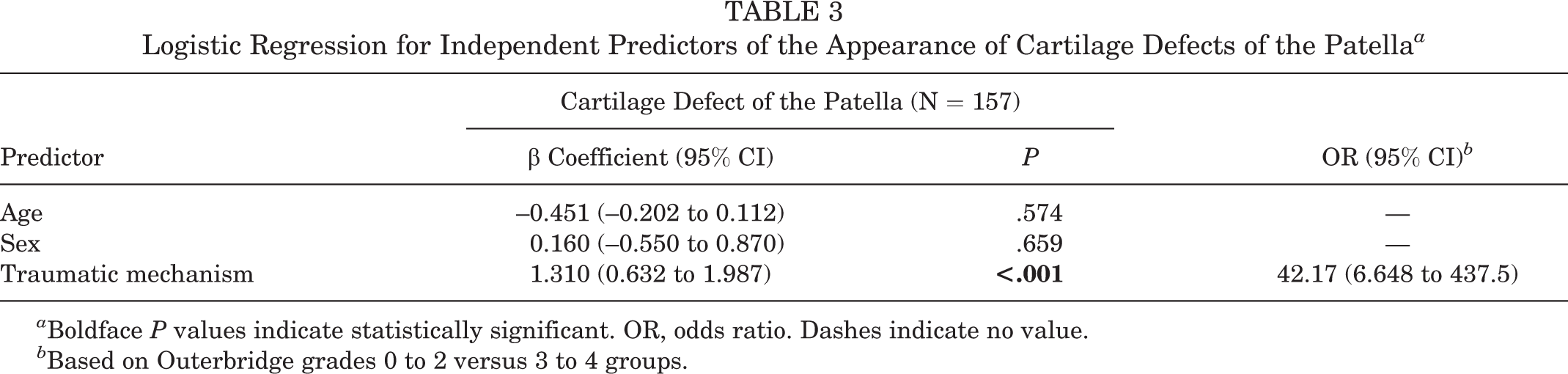
a Boldface P values indicate statistically significant. OR, odds ratio. Dashes indicate no value.
b Based on Outerbridge grades 0 to 2 versus 3 to 4 groups.
Discussion
This study has reported the localization and likelihood of chondral and osteochondral lesions in surgically treated children and adolescents after patellar dislocations. In 41 primary dislocations the reason for surgery was a cartilage lesion, but among the other 116 surgically treated knees with recurrent dislocations, 45% had additional chondral or osteochondral lesions. In summary, in our cohort the likelihood for femoral chondral and osteochondral lesions in surgically treated children and adolescents after LPD was significantly associated with a BMI ≥25, male sex, and physeal closure. In case of traumatic LPD, the likelihood for patellar and for femoral chondral and osteochondral lesions was significantly higher. The OR analysis revealed that a traumatic event increases the likelihood of lesions by a factor of 7 on the femur and a factor of 42 on the patella. Nevertheless, it should be noted that the 95% CI is very broad. To the best of our knowledge, this is the only series of chondral lesions in surgically treated patients in this age group in the literature.
Recurrent Patellar Dislocation
Nonsurgical treatment of primary dislocations is considered to be the standard of care. 2,3,10 However, with high rates of redislocation of up to 31% to 69% after conservatively treated primary patellar dislocation 11,13,16 and better results after surgery, the operative stabilization of the patella after primary dislocation is being increasingly recommended. 16,17 Neither the systematic review by Nwachukwu et al 16 nor other reports on LPD described any evidence on the incidence of osteochondral lesions in recurrent dislocations in children and adolescents. All previous studies focused on surgical techniques, the risk of redislocations, and functional results.
In our cohort, 45% of the knees that were surgically treated because of recurrent LPDs had additional chondral and osteochondral lesions and 37% of all lesions were grade 3 and 4 lesions (Outerbridge classification) with accordingly high therapeutic consequences. Pediatric orthopaedic surgeons should be aware of these high rates of chondral lesions, and the knowledge of concomitant chondral lesions is essential for making appropriate therapeutic decisions. 1,4,7
Chondral Lesions in Adults
During dislocation, the articular surface of the patella is exposed to abnormal shear forces and pressure. 21 There is strong evidence that these forces can lead to chondropathy and degenerative disease over time, probably due to chronic instability. 9,21 Although damage of the inferomedial patella in the case of LPD has long been known as a typical injury after acute patellar dislocation, little attention has been paid to the rest of the patellar surface, the lateral femoral condyle, and the trochlea. 19
Studies focusing on chondral lesions and especially chondromalacia focused on older patient populations and were therefore not comparable with our study. Vollnberg et al 20 analyzed MRIs of 129 knees among 125 patients after acute, recurrent, and chronic LPD and identified cartilage defects in nearly 80% of all cases, of which 75% had central patellar dome lesions. More than 50% had at least mild or moderate osteoarthritis of the FPJ. Mean age in Vollnberg et al's cohort was 26 years with a range up to 56 years and the time interval between patellar dislocation and MRI diagnosis was not mentioned. 20 With 45% of lesions in patients with recurrent dislocations in our cohort, approximately 35% fewer lesions were detected compared to the cohort Vollnberg et al`s study. All of our lesions were located at the medial rim of the patella and the lateral femoral condyle and not in the central patellar dome. Owing to variation in settings, especially the age of patients and long-lasting shear forces, the study by Vollnberg et al is not comparable with our cohort.
