
Abstract
Background:
The changes in glenohumeral joint stability after surgery in a clinical setting are yet unknown.
Purpose/Hypothesis:
This study aimed to compare the anterior humeral head translation between pre- and postsurgical conditions using ultrasonography. It was hypothesized that ultrasonographic assessment would reveal decreased anterior translation.
Study Design:
Case series; Level of evidence, 4.
Methods:
A total of 27 patients (24 male, 3 female; mean age, 24.1 ± 9.7 years) with anterior shoulder instability were studied prospectively. All the patients underwent the arthroscopic Bankart-Bristow procedure under general anesthesia, and ultrasonographic evaluation was performed before and immediately after surgery. The forearm was fixed with an arm positioner in the beach-chair position, and the ultrasonographic transducer was located at the posterior part of the shoulder to visualize the humeral head and glenoid rim at the level of interval between the infraspinatus tendon and teres minor tendon. The upper arm was drawn anteriorly with a 40-N force at 0°, 45°, and 90° of shoulder abduction with neutral rotation. The distance from the posterior edge of the glenoid to that of the humeral head was measured using ultrasonography with and without anterior force. Anterior translation was defined by subtracting the distance with anterior force from the distance without anterior force.
Results:
The humeral head position was translated posteriorly immediately after surgery in all patients. Anterior translation decreased significantly after surgery at 45° (7.7 ± 4.3 vs 5.8 ± 2.0 mm; P = .031) and 90° (8.9 ± 3.4 vs 6.1 ± 2.2 mm; P < .001) of abduction, whereas there was no difference between pre- and postsurgical translation at 0° of abduction (4.9 ± 2.3 vs 4.0 ± 2.1 mm, P = .089).
Conclusion:
Ultrasonographic assessment immediately after a Bankart-Bristow procedure showed the humeral head was translated posteriorly relative to the glenoid at 0°, 45°, and 90° of abduction. The surgery also decreased anterior translation in response to an anteriorly directed force at 45° and 90° of abduction.
Anterior shoulder instability is common in young athletes, particularly in those participating in collision sports. 2,19 Patients with anterior shoulder instability have been known to have excessive anterior translation of the humeral head, 20 which could provoke pain and anxiety related to dislocation and/or recurrent dislocation. A surgical procedure is often needed to enable these patients to continue sports activity. 18,28 Surgery for anterior shoulder instability seems to be effective in suppressing anterior translation of the humeral head, as a previous cadaveric study has shown that Bankart repair restored excessive anterior translation to its previous status (before creating the Bankart lesion). 14 However, in a clinical setting, the extent of change in the anterior translation after surgery remains unclear. This is because assessments of the anterior translation are generally conducted by means of nonquantitative methods, using manual examination, such as the load and shift test, anterior drawer test, apprehension test, or relocation test. 16,25
To evaluate joint stability quantitatively, several techniques have been reported, including stress radiography, electromagnetic tracking systems, ultrasonography, reconstructed 3-dimensional magnetic resonance imaging, and 4-dimensional computed tomography. 11,15,20,21,23,26 In a relatively small case series (n = 11) of patients with shoulder instability, Peltz et al 21 investigated the center of the humeral head against the glenoid using a computed tomographic model–based tracking technique on biplane radiographic images; they reported that the center of the humeral head was located more anteriorly in patients with glenohumeral instability than in those with intact shoulders at 90° of shoulder abduction and that it moved posteriorly at 6 months after surgery.
Ultrasonography has the advantage of enabling an easy, noninvasive, and dynamic assessment of musculoskeletal tissues. Moreover, sonographic assessments can be performed repeatedly without requiring radiation exposure. Assessment of translation of the humeral head using ultrasonography has been reported by several authors since Jerosch et al 8 first reported this method. 5,8,23 The development of ultrasonographic technology can provide examiners with clear images of the structures around the joint, which makes it possible to assess translation of the humeral head with high reproducibility. 23 Quantitative assessment of anterior translation of the humeral head with ultrasound after surgery also makes it possible to understand changes in glenohumeral joint instability after surgery.