Another radiologic study by Elias et al 7 based on MRI analysis documented lesions of the lateral femoral condyle in 80% and lesions of the medial patella in 61% of all cases, with intra-articular loose bodies in 15%. 7 The time period between patellar dislocation and MRI was not mentioned, and the mean age of patients was 20 years with a wide range of 9 to 57 years. The patients in our study had a mean age of 13.0 ± 2.1 years (range, 5-17 years) and the time period between the latest dislocation and surgery was a maximum of 10 weeks (a maximum of 6 weeks between the latest dislocation and presentation to our clinic and ≤4 weeks between presentation and surgery), so a direct correlation between LPD and cartilage defect in a homogeneous cohort was likely.
Nomura and Inoue 15 found a high prevalence of cartilage lesions of the patella in 96% of participants in cases of chronic LPD treated arthroscopically. The age of the patients was <40 years, the mean age was 22 years (range, 13-40 years), and the time between initial dislocation and arthroscopy was a mean of 8 years with a wide range of 0.5 to 30 years without a control group of patients, so any correlation between LPD and patellar cartilage lesions is questionable.
Our study shows a significantly higher likelihood for lesions in surgically treated adolescents with a BMI ≥25, male sex, and physeal closure, as well as in traumatic LPD. The reason for these findings might be that obese children and adolescents may have muscle weakness as a result of less physical activity. 4 Muscles play a shock-absorbing role during joint function and are crucial for knee joint stability. 4 Muscle weakness reduces joint stability. Increased body weight affects weight-bearing joints differently, depending on their anatomical configuration. The knee joint is a hinge joint, and surrounding tissues counteract large shearing, compressive, and axial loading forces. Any dysfunction in these surrounding tissues may cause increased stress on the joint. 4 D’Ambrosi et al 6 found a positive linear correlation between BMI and lesion size of symptomatic osteochondral lesions of the talus and hypothesized that there might be a correlation between the incidence of osteochondral lesions and obesity. In addition, Nakagawa and Maeda 14 observed that knee flexor muscle weakness was associated with joint malalignment and that quadriceps weakness was also associated with significantly higher levels of joint loading during gait. 4 Uimonen et al 19 found a difference by sex in location but not in risk for osteochondral fractures. This contrasts with our findings in which we found a significantly higher risk for chondral lesions associated with male sex.
In particular, in the population of obese male patients with closed physis, we recommend early MRI and consideration of surgical treatment after primary dislocation. Waiting for physeal closure before surgical treatment is not recommended from our point of view. We hypothesize that shear forces in traumatic LPD are higher than in nontraumatic LPD and therefore femoral and patellar lesions are more common. After traumatic LPD a timely MRI should be initiated and the indication for surgery should be made generously.
In the group of 12 children (16 knees) with congenital syndromes and hyperlaxity, no chondral or osteochondral lesions were detected, although each of these patients had ≥20 LPDs or chronic dislocations. The reason might be the lower shear forces and low contact pressure on the FPJ in the moment of dislocation because of the hyperlaxity associated with the syndromes.
A preoperative MRI often requiring anesthesia in these patients and a diagnostic arthroscopy as part of surgery are not the standard of care in children and adolescents with these syndromes in our clinic.
Limitations
The present study is based on retrospective data without a control group. This study is limited by the fact that all chondral injuries were only assessed in surgically treated patients. Hyperlaxity (eg, Beighton score) was not evaluated. Pathologic TT-TG distance, trochlear dysplasia, and a pathological Insall-Salvati index may influence the appearance of cartilaginous lesions. This must be investigated in further studies, as we decided to focus on parameters that can be measured on initial presentation in order to evaluate potential lesions and to initiate a timely MRI.
Conclusion
The likelihood for femoral chondral and osteochondral lesions in surgically treated children and adolescents after LPD was significantly associated with a BMI ≥25, male sex, and physeal closure in our cohort. In case of traumatic LPD, the likelihood for patellar and for femoral chondral and osteochondral lesions was significantly higher. Therefore, we recommend that all obese adolescents, as well as all male patients, patients with physeal closure, and adolescents after traumatic LPD, have an MRI; furthermore, early surgical treatment should be considered. With 45% of chondral and osteochondral lesions in adolescents with recurrent LPDs, the pediatric orthopaedic surgeon should be aware of these lesions.
Footnotes
Final revision submitted July 6, 2022; accepted August 12, 2022.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Ethik-Kommission der Ärztekammer Hamburg (ref No. WF-169-20).