In this study, we aimed to use ultrasonography to compare pre- versus postsurgical translation in patients who underwent the Bankart-Bristow procedure for anterior shoulder instability. We hypothesized that anterior translation would be decreased after surgery.
Methods
The protocol for this study received ethics committee approval. A total of 27 shoulders in 27 patients who were scheduled for an arthroscopic Bankart-Bristow procedure for traumatic anterior shoulder instability at a single institution specializing in arthroscopy and sports medicine were prospectively included in this study. Patients with osteoarthritis of the glenohumeral joint, multiple directional instability, or unstable painful shoulders and those who were unaware of apparent dislocation were excluded. Informed consent was obtained from all patients.
The ultrasonographic measurements were performed by a single surgeon (A.T.) with over 20 years’ experience in arthroscopic surgery and ultrasonographic examination, and the surgery was performed by the same surgeon. The arthroscopic Bankart-Bristow procedure was selected for patients with greater than 20% glenoid defect, off-track bipolar bone loss, a history of failed surgery, or participation in collision sports.
Surgical Methods
All surgeries were performed with the patients in the beach-chair position, under general anesthesia, and with an interscalene block using 10 mL of 0.25% levobupivacaine. Five portals (posterior, anterior, anterolateral, immediately above the coracoid, anteromedial transpectoralis major muscle) were used. The anteroinferior labrum complex was detached from the glenoid rim at the 6-o’clock position. The anterior 3 mm of the articular cartilage was removed, and the anterior surface of the glenoid was flattened. The coracohumeral and pectoralis minor tendons were detached from the coracoid. The coracoid process was cut with an oscillating saw and extracted immediately above the coracoid portal. The coracoid process was formed into a length of 10 mm from the tip. A 3.75-mm cannulated cancellous screw with a washer was inserted into the coracoid process and placed within the portal. The subscapularis tendon was split parallel to the direction of the fibers at the 3:30 clockface position on the right shoulder (8:30 clockface position on the left shoulder). A guide pin was inserted into the glenoid from the anteromedial transpectoralis major muscle portal, followed by drilling. The screw in the coracoid and the guide pin were connected arthroscopically, and the screw was inserted into the glenoid. The coracoid block was placed flush with the glenoid articular surface. Finally, the anteroinferior labrum complex was repaired with 4 anchors, placed from the 5-o’clock to the 2-o’clock position on the right shoulder (7-o’clock to 10-o’clock position on the left shoulder).
Ultrasonographic Measurement
Ultrasonographic measurements were performed immediately after administering general anesthesia and an interscalene block (presurgical). In addition, the same procedure was repeated immediately after completing surgery (postsurgical). The patient was positioned on the bed, flexed at 45°, with the forearm fixed using an arm positioner (Trimano Fortis; Arthrex), which was connected to the bed; the shoulder was placed in 0° of flexion and neutral rotation; and the elbow was placed in 90° of flexion and neutral rotation. All sonographic procedures were performed with an ultrasound machine (Sonimage HS1; Konica Minolta) with an 11- to 3-MHz linear array transducer. To visualize the glenohumeral joint at the level of the interval between the infraspinatus and the teres minor, a transducer was set parallel to the craniocaudal axis to visualize the short axis of the infraspinatus and the teres minor, and the transducer was rotated approximately 90° at the interval of the 2 muscles, parallel to the scapular spine (Figure 1A). Consequently, the posterior edge of the glenoid and the humeral head was visualized (Figure 1B). With 1 examiner keeping the transducer at the same position, another examiner translated the humerus anteriorly with a 40-N force, measured using a dynamometer (Ergo FET; Nihon Medic Co). The traction band was set at the proximal third of the upper arm (Figure 2).

(A) Location of the transducer for visualizing the glenohumeral joint at the level of the interval between the infraspinatus and the teres minor (right shoulder). (B) Ultrasonographic image with a view of the posterior edge of the glenoid and that of the humeral head.

Examination for anterior translation of the humeral head. While 1 examiner kept the transducer at the same position, another examiner distracted the humerus anteriorly with a 40-N force using a dynamometer.
Ultrasound images were recorded with and without the anteriorly directed force. The examination was performed at 0°, 45°, and 90° of shoulder abduction with neutral rotation. Once an examination had been performed with anterior translation, a compression force was applied manually to the humeral head to reduce the humeral head at the center of the glenoid.
To calculate the inter- and intraobserver reliabilities for the position of the posterior part of the humeral head against that of the glenoid, the presurgical measurement was performed at 0° of shoulder abduction by 2 observers (A.T., N.O.) and repeated by 1 of the observers (A.T.) in the first 16 patients.
The preserved sonographic images were transferred to picture archiving and communication systems (RapideyeCore; Canon Medical Systems) and were analyzed by another orthopedic surgeon (J.I.), who was blinded to the measurements taken during the surgery and the examination. To measure distance, 2 lines were drawn parallel to the posterior edge of the glenoid and humeral head. The shortest distance between the 2 lines was measured without (D1) and with 40-N distraction (D2). Negative values were assigned when the posterior edge of the humeral head was anterior to that of the glenoid. Anterior translation of the humeral head was defined by subtracting D2 from D1 (Figure 3).

Ultrasonographic images (A) without distraction and (B) with 40-N distraction. Two parallel lines were drawn through the posterior edges of G and HH. The shortest distance between the 2 lines was measured both without (D1) and with (D2) 40-N distraction. Anterior HH translation was calculated by subtracting D2 from D1. HH, humeral head; G, glenoid.
Statistical Analysis
The distance from the posterior edge of the glenoid to that of the humeral head without any applied force and with the anterior force applied was compared pre- and postsurgically using a paired t test. Statistical significance was set at P < .05. All statistical analyses were performed using SPSS Version 21.0 software (IBM).
The inter- and intraobserver reliabilities for humeral head position measurements were calculated using the intraclass correlation coefficient (ICC). ICC values were interpreted as follows: <0.50, poor agreement; 0.50 to 0.75, moderate; 0.76 to 0.90, good; and >0.90, excellent. 10
Statistical power was calculated with G* Power Version 3.1.9 (Heinrich Heine University) to determine the required sample size for identifying the changes in translation from before to after surgery. At least 21 cases were needed to achieve a power of 0.80, with an effect size of 0.66, which was determined according to the results of the primary cases, and significance (α) was set at .05.
Results
Of 27 patients (mean age, 24.1 ± 9.7 years), 24 were male and 3 were female. The mean height was 168.0 ± 6.5 cm, mean weight was 68.9 ± 9.6 kg and mean body mass index was 24.3 ± 2.7. The mean number of dislocations or subluxations was 15.3 ± 18.3. The mean duration of symptoms was 5.2 ± 6.4 years. Five patients had a failed previous surgery. A complete description of the patient characteristics is summarized in Table 1.
Patient Characteristics a

a Data are reported as mean ± SD (range) or No. (%) of shoulders.
The inter- and intraobserver reliabilities for measurement of the humeral head position were 0.912 (95% CI, 0.828-0.956) and 0.952 (95% CI, 0.904-0.976), respectively, indicating excellent agreement. Before surgery, the posterior aspect of the humeral head was located at a mean 6.4 ± 2.1 mm posterior to the posterior edge of the glenoid at 0° of abduction, 5.4 ± 2.2 mm at 45° of abduction and 4.2 ± 2.0 mm at 90° of abduction. After surgery, the humeral head was posteriorly translated 3.1 mm at 0° of abduction (P < .001), 3.2 mm at 45° of abduction (P < .001), and 3.3 mm at 90° of abduction (P < .001) (Figure 4).
Comparison of pre- and postsurgical location of the posterior aspect of the humeral head relative to the posterior edge of the glenoid without any applied force. Positive values represent the posterior direction. Error bars represent SD. The distance increased significantly after surgery at 0°, 45°, and 90° of shoulder abduction (**P < .01).
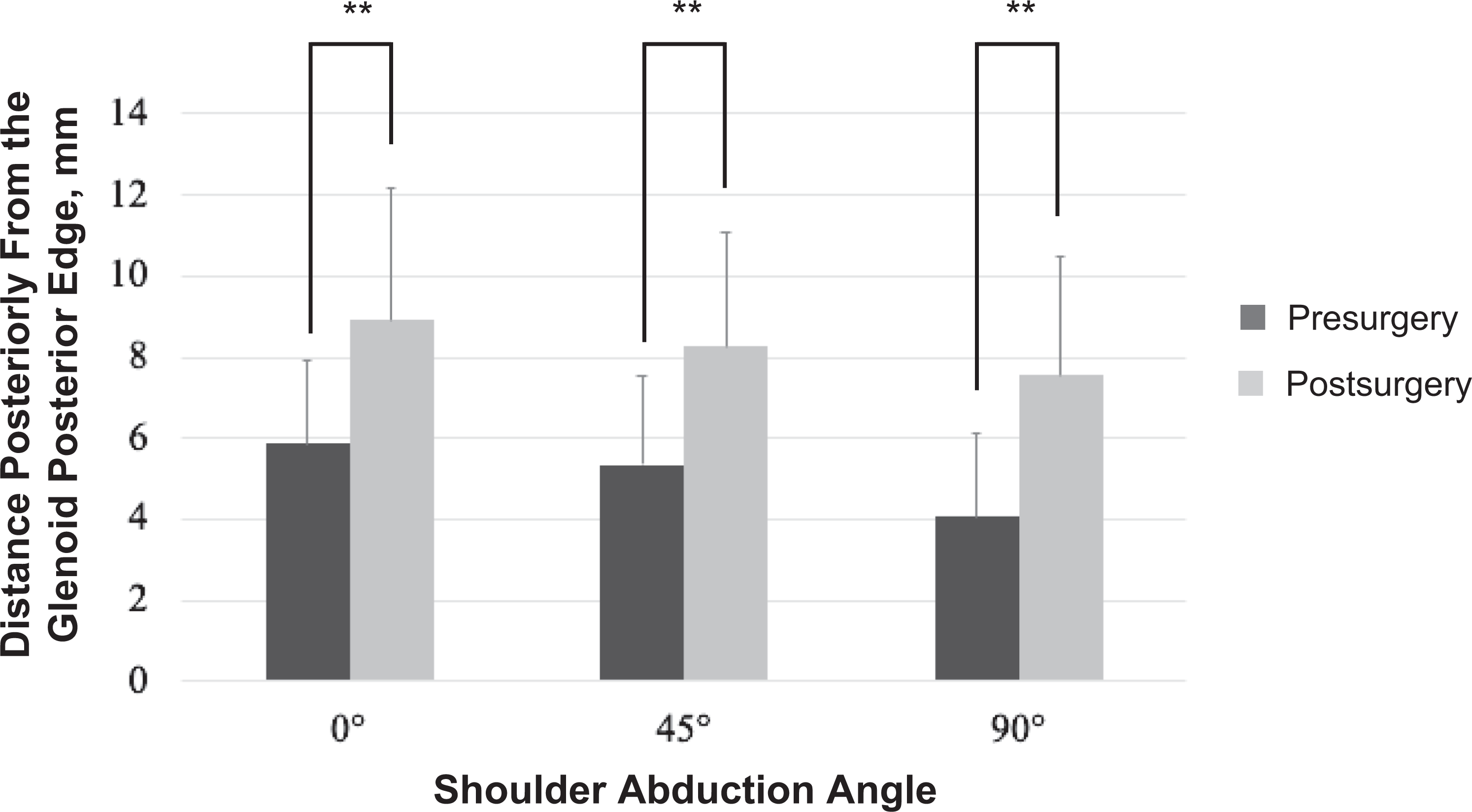
The mean translation after application of the anterior force decreased by 0.9 mm after surgery from 4.9 ± 2.3 to 4.0 ± 2.1 mm at 0° of abduction; however, this change was not statistically significant (P = .089). However, the mean translation decreased significantly by 1.9 mm after surgery, from 7.7 ± 4.3 to 5.8 ± 2.0 mm (P = .031) at 45° of abduction, and by 2.8 mm, from 8.9 ± 3.4 to 6.1 ± 2.2 mm (P < .001), at 90° of abduction (Figure 5).

The pre- and postsurgical anterior translation of the humeral head with an applied 40-N anterior force. Error bars represent SD. Anterior translation decreased significantly after surgery at 45° (*P < .05) and 90° (**P < .01) of abduction.
Discussion
The findings of the present study revealed that surgery had 2 significant effects on anterior shoulder instability: there was a postsurgical posterior shift of the humeral head without any applied force and a decrease in anterior translation with anteriorly directed force, compared with the presurgical condition. Anterior translation of the humeral head was suppressed significantly at 45° and 90° of abduction after surgery; however, there was no significant difference at 0° of abduction. With no force applied, the humeral head moved posteriorly relative to the glenoid at 0°, 45°, and 90° of abduction after surgery.
It has been reported that the center of the humeral head is located anteriorly in anterior shoulder instability 9,26 and that the pathological position of the humeral head could be a cause of discomfort, anxiety, and/or a painful shoulder. 4,13 A previous study using 3- and 2-dimensional model image registration techniques showed that the center of the humeral head was located 2.3 mm more anteriorly in cases of traumatic anterior shoulder instability at 20° of shoulder abduction with neutral rotation than in the contralateral side. 9 Another study using magnetic resonance imaging showed that the center of the humeral head was located 1.5 mm more anteriorly in traumatic anterior shoulder instability, at 90° of shoulder abduction with neutral rotation, than on the contralateral side. 26 In addition, various studies have investigated the humeral head position several months after surgery. Peltz et al 21 reported that the center of the humeral head was positioned 2.1 mm more anteriorly, at 90° of shoulder abduction with external rotation, in patients with anterior shoulder instability than in healthy control patients and that this displacement was reduced to only 1.1 mm more posteriorly at 6 months after arthroscopic Bankart repair than in the presurgical condition. Moreover, Lädermann et al 11 mentioned that the anterior shift of the humeral head was not normalized at 1 year after the Latarjet procedure. In the present study, the humeral head, without distraction, moved approximately 3 mm posteriorly immediately after surgery, at 0°, 45°, and 90° of abduction. This finding seemed to reflect the postsurgical posterior shift of the center of the humeral head relative to the glenoid. This would result from a repaired anterior capsulolabral complex or transferred conjoint tendon, pushing the humeral head posteriorly.
Some cadaveric studies have investigated the surgical effect on anterior translation of the humeral head. 1,3,14,22 Marquardt et al 14 reported that anterior translation was decreased at both 0° and 90° of glenohumeral abduction with external rotation after Bankart repair (by 2.7 mm at 0° and 2.9 mm at 90°). Black et al 3 investigated the change in anterior translation after Bankart repair, at 0°, 45°, and 90° of glenohumeral abduction with neutral rotation, and reported that the surgical effect was greatest at 90° and smallest at 0° (0.9 mm at 0°, 2.9 mm at 45°, and 3.4 mm at 90°); our findings were consistent with their results.
The anterior inferior glenohumeral ligament (AIGHL) is known to work at 90° of abduction with external rotation 6 ; however, previous studies showed that AIGHL had an important function not only in external rotation but also in neutral rotation. 7,17 Debski et al 7 measured the in situ force in each glenohumeral ligament at different angles of glenohumeral joint abduction with neutral rotation when anterior load was applied to the glenohumeral joint; AIGHL had the highest force at 90° of abduction during anterior translation. O’Brien et al 17 also reported that the primary stabilizer was AIGHL at 90° of glenohumeral joint abduction in neutral rotation. In the current study, the decrease in anterior translation was greatest at 90° of shoulder abduction after surgery. This result might reflect the recovered function of the AIGHL, which worked as a significant restraint for anterior translation at 90° of shoulder abduction. 7,17 Meanwhile, the sling effect of the coracoid transfer could also contribute to the result, as it was reported to affect anterior translation at 90° of shoulder abduction both in external rotation and in neutral rotation. 27 Abdulian et al 1 also reported that a modified Bristow procedure restored anterior-inferior translation nearly to the level of intact condition and additional Bankart repair did not significantly decrease translation. Considering these cadaveric studies, in the current study, it was unknown which procedure, Bankart repair or Bristow procedure, contributed most to suppress anterior translation.
Marquardt et al 14 also investigated posterior translation of the humeral head after Bankart repair when the humeral head was distracted posteriorly and reported a decrease in posterior translation of the humeral head (2.7 mm at 0°, 2.1 mm at 90°). Considering the finding in the present study that the humeral head shifted posteriorly after surgery (3.1 mm at 0°, 3.2 mm at 45°, 3.3 mm at 90°), the decrease in posterior translation may have occurred due to the posterior shift of the humeral head at the starting position. Two crucial surgical effects should be considered when glenohumeral instability is assessed after surgery: the posterior shift of the humeral head without distraction and decrease of anterior translation with anteriorly directed force. Ultrasonographic examination could be used to assess whether the surgery was properly performed; however, future research should assess the relationship between the magnitude of postsurgical translation and clinical outcomes to investigate the proper postsurgical anterior translation.
Limitations
This study had some limitations. First, the contralateral side was not examined in the current study. Consequently, the normal values for anterior translation or positional relationship between the humeral head and the glenoid were not identified. It is also unknown whether the surgery is “overtightening” the shoulder. Second, the shoulder was looked at only immediately after surgery. With capsular healing there may be changes in the amount of posterior translation at rest, which could result in decreased laxity (and predispose to capsulorrhaphy arthropathy) or recurrent laxity (with recurrence of symptoms). Third, outcomes of the patients were not investigated in the current study. Therefore, it is unknown whether outcomes correlated with the amount of posterior translation that occurred. Fourth, the applied anterior force on the humeral head may vary according to the condition or thickness of the soft tissue, since the force was applied through a strap around the patient’s arm. Fifth, the examination was not performed at the end-range position (in external rotation) but only at the midrange position (in neutral rotation) although the difference of these positions could affect the results due to the different stabilizing mechanisms. 12,24,27 However, if anterior force was applied to the externally rotated shoulder immediately after surgery, there was a risk of applying a large stress to the surgically repaired site. Finally, the accuracy of our methods of the ultrasonographic measurements was not investigated. A previous cadaveric study reported that anterior translation obtained using ultrasonography was significantly smaller than that obtained using the motion tracking system when the ultrasonographic probe was set from the anterior shoulder. 23
Conclusion
Ultrasonographic assessment immediately after a Bankart-Bristow procedure showed the humeral head was translated posteriorly relative to the glenoid at 0°, 45°, and 90° of abduction. The surgery also decreased anterior translation in response to an anteriorly directed force at 45° and 90° of abduction.
Footnotes
Acknowledgment
The authors thank the staff of the Department of Orthopedic Surgery, Meitetsu Hospital, for supporting this study.
Final revision submitted August 1, 2022; accepted August 10, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.Y. belongs to an affiliation supported with research grants from Zimmer Biomet, Stryker Japan, and PRO Medical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Meitetsu Hospital (ref No. 238).